Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Createmedic.co.jp
CLINY Ileus Tube - 1/8 Univ. Professor Dr. med. Jakob R. Izbicki, FACS Direktor der Klinik und Poliklinik für Allgemein,- Viszeral- und Thoraxchirurgie Martinistraße 52 20246 Hamburg Universitätsklinikum Hamburg-Eppendorf Martinistraße 52 20246 Hamburg Medical reports on clinical uses of CLINY Ileus Tube
1 A 66 year old male patient who was treated with a CLINY Ileus Tube
The patient was hospitalized from May 22nd, 2003 to June 16th, 2003 in our Department of
Diagnoses:
1. Recurrence of ileus caused by abdominal adhesions
2. Condition of site where appendectomy was performed 40 years ago
3. Condition of site where ileus operation of partial resection of the colon was performed
Our treatment policy:
3. Intra-operative splinting of small bowel with CLINY Ileus Tube
Epicrisis:
A 66 year old male patient with an adhesion ileus came in our emergency admission.
Appendectomy was performed to the patient more than 40 years ago. Ileus operation was
also performed 20 years ago. In recent years he had signs of recurrent ileus which made
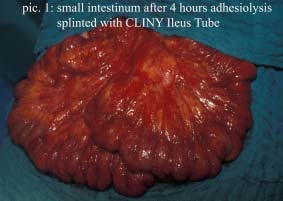
clinical treatment necessary. In a 4 hours operation, we did an extensive enterolysis and a
partial resection of the small bowel. During the operation, no-torsion of the duodenum was
diagnosed. In operation, CLINY Ileus Tube was inserted trans-nasally by anesthesiologist
and it was pushed further up to the cecum with surgical assistance. Aspiration was made
during the insertion. The balloon of the CLINY Ileus Tube was inflated with 25ml distilled
water for blocking the inner cecum (picture 1). The splinted bowel by CLINY Ileus Tube was
repositioned in the abdomen with a Noble’s like procedure.
CLINY Ileus Tube - 2/8 Univ. Professor Dr. med. Jakob R. Izbicki, FACS Direktor der Klinik und Poliklinik für Allgemein,- Viszeral- und Thoraxchirurgie Martinistraße 52 20246 Hamburg Universitätsklinikum Hamburg-Eppendorf Martinistraße 52 20246 Hamburg
When the tube was left 70cm in the patient,
In a postoperative process the patient had
singultus on first day. And he was not able
In the following days the patient could be
discharged as a regular intestinal passage
CLINY Ileus Tube - 3/8 Univ. Professor Dr. med. Jakob R. Izbicki, FACS Direktor der Klinik und Poliklinik für Allgemein,- Viszeral- und Thoraxchirurgie Martinistraße 52 20246 Hamburg Universitätsklinikum Hamburg-Eppendorf Martinistraße 52 20246 Hamburg
2 A 67 years old man who was treated with a CLINY Ileus Tube
The patient was treated from 21st of December, 2003 to 13th of January, 2004 by our Surgical
Diagnoses:
1. Advanced mechanical ileus by incarcerated jejunum and resulted paralysis of the
2. Haemorrhagic erosive enterocolitis with gastrointestinal bleeding
3. Situation of 6 days after kidney transplantation
4. Situation after terminal renal insufficiency due to an IgA-nephritis and a diabetic
Our treatment policy:
1. Explorative laparotomy with reposition of the incarcerated small bowel loop
2. Aspiration and splinting of the small bowel with CLINY Ileus Tube
Verlauf:
A 67 years old male patient had developed the clinical signs of a paralytic ileus on the 6th
postoperative day after kidney transplantation with terminal renal insufficiency due to an IgA-
nephritis and diabetic nephropathia during his stay at the intensive-care-unit. In the following
explorative relaparotomy, 5cm dehiscence of the fascia and the peritoneum with an
incarceration of jejunal loop itself was confirmed as the reason for his symptoms. A paralysis
of the whole small bowel was demonstrated. After reposition of the bowel by surgeon, a
transnasal insertion of the Cliny Ileus Tube with its guidewire was undone by the
anesthesiologist. The CLINY Ileus Tube was pushed into the cecum after passing the
stomach, duodenum and the rest of the small bowel by surgical assistance and the balloon of
CLINY Ileus tube was inflated with 25ml distilled water for blocking the inner cecum. After
CLINY Ileus Tube - 4/8 Univ. Professor Dr. med. Jakob R. Izbicki, FACS Direktor der Klinik und Poliklinik für Allgemein,- Viszeral- und Thoraxchirurgie Martinistraße 52 20246 Hamburg Universitätsklinikum Hamburg-Eppendorf Martinistraße 52 20246 Hamburg
emptying the small bowel by aspirating with the CLINY Ileus Tube, Noble’s procedure was
made to the splinted small bowel, and then repositioned in the abdomen.
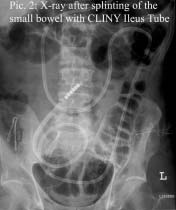
24 hours later the blocking with balloon was released and abdominal X-ray photo was taken
after insertion of the CLINY Ileus Tube, an
upper gastrointestinal bleeding was found,
gastrointestinal blood, the patient got first
and finally in a further relaparotomy, a
hemorrhagic erosive enterocolitis caused by CMV. In the whole time, the patient stayed at
the intensive-care-unit and got parenteral feeding. Immunological suppressed patient died in
CLINY Ileus Tube - 5/8 Univ. Professor Dr. med. Jakob R. Izbicki, FACS Direktor der Klinik und Poliklinik für Allgemein,- Viszeral- und Thoraxchirurgie Martinistraße 52 20246 Hamburg Universitätsklinikum Hamburg-Eppendorf Martinistraße 52 20246 Hamburg
3A 64 year old male patient who was treated with a CLINY Ileus Tube
The patient was hospitalized from February 20th, 2004 to March 2nd, 2004 in our Department
Diagnoses:
1. Incarcerated hernia of small bowel with fused bowels
2. Situation after resection of the sigmoid
Our treatment policy:
1. Complete adhesiolysis with explorative laparotomy
2. Relief and splinting of the small bowel with CINY Ileus Tube during operation
3. Plastic closure of the abdominal wall
Epicrisis:
The 64 years old man came to us with colic-like pain of the bowel, nausea and vomit. He told
us that there had been no defecation for 4 days. In the clinical examination the patient had
significant meteorism. We further examined and found that a resection of the sigmoid was
A conventional radiograph of the bowel showed an ileus of the small bowel with several
endoluminal surfaces. In a radiopaque-enhanced CT we saw distended, obstructed bowels
of the small bowel with surfaces which matches a situation of an ileus. No tumor was seen,
which could be blamed to cause the ileus. On February 20th, 2004 we performed an
explorative laparotomy. It showed a hernia with an incarcerated loop of jejunum and a
chronically inflammatory gallbladder. We repositioned the hernia and performed a plastic
closure of its laparotomic site. Afterwards the gallbladder was resected and a complete
adhesiolysis of the bowel was made. Finally the anesthesiologist insert the CLINY Ileus Tube
with a guidewire transnasally until the terminal ileum through the stomach, duodenum and
CLINY Ileus Tube - 6/8 Univ. Professor Dr. med. Jakob R. Izbicki, FACS Direktor der Klinik und Poliklinik für Allgemein,- Viszeral- und Thoraxchirurgie Martinistraße 52 20246 Hamburg Universitätsklinikum Hamburg-Eppendorf Martinistraße 52 20246 Hamburg
small bowel by surgical assistance. The balloon of the CLINY Ileus Tube was inflated with
25ml distilled water for 12 hours in order to block the inner bowel. An antibiotic treatment with
Cefazolin and Metronidazol was performed and the patient was moved to normal ward. The
duration of the operation was about 2 hours.
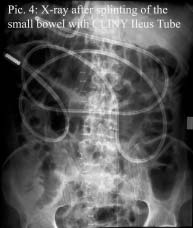
The post operative healing process was uncomplicated. On the 1st postoperative day, a
conventional radiograph of the bowel was performed to make sure the CLINY Ileus Tube was
After that, blocking with balloon was released on
the same day. From the 4th postoperative day,
the tube was extracted by 20 to 30cm every day.
And it was completely removed on the 8th day.
The patient tolerated enteral nutrition without
complications. On the 10th postoperative day we
discharged the patient in a good general status
of health and with a regular intestinal passage.
On the 10th postoperative day we discharged
the patient in a good general status of health
CLINY Ileus Tube - 7/8 Univ. Professor Dr. med. Jakob R. Izbicki, FACS Direktor der Klinik und Poliklinik für Allgemein,- Viszeral- und Thoraxchirurgie Martinistraße 52 20246 Hamburg Universitätsklinikum Hamburg-Eppendorf Martinistraße 52 20246 Hamburg
4 A 6 years old female patient who was treated with CLINY Ileus Tube
The patient was hospitalized from February 20th, 2004 to March 1st, 2004 in our Department
Diagnoses: Our treatment:
1. Laparotomy and explortion of the abdominal cavity
3. Resection of 6 diverticula of the small bowel
4. Intra-operative splinting of the small bowel with a CLINY Ileus Tube
Epicrisis:
A 63 years old female patient was referred to our hospital with clinical signs of an ileus. No
defecation took place for at least 30 hours, but no nausea or vomiting either. An unspecific
pain was described in the right hypogastricum. An appendectomy and a cholecystectomy
were performed several years ago. On the clinical inspection, there was no muscular
defence of the abdominal wall. No fever and no suspect were observed as the results of the
rectal examination or the urine tests. We auscultated reduced peristaltic sounds. A
conventional X-ray of the abdomen showed an ileus of the small bowel with several
In a 3 hours and 20 minutes operation, we performed an extensive adhesiolysis and atypical
resections of 6 small bowel diverticula, which were found accidentally.
CLINY Ileus Tube - 8/8 Univ. Professor Dr. med. Jakob R. Izbicki, FACS Direktor der Klinik und Poliklinik für Allgemein,- Viszeral- und Thoraxchirurgie Martinistraße 52 20246 Hamburg Universitätsklinikum Hamburg-Eppendorf Martinistraße 52 20246 Hamburg
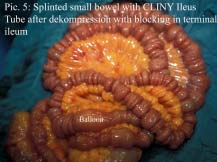
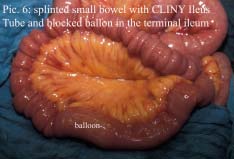
Finally the anethesiologist inserted the CLINY Ileus Tube with a guidewire trans-nasally until
the terminal ileum through the stomach, duodenum and small bowel by surgical assistance.
The balloon of the CLINY Ileus Tube was inflated with 25ml distilled water for 12 hours in
order to block the inner bowel (pictures 5, 6). An antibiotic treatment with Cefazolin and
On the 1st postoperative day the patient was
transferred to the normal ward. To evaluate the
right position of the CLINY Ileus Tube, an X-ray
Afterwards the blocking was released. From the
4th postoperative day, we started the extraction of
the tube by 20 to 30cm every day and the CLINY
Ileus Tube was completely extracted on the 8th
postoperative day. Then any complications did not
occur and we started the enteral nutrition of the
patient. On the 10th postoperative day, we
discharged the patient in a good general status of
health and with a regular intestinal passage.
Steven L. Almany, MD, FACC William W. O'Neill, MD, FACC To be honest, I was extremely skeptical of using the radial artery as an access site for procedures. William O'Neill, MD, FACC, Director of Cardiovascular Diseases at William Beaumont Hospital in Royal Oak, Michigan, suggested I spend time looking into this as he believed (and he was right) that this would be a new trend in Intervent
 CLINY Ileus Tube - 1/8
CLINY Ileus Tube - 1/8 
 CLINY Ileus Tube - 2/8
CLINY Ileus Tube - 2/8  CLINY Ileus Tube - 3/8
CLINY Ileus Tube - 3/8 
 CLINY Ileus Tube - 4/8
CLINY Ileus Tube - 4/8  CLINY Ileus Tube - 5/8
CLINY Ileus Tube - 5/8 
 CLINY Ileus Tube - 6/8
CLINY Ileus Tube - 6/8  CLINY Ileus Tube - 7/8
CLINY Ileus Tube - 7/8 
 CLINY Ileus Tube - 8/8
CLINY Ileus Tube - 8/8