Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Accumed.pdf
Steven L. Almany, MD, FACC William W. O'Neill, MD, FACC
To be honest, I was extremely skeptical of using the radial artery as an access site for procedures. William
O'Neill, MD, FACC, Director of Cardiovascular Diseases at William Beaumont Hospital in Royal Oak, Michigan, suggested I spend time looking into this as he believed (and he was right) that this would be a new trend in Interventional Cardiology. Because of my respect for his foresight in our field, I traveled to Hospital Laval, Quebec City, Canada, to work with Dr. Gerald Barbeau. Dr. Barbeau, considered one of the pioneers in this area, further stimulated my interest and now, some two years later, I am an avid proponent of radial access.
Through subsequent experiences at William Beaumont Hospital, review of the work of leaders in the field, and recent involvement in designing equipment for this type of procedure, this manual was born. Its purpose is hopefully to stimulate the interest of the Cardiologist/Radiologist just as ours was several years ago. In addition, we hope to point out some of the pearls and perils of this type of procedure, making your transition into a radial advocate just a little smoother.
Although I doubt that transradial access will ever replace transfemoral intervention, I do believe that this type of access will have an ever-important role for diagnostic and interventional procedures. It will be driven by cost containment, improvements in equipment, operator experience and, most importantly, patient preference.
Steven L. Almany, MD, FACC William Beaumont Hospital Royal Oak, Michigan
TABLE OF CONTENTS
Page Forward… … … … … … … … … … … … … … … … … … … … … … … … … … … … … … … … … … … .
Background of Transradial Access.… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … . 4
Comparison of Transfemoral and Transradial Access Site… … … .… … … .… … … .… … … .… … … … . 4
Contraindications… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … … … … . 5
Pertinent Anatomy… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … 6
Patient Preparation… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … 7
Cath Lab/Staff Preparation.… … … .… … … .… … … .… … … .… … … .… … … .… … … … … … .… … . 8
Transradial Artery Access… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … . 8
Transradial Medications… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … . 9
Transradial Catheters / Guides… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… 10
Hemostasis Devices… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… . 13
Sheath Removal… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … . 13
Pitfalls of Transradial Intervention … … … .… … … .… … … .… … … .… … … .… … … .… … … .… … . 13
Post Procedural Management… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … … … 14
Accessories … … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… . 15
References… … … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … .… … … … . 17
I. Background of Transradial Access The history of radial artery intervention appears to date back to 1989 when Campeau et al (1) performed 100 catheterizations via this approach. He was successful in 88 of the patients, although an absent or diminished pulse was documented in 22 patients. The first transradial PTCA occurred in Amsterdam (2) followed by the first transradial stent in 1993 (3). This procedure is now widely used in several locations around the world. II. Potential Market for Transradial Intervention With nearly 800,000 interventions and nearly 1.1 million catheterizations being performed in the United States alone (4), the potential market for a different form of diagnostic and interventional access is large. This does not include the non-US market, which is usually regarded as twice as large. In addition, this type of access is certainly applicable in the field of invasive radiology. The benefit of radial access lies in the potentially lower direct costs, patient preference, lower incidence of vascular complications (and their subsequent costs), as well as earlier ambulation. Although percutaneous closure devices do allow earlier ambulation, they are also associated with increased direct costs as well as occasional failure. Collagen devices, although less expensive, often limit access at the same site for weeks or even months.
Despite the advantages, transradial access interventions have grown slowly in the US. This is likely because of physicians' familiarity with the femoral or brachial approach, a lack of 6F compatible equipment, as well as the development of closure devices. However, the development of 6F compatible systems, patient preference, and increasing operator experience seem to suggest that more invasive Cardiologists and Radiologists are willing to learn this procedure.
III. Comparison of Transfemoral and Transradial Access Sites The transfemoral approach for cardiac catheterization and intervention has gained widespread acceptance. Its advantages include:
• Long history of use• Technically easy• Facilitates the use of larger catheters/equipment
It is, however, plagued with some disadvantages that are inherent with this type of access and these include:
• Prolonged bed rest required (usually one hour per sheath size) or use of a closure device (which increases cost) • Femoral access is more commonly associated with back pain, urinary retention, and neuropathy than the radial • 0.5-4.0% incidence of vascular complications including pseudoaneurysm, a-v fistula, transfusions and/or
• Bleeding can be significant (before it is detected clinically)
The radial approach has certain inherent advantages:
• Dual blood supply which limits the potential for limb threatening ischemia• Advantageous for patients with severe occlusive aortoiliac disease
• Advantageous for patients with difficulty laying/lot (back pain, obesity, CHF)• The vessel is easily compressible• Less chance for local nerve injury• Radial approach allows earlier patient ambulation and likely will cost less (closure devices are not necessary)• Vascular complications are less frequent (1, 8-10)• Randomized trials to date suggest patients prefer the radial approach
There are potential disadvantages to a radial approach. We believe that most of these will be diminished with improved equipment and increasing operator experience. They include:
• The radial artery is smaller than the femoral (approximately 2-2.3mm) • Obtaining radial access involves a learning curve • Smaller sheaths are required (4-8F)• Vessel spasm is more common• Guide placement is more challenging and requires learning a different technique• Many physicians are not familiar with the equipment and anatomy, and thus are reluctant to try a new approachIV. Contraindications A radial access approach is not appropriate in all patients. Absolute contraindications would include:
• Patients who have evidence of an abnormal Allen's test (described later). It has beenreported that approximately 10% of the population will have an abnormal Allen's test. (11 -12) The authors, in fact, do not advocate the Allen's test as we feel it is quite subjective and question its reproducibility.
• Patients who display evidence of abnormal oximetry/ plethysmography (described later). We prefer this because it can produce a (legal) record of radial competence and is not as subjective as the Allens' test. In addition the patient can wear a finger oximeter on the hand that is being intervened upon, which will allow for continuous monitoring of not only overall oxygen saturation but also the integrity of the hand's blood supply.• Patients who may require intra-aortic balloon pump counterpulsation (IABP).• Patients who may require devices that are not compatible in 7F or smaller sheaths (TEC, larger Rotoblator burrs,
• Patients with known upper extremity vascular disease. Some patients (less than 5%) will have congenital abnormalities of their upper extremity arterial system (including extreme tortuosity, anomalous take off of the radial artery, or severe atherosclerosis).
• Patients with Buergers Disease, severe Raynauds, or other forms of upper extremity peripheral vascular disease.
• Patients with known internal mammary grafts contralateral to the site of entry. It should be noted, however, that catheters specifically designed for IMA 's through a radial/brachial contralateral approach are available.• Patients in whom the radial artery may be considered as a conduit for coronary artery bypass grafting or for a V. Pertinent Anatomy
The aorta trifurcates into the right subclavian, the left common carotid, and the (right) innominate artery. Although it is easier to learn the radial approach from the left side, as it mimics a transfemoral approach more accurately, a right-sided approach is probably more commonly used because of the current set up in most catheterization labs. The innominate artery becomes the subclavian artery after the right common carotid arises. It then becomes the axillary artery as it passes into the shoulder. As the axillary artery passes into the upper arm it becomes the brachial artery. In most patients the brachial artery divides into the radial and ulnar artery below the elbow. On occasion the radial artery will originate from the upper brachial artery or the axillary artery. It is important for physicians involved in radial access to take the time to review not only the pertinent anatomy associated with this procedure, but also the anatomic variants that can be found. These are described well in most anatomy books.
VI. Brachial Artery The brachial artery courses from the level of the shoulder along the inner and anterior aspect of the upper arm. At its origin it lies medial to the insertion of the humerus and the biceps muscle but as it approaches the level of the elbow it lies more anterior. At the level of the elbow, it lies between the two condyles covered by skin and fascia on the medial aspect of the arm and overlapped by the biceps on the other side. The brachial artery then travels beneath the supinator longus muscle and the pronator radii teres muscle. At this point it divides into the radial and ulnar arteries, which extend from the forearm into the hand. VII. Radial and Ulnar Artery In most patients, the radial artery branches off of the brachial artery just below the level of the elbow crease. At this point, it passes on the lateral margin
of the forearm until it reaches the level of the wrist.
There are a significant number of patients (reported to be up to 12%) that may have an anatomic
variant. The most common involves the radial
artery originating just superior to the elbow, although in a few patients it may originate much higher in the arm. In the majority of patients where the artery originates just below the elbow the
vessel is deep to the body of the supinator longus muscle in the upper part of the forearm. In the mid forearm, down to the level of the wrist, it lies between the tendons of the supinator longus and
At the level of the wrist, the radial artery lies atop of the scaphoid bone, the trapezium and the external lateral ligament. If one tries to cannulate the artery too distal, they will encounter the reticulum and find the artery is diving deep and lateral. In addition, there are smaller superficial branches of the radial artery that exit at this point. It is important therefore to attempt cannulation approximately 2-3cm from the flexion crease of the wrist.
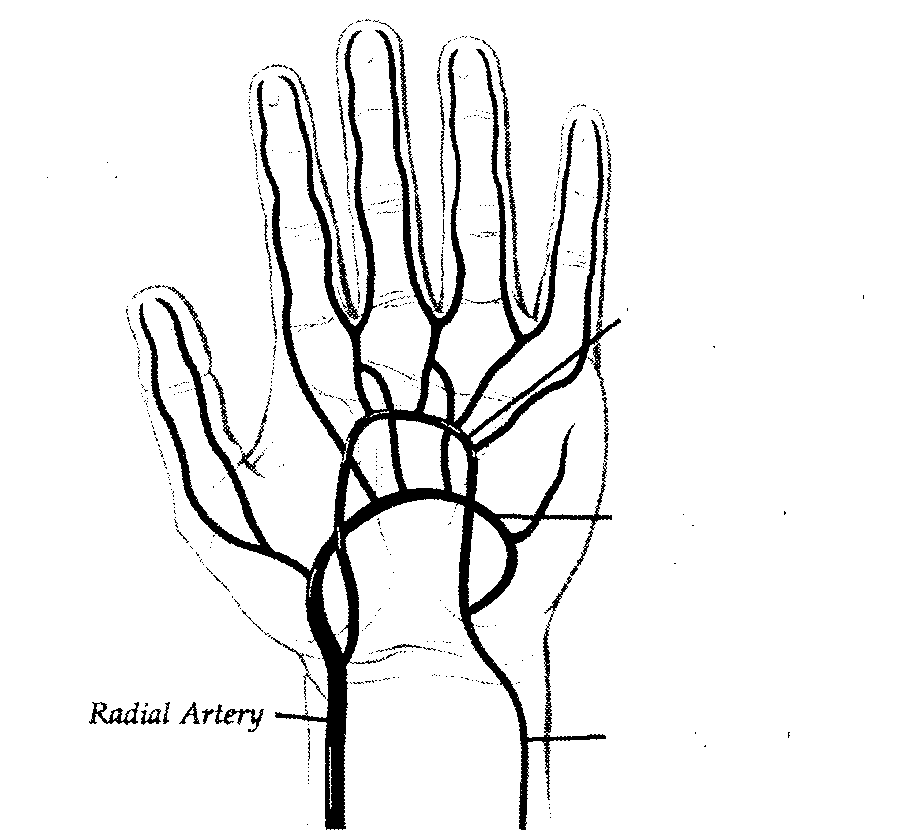
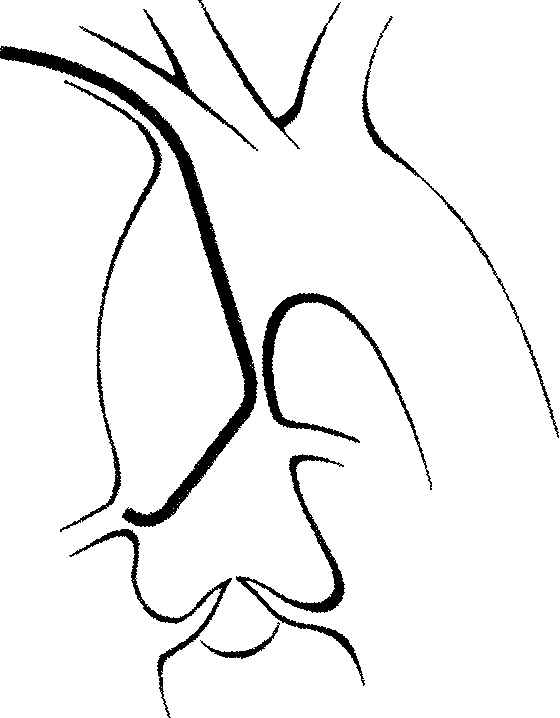
At the level of the hand, the radial artery passes from the space between the metacarpal bones of the thumb and index finger into the palm of the hand. The vessel then crosses the base of the metacarpal bone of the little finger,
where it joins with the deep communicating branch of the ulnar artery and forms the deep palmar arch. The
superficialis branch of the radial artery joins with the palmar portion of the ulnar artery to complete the superficial palmar arch.
The ulnar artery also branches off the brachial artery and passes along the inner aspect of the forearm. At the level of the wrist, it divides into two branches that join the radial artery and its superficial branch to form the deep and superficial palmar arches.
It is not uncommon for a patient to display adequate ulnar and radial pulses, and have abnormal plethysmography (or Allen's test). Whether this represents true radial or ulnar dominance or inadequate/ incomplete palmar circulation (reported in up to 10-23% of patients) (11-12) is difficult to ascertain. Obviously patients who display radial dominance should not be intervened upon from the radial artery. In addition, patients with ulnar dominance would have a higher incidence of radial artery access problems, although this is not well described in the literature.
VIII. Patient Preparation The wrist should be shaved (if necessary) and cleansed in the usual sterile fashion. In addition, the groin should be prepped in case of access failure or the need for urgent IABP or a temporary venous pacemaker. At William Beaumont Hospital, generally, PTCA is performed with the radial artery access site and an adequate peripheral intravenous line. A central venous line is not routinely placed unless rapid volume or temporary pacing will be necessary. We prefer that the IV be started in the contralateral arm so as to allow adequate flow even when a hemostasis device is in place. If an IV must be placed in the arm on the side of the intervention it should be placed proximal to the wrist (preferably at the level of the elbow). All potentially constrictive clothing, jewelry and ID bracelets should be removed prior to the procedure. An Allen's test, or preferably oximetry/plethysmography, should be documented by the physician and/or nursing staff. At William Beaumont Hospital we are currently placing the radial sheath in the holding room, which facilitates cam lab turnaround.
The Allen's Test. (or modified plethysmography), should be documented in every patient undergoing a radial artery procedure. These authors feel that the modified plethysmography allows for more reproducible data and probably serves as a better medical record. To perform the Allen's Test, both the radial and ulnar arteries should be occluded so as to notice obvious pallor of the hand. Pressure on the ulnar artery is then removed (while maintaining pressure on the radial site). An abnormal test occurs when the color of the hand does not return within 8 seconds.
In those patients who require a second procedure through the same radial site it may be helpful to perform a Reverse Allen's Test. In this situation, the physician releases pressure over the radial artery rather than the ulnar. This may detect proximal radial artery disease/occlusion that may be asymptomatic. Patients with an abnormal Reverse Allen's Test should not undergo a repeat transradial procedure from this radial site.
For patients who require the placement of a Swan Ganz catheter or an intravenous temporary pacing wire, we have been placing these in the ipsilateral brachial vein. This access can be achieved in the holding room prior to the case (by placing a 16 gauge IV). This size of IV will allow exchange with a .035 J tipped wire and placement of a sheath.
IX. Cath Lab/Staff Preparation It is important that the catheterization lab staff be educated as to the nuances of radial artery intervention. There are some subtle, but important, differences in the way staff prepare for a case:
• A pulse oximeter should be placed on the index finger or thumb of the arm that is being intervened upon. This allows for continuous assessment of the vascular integrity of the radial/ulnar system.
• The wrist should be adequately "cocked" to facilitate arterial access. This can be accomplished with either a small, well-rolled gauze or a splint-like device (Accumed Systems, Inc.).• The armboard should allow for access at approximately a 45- degree angle from the patient and then allow the arm/wrist to be placed next to the hip.• Conventional drapes are often inadequate. Specialized radial drapes are now available. It is often possible to move a femoral drape over to cover the wrist and the propped groin or to use brachial drapes.X. Transradial ArteryAccess There is a variety of equipment available for radial artery access. The basic components include a needle, wire and sheath. The specifications of each of these components vary considerably, making it vital to familiarize oneself with characteristics that allow successful access. Some physicians make a small incision in the skin over the needle while it is still in the artery. This helps facilitate insertion of the dilator and sheath.
The needle varies in length from approximately 2-5 cm and 19-21 gauge. We believe that longer needles allow the operator to pass through the radial artery without seeing the "flash" of blood return (which is quite minimal compared to a femoral approach with a larger gauge needle). Therefore, shorter needles seem more desirable. The bevel of the needle is important because of the small caliber of the artery. A gentler bevel angle allows for smoother movement of the wire.
The wires that are supplied are usually 30-50cm and often have floppy tip and a more rigid shaft. Considering the small caliber of the artery those wires with either a small angulation or even a straight tip seem to work better. J tips often get caught either in the sheath or the proximal artery. If the operator has difficulty with the wire in a kit, successful access is usually obtained with a hydrophilic-coated angulated wire.
The most common sheath size in radial intervention is 6F, although both 5F and 7F are not uncommon. Some experienced operators seem to prefer longer (23cm) sheaths to limit radial artery spasm. Sheath delivery into the artery can be difficult in cases were there is a step up in the transition between the dilator and sheath. A sidearm on the sheath is preferable to allow delivery of anticoagulation and antispasm medications.
XI. Transradial Medications
The medications that are used in transradial access are not yet standardized. There are several different combinations that are probably effective. We do not propose a specific combination, but instead offer suggestions for the operator based on our experience and review of the literature. Figure 1 summarizes the information.
Sedation: This is treated similarly to femoral intervention with the exception that the radial access patient is most likely to be uncomfortable during sheath insertion and removal and therefore conscious sedation protocol needs to be particularly addressed during these times. Many operators find fentanyl satisfactory. Antispasm; The radial artery can be subject to rather intense spasm which can be painful to the patient and make sheath and catheter movement difficult. A variety of medications have been used to help alleviate this including nitroglycerine, adenosine, verapamil, lidocaine, and papaverine. These medications are usually given during sheath placement and removal, and when the operator believes radial spasm is limiting catheter movement. We usually have syringes of nitroglycerin (200 mcg/cc), Verapamil (500 mcg/cc) and Lidocaine 2% (given in 20 mg aliquots) available. Occasionally, we have used Papaverine to wipe the sheath or catheter as this is a short acting myovascular relaxant. It has a direct paralytic action on the smooth muscle of the blood vessel. Although adenosine appears to have significant arterial dilatation properties its use seems to be limited by cost. Anticoagulation: This may be the most important aspect of radial artery intervention. Early studies had suggested very high rates of radial artery occlusion/thrombosis, which appeared to be related to insufficient anticoagulation (12-17). We administer a minimum of 5.000 units of intra-arterial heparin for diagnostic procedures and a minimum of 10.000 units for interventional procedures. Because direct injection of heparin intra-arterial can be quite painful, we mix it thoroughly with blood from the sheath. We have not experienced any increased rate of complications using radial access in those patients that had either been administered thrombolytics or intravenous GPIIb/IIIa inhibitors. We do not reverse anticoagulation before we remove the sheath.
Figure 1. Some medications used in transradial catheterizations
NTG200 mcg/cc Verapamil XII. Transradial Catheters/Guides Judkins Left and Right Judkins Left Judkins Right
One of the limitations of radial artery interventions has been the equipment that we, as interventionists, have available to us. In particular, this procedure has been limited by the diagnostic and guide catheters available. In the last several years, however, several new innovative designs have become available.
Despite these new designs, it is not uncommon to use standard Judkins catheters. Because of the different orientation in the aorta (from a radial approach) it is necessary to use different curves. When using a Judkins left from the right radial artery the curve should usually be .5 cm smaller than would be picked for a femoral approach with a similar aortic root. If this is not available a standard 4 curve can be used with a short tip.
When cannulating the right coronary from the right radial approach it is usually helpful to use a curve that is approximately 1 cm larger (i.e. a JR 5 instead of a JR4). When access is achieved from the left, radial conventional curves are usually satisfactory.
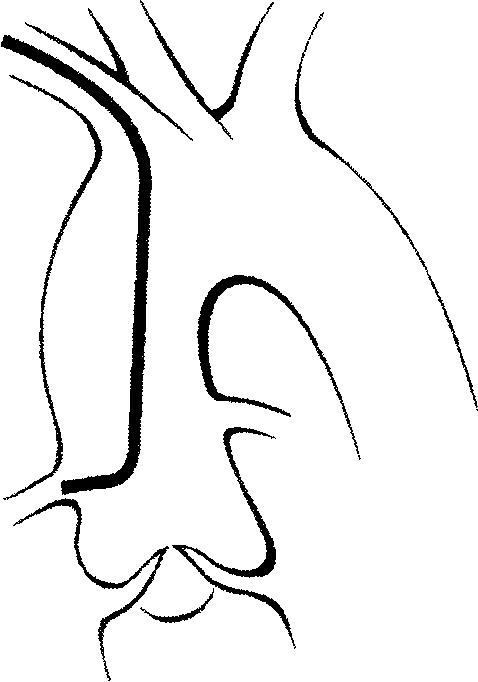
The Hockey Stick and Extra Back Up Hockey Stick Extra Backup
Two other catheters that were primarily designed for the femoral approach are helpful during radial cases. The Hockey Stick takes advantage of a relatively sharp 90-degree angle and relatively long distal segment (somewhat like a JR 5). This catheter can be used to cannulate both the right and left coronaries.
The EBU (extra backup), which is similar to the VODA®, takes advantage of the support offered by the contralateral wall of the aorta. Although this catheter offers excellent support, when used in 6F sizes, longer stents have some difficulty transversing the primary and secondary curves. This curve is best suited from a left radial approach and is used only for cannulation of the left coronary.
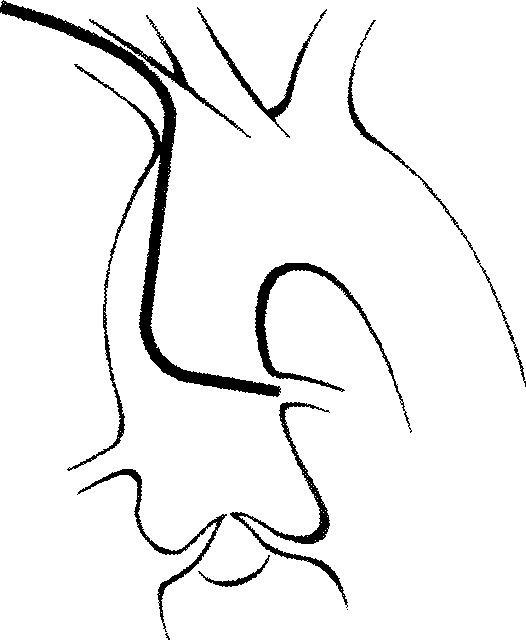
Multipurpose
The Multipurpose catheter, it's modified version Barbeau Curve, Kimny and others can be used from either arm to cannulate both the right and left coronaries as well as vein grafts. The Multipurpose A catheter has a subtler angle and is suited for inferior directed takeoffs. The Multipurpose B catheter has a right angle curve of approximately 90 degrees and is therefore better suited for horizontal or superior takeoffs. Multipurpose A Left (Modified) Multipurpose Kimny Curve
This catheter serves as the workhorse at William Beaumont Hospital for cannulation of both coronaries. It is specifically designed for radial artery intervention. The primary curve is 45 degrees with a secondary curve of 90 degrees that allows it to support itself on the contralateral aortic wall. It is common to cannulate the left coronary from below with this catheter while coming from a horizontal or superior position to cannulate the right.
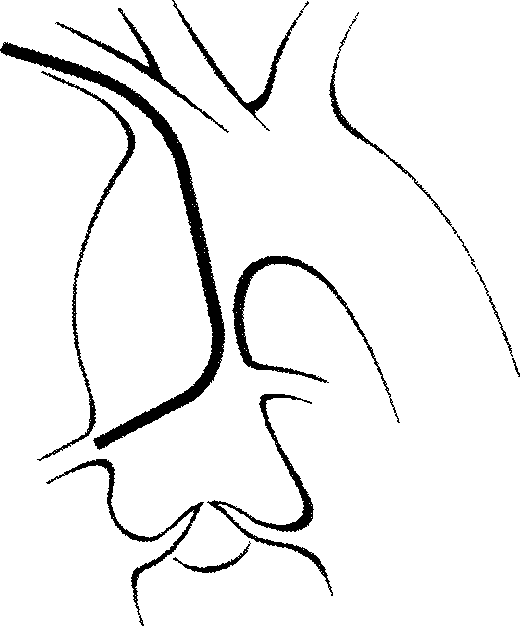
MPA2 Modified Left MPA2 Modified Right BarbeauCurve®
This catheter is a modification of the Multipurpose A. It has an additional 135-degree curve at the tip to assist in cannulation. It is best used via a right radial approach for the right coronary artery and/or vein grafts. Other There are a number of other catheters/guides available that are suitable for radial interventions that are not pictured here. These include: Sones catheters, Radial catheters, IMA catheters, modified sapheneous graft, as well as Castillo curves. The modified sapheneous curves and the IMA catheters should be used with caution by experienced operators as they incorporate very acute angles and could be potentially traumatic. XIII. Hemostasis Devices
There are various methods for obtaining hemostasis, as well as several hemostasis devices. The optimal method/device is not known, but each operator should probably be familiar with several methods/devices in case he/she comes across a case where it is difficult to achieve hemostasis. The methods/devices include:
• Gauze - Hemostasis can be obtained by placing several rolled 4 x 4's over the radial site and securing them with a • Hemoband (Access®) - This was designed to obtain hemostasis in patients with hemodialysis grafts and
therefore has a wide based area that compresses the radial artery. Although usually effective, it causes compression of the venous system leading to hand engorgement and is uncomfortable.
• Radial Clamp® - This device allows for a clamp-like device to put pressure directly on the radial site. • Radistop® - Similar concept to the Femstop and allows compression over the site. Moderate price. • Hemostasis Band (Schneider) - A simple elastic strap that allows compression of the entire wrist. It does not
allow point compression on the radial site and will cause some venous engorgement.
• Hemostasis Band (Accumed Systems, Inc.) - Specifically designed to allow point compression of the radial
site. Support blocks on the band allow for adequate venous return and therefore minimal discomfort.
• Blood Pressure Inflatable Cuff - Although rarely needed, this can control bleeding if the radial site is XIV. Sheath Removal & Hemostasis When preparing to remove the sheath, it is helpful to have several medications and certain equipment (as noted above) available. The medications include:
• Verapamil - Although not consistently given by all operators pre-removal some believe that it aids in removal by
• Nitroglycerin - Not used by all. It probably is less successful at arterial vasodilation. • Lidocaine - Given by some operators intra-arterial prior to sheath removal to decrease pain. Given in aliquots up to
• Sedation - Similar to drugs given during femoral line removal. Some operators find Fentanyl 50-100 mcg
XV. Pitfalls of Transradial Intervention Difficult Access
Hit it on the first try! The radial artery is prone to spasm and it is not uncommon, after you nick the artery, to notice a diminished (even if transient) pulse. If this occurs, and it appears to be related to spasm, you have several options:
• Have the patient clench/open the hand • Go to another site
If, however, there is a good pulse, but no blood flash is noticed in the needle, the physician needs to consider whether the radial artery has potentially closed and, if so, does the pulse represent flow from the ulnar through the palmar system?
On occasion the artery will be quite palpable, but difficult to stick. This is often seen in atherosclerotic calcified vessels. This is usually addressed by fixing the radial artery with the left thumb while attempting radial access.
Difficult Guide Wire Movement
After successful access is achieved it is sometimes difficult to advance the guide wire. The differential diagnosis includes:
• Spasm • Radial is occluded • Guidewire is in a side branch (usually too distal in the artery) • Abnormal take off of the radial (off of the brachial) • Radial artery stenosis • Against the wall or subintimal
If this situation occurs, the following options should be tried:
• Rotate the needle to change the angle of the bevel • Do a radial angiogram • Use a hydrophilic-coated wire • Trya.018PTCAwire • Give vasodilators through the needle and then try to advance wire
Difficulty Removing Sheath
This is quite uncommon but can be seen in smaller patients, women and patients with intense forearm radial spasm. In these cases consider:
• Pre sheath removal vasodilators and pain medications (see page 14) • Fix the proximal sheath (near the elbow) with your left hand • Gently rotate the sheath upon removal • Hold the skin distal to the incision to avoid "buckling"
Difficult Guide Placement
Although diagnostic and guiding catheters are now increasingly suited for radial intervention, the placement is still somewhat different than that used via femoral access.
Radial intervention requires knowledge of appropriate catheters and sizes (as detailed earlier in this manual). Several other maneuvers facilitate guide placement:
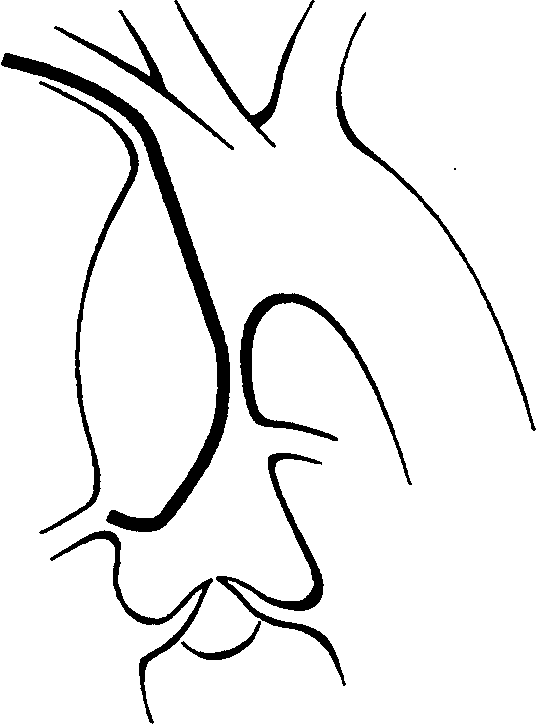
• Start the guide below the ostium (especially when approaching the left coronary). By pushing down on the catheter,
the tip will bend up toward the left main. Pulling the catheter back then will allow the tip to cannulate the ostium. This is different than conventional placement via a femoral approach, which usually engages the ostium from a superior position.
• Always use an exchange length wire when changing catheters to avoid the need to recross the great vessels. • Although rarely needed the patient can be asked to inspire and/or change the angle of the arm to facilitate catheter
XVI. Post Procedural Management It is our current policy to pull radial lines without waiting for a drop in anticoagulation parameters. Lines are pulled in the face of thrombolytics and intravenous GPIIb/IIIa inhibitors. Hemostasis is rarely a problem. In general, we leave the Accumed hemostasis band on for 30 minutes for a diagnostic case (5,000 units ofheparin) and 60 minutes for an interventional cases (10,000 or more units of heparin or Reopro). The site is then checked for hemostasis. If there is still evidence of bleeding, the band is left intact for another 30 minutes. In cases of profound bleeding where a lacerated artery is suspected, an inflatable blood pressure cuff can be used to control bleeding. Patients who undergo diagnostic radial intervention can be discharged within two hours. Patients can ambulate when their sedation wears off.
Complications arising from radial access are extremely rare and seem to be better tolerated than femoral access, despite the limitations in radial equipment to date (12-14,17). Pseudoaneurysms may form, but can be treated with local pressure dressings. If the site is enlarging or quite painful, an ultrasound should be performed and consultation with peripheral vascular surgery obtained.
When patients are discharged they are instructed to avoid flexion and extension of the wrist for the remainder of the day. Local swelling is treated with ice and analgesics. Rebleeding is treated with hand elevation and local pressure. Rebleeding at a radial site is certainly better tolerated and treated by patients than rebleeding of a femoral site.
XVII. Accessories A growing number of accessories have become available to help facilitate radial artery intervention. Wrist splint
The wrist splint (Accumed Systems, Inc.) keeps the
patient's forearm supinated and facilitates both access
and sheath removal/hemostasis. Without the splint
the patients have the tendency to progressively
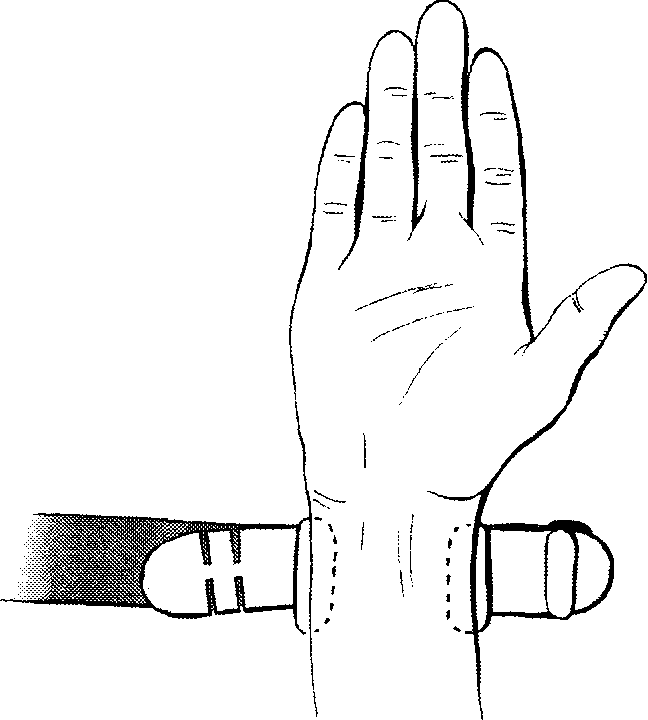
pronate the wrist during the procedure. The splint also reduces flexion of the wrist after hemostasis is obtained, which decreases the likelihood of re-bleeding.Hemostasis Band
Although there are several satisfactory ways to obtain hemostasis, we have found the use of the Hemostasis Band from Accumed Systems, Inc. superior to other available devices and techniques. This band reduces physician and/or nurse/technician time necessary to achieve hemostasis. In addition, it offers the security of preventing potentially serious rebleeds. Its unique design is comfortable and the foam support pad allows adequate venous return (a problem frequently encountered with bands or tourniquet devices).
There are a variety of sheaths available on the market that are probably suitable for radial access. There are some characteristics, however, that are desirable in a radial sheath. Although not utilized by all experienced operators, there is a trend toward longer sheaths (23-25cm) because of the concern of forearm radial spasm. It is not clear if this improves catheter movement, but they are widely used.
The sheaths used often come in a single or double dilator setup. The advantage of the double dilator setup is a more tapered atraumatic tip to avoid radial laceration. These sheaths however have a transition between the first and second dilators, which can often catch on the skin incision. The single dilator system, while transition less, is often more traumatic on the skin/ radial insertion site.
Several companies are currently engaged in development of sheaths specific for radial intervention. These prototypes include sheaths that can be dilated up in size; porous sheaths equipped for antispasm medication administration; and transition-less systems. References
1. Campeau, L. Percutaneous radial artery approach for coronary angioplasty. Cathet Cardiovasc Diagn, 1989;
2. Kiemeneij, F et.al. Transradial artery coronary angioplasty. Am Heart J, 1989;
3. Kiemeneij, F et.al. Percutaneous transradial artery approach for coronary Palmaz-Shatz stent implantation. Am
4. 1997 Cardiac Catheterization Lab Market Summary Report, Technology Marketing Group, 1998. 5. Johnson, WL et.al. Peripheral vascular complications of coronary angioplasty by the femoral and brachial
technique. Cathet Cardiovasc Diagn, 1994; 31:165-172.
6. Skillman, JJ et.al. Vascular complications of percutaneous femoral cardiac interventions. Arch Surg, 1988;
7. Oweida, SW et.al. Vascular complications associated with percutaneous transluminal coronary angioplasty. J
8. Otaki, M. Percutaneous transradial approach for coronary angioplasty. Cardiology, 1992;
9. Lotan, C, et.al. Transradial approach for coronary angiography and angioplasty. Am J of Card, 1995; 76:164-
10. Barbeau, GR, et.al. Right transradial approach for coronary procedures: Preliminary results. J oflnv Card,
11. Allen, EV. Thrombangiitis obliterans: Methods of diagnosis of chronic occlusive arterial lesions distal to the
wrist with illustrative cases. J Med Science, 1929; 178-237.
12. Spaulding, C, et.al. Left radial approach for coronary angiography: Results of a prospective study. Cathet
13. Benit, E. et.al. Frequency of a positive modified Allen's test in 1000 consecutive patients undergoing cardiac
catheterization. Cath Cardiovasc Diagn, 1996; 38:352-354.
14. Bush, CA, et.al. Cardiac catheterization and coronary angiography using 5 French performed (Judkins)
catheters from the percutaneous right brachial approach: A comparison analysis with the femoral approach. Cath Cardiovasc Diagn, 1993; 29:267-272.
15. Slagboom, T, et.al. Incidence and outcomes of radial artery occlusion following
transradial artery coronary angioplasty. Cathet Cardiovasc Diagn, 1997; 40:156-158.
16. Cooper, CJ, et.al. Patient preference for cardiac catheterization via the transradial vs. transfemoral approach. J
American College Cardiology, 1997; 29:30A.
17. Lefevre, T, et.al. Radial artery patency after percutaneous left radial artery approach for coronary angiography.
Theroleofheparin. European Heart Journal, 1995; 16:293.
Several websites are being developed which will allow the radial interventionalist to communicate with colleagues from around the world.The Radial Force at www.radialforce.org is an excellent reference site. In addition, our hope is to keep this manual updated on a regular basis at www.mhgpc.com.
The following references were obtained as of March 1999 and are felt to represent the most notable work in the field of radial artery intervention.
MASTER GARDNER INTERNATIONAL CONFERENCE Sponsored by The University of California, Davis DYNAMIC GROWING FOR MASTER GARDENERS WILLIAM R. JACKSON, PhD Author, Consultant, Educator This concise synopsis was made available to the Master Gardeners International for its Conference July 15-19, 1997, in Sacramento, California. At the time of this presentation on July 16, the audience s
Martina Lambert Head of Marketing and Communications LBBW Bank CZ a.s. Telephone +420 224 406 233 Telefax +420 224 406 483 martina.lambert@LBBW.cz www.LBBW.cz LBBW offers IQ Account for Entrepreneurs LBBW enhances its product portfolio with product especially designed for SME’s – IQ Account for Entrepreneurs IQ Account for Entrepreneurs is a package of com
 V. Pertinent Anatomy
V. Pertinent Anatomy 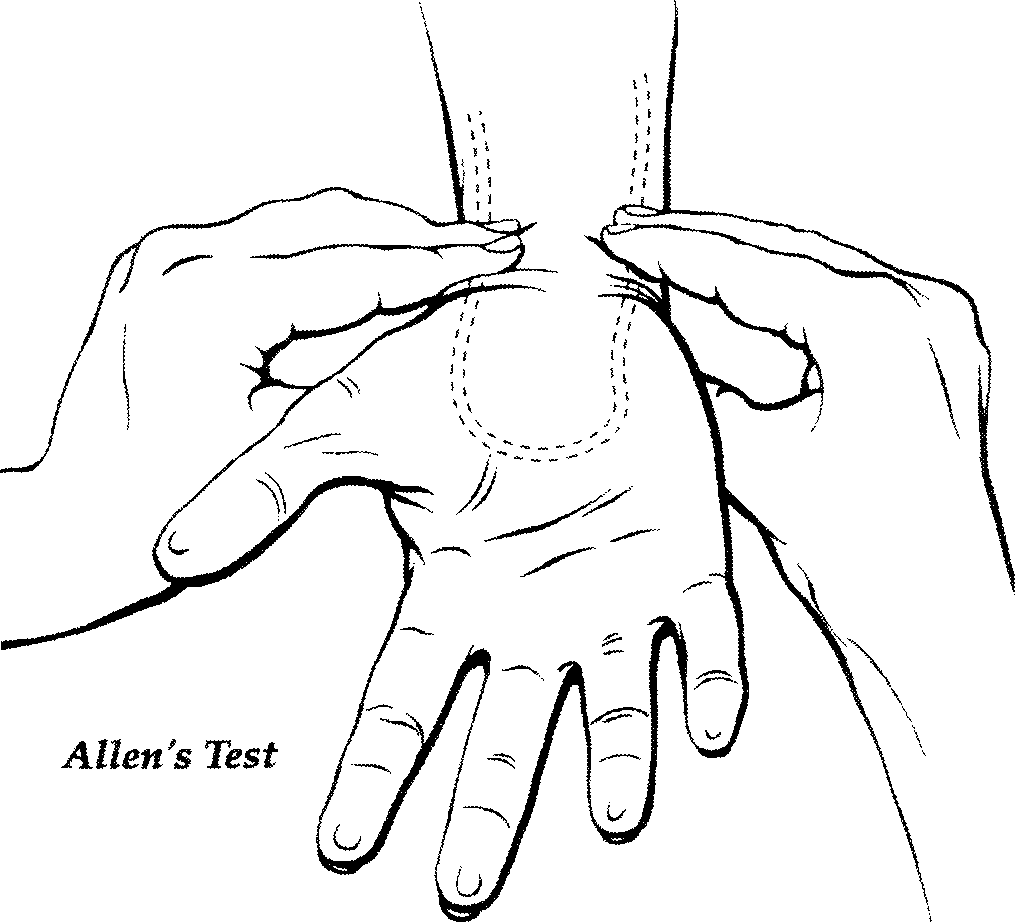 where it joins with the deep communicating branch of the ulnar artery and forms the deep palmar arch. The
superficialis branch of the radial artery joins with the palmar portion of the ulnar artery to complete the superficial palmar arch.
The ulnar artery also branches off the brachial artery and passes along the inner aspect of the forearm. At the level of the wrist, it divides into two branches that join the radial artery and its superficial branch to form the deep and superficial palmar arches.
It is not uncommon for a patient to display adequate ulnar and radial pulses, and have abnormal plethysmography (or Allen's test). Whether this represents true radial or ulnar dominance or inadequate/ incomplete palmar circulation (reported in up to 10-23% of patients) (11-12) is difficult to ascertain. Obviously patients who display radial dominance should not be intervened upon from the radial artery. In addition, patients with ulnar dominance would have a higher incidence of radial artery access problems, although this is not well described in the literature.
VIII. Patient Preparation
where it joins with the deep communicating branch of the ulnar artery and forms the deep palmar arch. The
superficialis branch of the radial artery joins with the palmar portion of the ulnar artery to complete the superficial palmar arch.
The ulnar artery also branches off the brachial artery and passes along the inner aspect of the forearm. At the level of the wrist, it divides into two branches that join the radial artery and its superficial branch to form the deep and superficial palmar arches.
It is not uncommon for a patient to display adequate ulnar and radial pulses, and have abnormal plethysmography (or Allen's test). Whether this represents true radial or ulnar dominance or inadequate/ incomplete palmar circulation (reported in up to 10-23% of patients) (11-12) is difficult to ascertain. Obviously patients who display radial dominance should not be intervened upon from the radial artery. In addition, patients with ulnar dominance would have a higher incidence of radial artery access problems, although this is not well described in the literature.
VIII. Patient Preparation 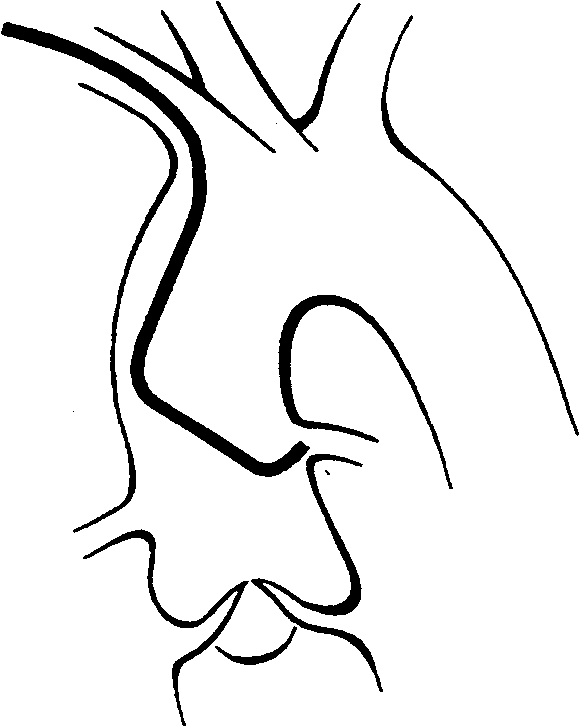
 XII. Transradial Catheters/Guides
XII. Transradial Catheters/Guides 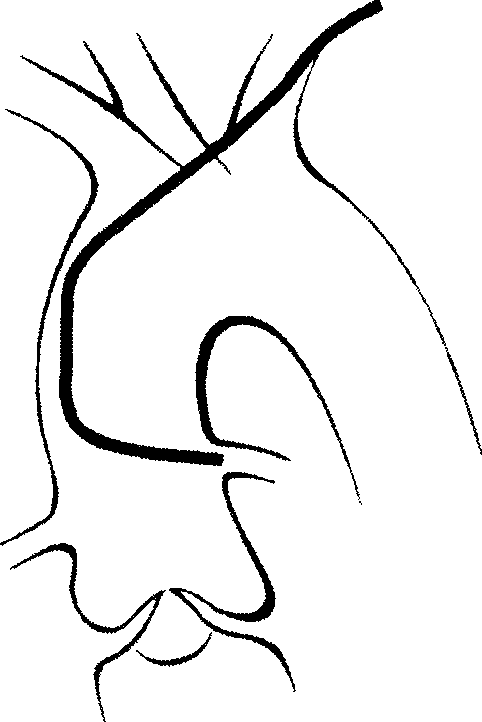
 The Hockey Stick and Extra Back Up
The Hockey Stick and Extra Back Up 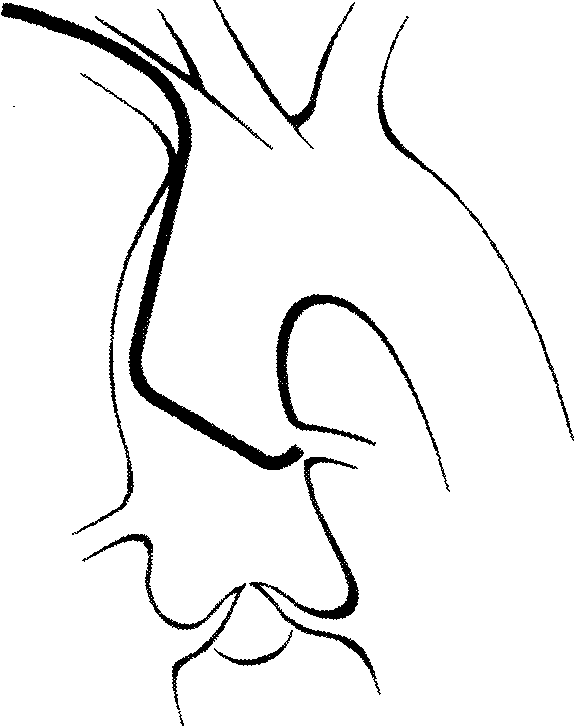
 (Modified) Multipurpose
(Modified) Multipurpose 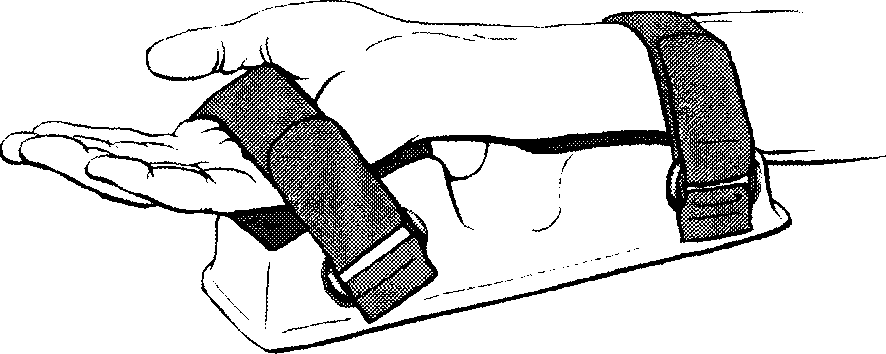
 XVII. Accessories
XVII. Accessories