Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Severnanesthesiaadvancedpainmedicine.com
CONFIDENTIAL SEVERN ANESTHESIA ADVANCED PAIN MEDICINE HEALTH QUESTIONNAIRE
Thank you for arranging to visit one of our physicians. When you come for your first visit, please bring this completed form along with any medical records, X-rays, CT or MRI scans, medication bottles and other medical information related to the problem for which you are being seen. Should you have any questions, please do not hesitate to contact us. Thank you very much. We look forward to seeing you. Please complete the attached questionnaire before your appointment. It is confidential and will be part of your medical
record. It asks for information about your current problems and
your past medical history. This form will give your doctor a
better understanding of your problem, and will allow him or her
to spend more time discussing treatment plans with you.
SEVERN ANESTHESIA ADVANCED PAIN M E D I C I N E Admin. office: 301 Hospital Drive Clinic Address: 300 Hospital Drive Glen Burnie, Maryland 21061 Suite 230 Phone: (410) 553-8056 Glen Burnie, MD 21061 Fax: (410) 595-1907 Mailing Address: PO BOX 403 Millersville, MD 21108 DATE:______________________________
Name:_____________________________________________________________________________________
City____________________________ State________ Zip___________
Primary Care Physician: Name:_______________________________________________
Address:_____________________________________________
____________________________________________________
# ___________________
List all other Physicians that your records should be sent to:
Pain Related Information. Please answer all questions.
1) Describe the event(s) surrounding the onset of your pain. (I.e. date of injury, is it the same or getting worse?).
___________________________________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
3) How many physicians have been involved in the treatment of your pain? (Please circle) 0-3
4) How many emergency room visits have you had in the last year for pain? (Please circle)
5) Circle all the things that make your pain worse:
6) Circle all the things that make your pain better:
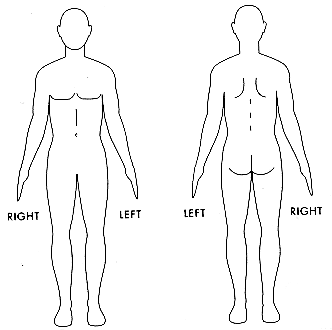
7) On the diagram, shade in the areas where you feel pain. Put an X on the area that hurts the most.
8) I have some form of pain now that requires medication each and every day Yes No
9) Did you take pain medications in the last 7 days? Yes No
Name: _____________________ DOB: _____________________
10) Throughout our lives, most of us have had pain from time to time (such as minor headaches, sprains, toothaches). Have
you had pain other than these everyday kinds of pain during the last week? Yes No If YES, what kind?
11) Please rate your pain by circling the one number that best describes your pain at its worst in the last week.
12) Please rate your pain by circling the one number that best describes your pain at its least in the last week.
13) Please rate your pain by circling the one number that best describes your pain on the average.
14) Please rate your pain by circling the one number that tells how much pain you have right now.
15) What kinds of things make your pain feel better (for example, heat, medicine, rest)?
16) What kinds of things make your pain worse (for example, walking, standing, and lifting)?
17) In the last week, how much relief have pain treatments or medications provided? Please circle the one percentage that
most shows how much relief you have received.
18) If you take pain medication, how many hours does it take before the pain returns? Circle appropriate response
19) I believe my pain is due to: a) The effects of treatment (for example, medication, surgery, radiation, prosthetic device)
b) My primary disease (meaning the disease currently being treated and evaluated)
c) A medical condition unrelated to my primary disease (for example, arthritis)
20) For each of the following words, circle Yes or No if that adjective applies to your pain.
Name: _____________________ DOB: _____________________
21) Circle the one number that describes how, during the past week, pain has interfered with your:
d) Normal Work (includes both work outside the home and housework)
22) I prefer to take pain medicine: (circle appropriate response)
23) I take my pain medicine (in a 24 hour period):
24) Do you feel you need a stronger type of pain medication?
25) Do you feel you need to take more of the pain medication than your doctor has prescribed?
26) Do you feel you need to receive further information about your pain medication?
Name: _____________________ DOB: _____________________
27) Other methods I have used to relieve my pain include: (Please check all that apply)
28) Check the nerve blocks, injections that you have had to relieve your pain?
Medical History: (including high blood pressure, diabetes, cancer, seizure disorder, stroke, etc)
Please List: ________________________________________________________________________________________
___________________________________________________________________________________________
Surgeries:
Have you had surgery in the past? YES NO
If yes, please list by date____________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
Family’s Medical History
Please list any major illnesses in your family. Including cancer, stroke, high blood pressure, diabetes, chronic pain, and others.
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
Medication Allergies
_____________________________________ ___________________________________________________
_____________________________________ ___________________________________________________
Are you allergic to iodine or contrast dye (for IVP, myelogram, etc.)? YES
If allergic, what happens? ______________________________________________________________________
Past Pain Medications: Have you ever taken any of the following pain-related medications? If so, please check and note any reason for discontinuing. Medication Last dose Stopped due to: Didn’t Stopped WorkWorking
ACETAMINOPHEN (TYLENOL) __________________
________________________________________
IBUPROFEN (MOTRIN, ADVIL) __________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
NORTRIPTYLINE (PAMELOR) __________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
PENTAZOCINE HCI (TALWIN) __________________
________________________________________
PROPOXYPHENE (DARVOCET) __________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
________________________________________
_______________________________________
________________________________________
_______________________________________
________________________________________
_______________________________________
________________________________________
Review of Systems:
Please review the list below. If you have currently, or have had a problem in any of these areas, please
circle "yes" and explain in the space below. If not, please circle "no". General/ENT
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
Lungs and Chest
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
Heart and Blood Vessels
______________________________________________________________
YES ______________________________________________________________
YES ______________________________________________________________
YES ______________________________________________________________
YES ______________________________________________________________
YES ______________________________________________________________
YES ______________________________________________________________
YES ______________________________________________________________
YES ______________________________________________________________
Urinary/Genital
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
YES ______________________________________________________________
______________________________________________________________
Bones/Joints
______________________________________________________________
______________________________________________________________
______________________________________________________________
Nerves/Brain
YES ______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
YES ______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
YES ______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
Stomach/Esophagus/Intestines
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
YES ______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
Psychology/Psychiatry
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
YES ______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
Endocrine
YES ______________________________________________________________
______________________________________________________________
YES ______________________________________________________________
Name: _____________________ DOB: _____________________
YES ______________________________________________________________
YES ______________________________________________________________
Abnormal Vaginal Bleeding, Discharge, or Pain
YES ______________________________________________________________
YES ______________________________________________________________
YES ______________________________________________________________
If yes, what do you do? ______________________________________ How many hours per day___________________
If no, how long have you been out of work? ___________ What was your occupation? ____________________________
If you do not work, how do you spend your day? __________________________________________________________
Yes No (explain)___________________________________________
Are you involved with Worker’s Compensation?
Is there any litigation pending against an employer or individual involved in an accident or injury?
Are you applying for disability or worker’s compensation? If so, which one? ____________________________________
HOUSEHOLD:
What are your hobbies?_______________________________________________________________________________
Single Married Separated Divorce Widowed
If you have children, how many and how old?_____________________________________________________________
DAILY ACTIVITIES: What exercises do you participate in? ___________________________________________________________________
Circle the number between 0 and 10 which represents your activity level.
inactive ) 0 1 2 3 4 5 6 7 8 9 10 (Very active) SPIRITUALITY:
Do you have a religious affiliation? YES ____________________
Circle the number between 0 and 10 which represents your involvement in religious activities (i.e. church, synagogue, mosque)
Name: _____________________ DOB: _____________________
EDUCATION: Have you completed? (circle)
Circle the number between 0 and 10 which represents your involvement in social activities
Is this a change since the onset of your pain?
If yes, how many packs per day? ___________ How many years? __________________
About how often? __________________________________________________
Was there ever a time in your life when you may have had an alcohol problem? YES
Did you or do you use street drugs? If yes, which ones _______________________________________________ NO
Have you ever been addicted to prescription drugs
Does anybody in your family have a history of drug misuse/abuse/addiction?
Have you ever been in a treatment program for alcohol or drug abuse?
If Yes, please explain________________________________________________________________________________
Current Opioid Therapy, if applicable (for example, percocet, oxycontin, duragesic patch):
What percent relief do your opioids (narcotics) provide? ___________________________________%
Do you you have any side effects from your opioids? (circle those that apply) no side effects, constipation, itching, dry mouth, nausea,
erectile problems, menstrual change, vomiting, dizziness, sleepiness, lightheadedness, problems urinating, appetite change, tooth
Are you any more functional from using opioids? (circle) No Yes If so, how?
___________________________________________________________________________________________
Are your opioids kept in a secure place? (circle) No Yes Where?______________________________________
Do you feel that your mood has improved from opioid therapy? (circle) No Yes If so, how?
________________________________________________________________________________________________
Has your quality of life improved? (circle) No Yes If so, how?____________________________________________
Name of pharmacy listed on opioid bottle? _____________________________________________________________
EXPECTATIONS:
What are you hoping to gain from your visit with Severn Anesthesia Advanced Pain Medicine?
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
Circle the percentage of pain relief you would feel would make your treatment worthwhile.
PLEASE NOW FILL OUT THE ENCLOSED “CURRENT MEDICATION LIST”. LIST ALL MEDICATIONS YOU ARE CURRENTLY TAKING (PRESCRIPTION, OVER THE COUNTER AND HERBAL). THANK YOU FOR COMPLETING THIS FORM.
ASU Herberger Institute Season Subscriptions Ticket Form Please specify the number of tickets next to the preferred date and time below. Subscription enrol ment requires a minimum purchase of four event tickets per person. Information Colin Higgins: The Best Big Love by Charles L. Mee Little Whorehouse in Texas Last Name Emerging Artists I (Workshop $8) (Smith
derStandard.at | Gesundheit | Körper "Zur Sicherheit Antibiotika" Die Antibiotika-Debatte um gefährliche Resistenzen und Nebenwirkungen verunsichert die Patienten - Eine STANDARD- Diskussion Antibiotika haben zurzeit nicht den besten Ruf. Die Resistenzproblematik steigt -dazu gelten sie als mögliche Auslöser von Allergien. Bert Ehgartner bat denInfektionsexperten Stefa
 Pain Related Information. Please answer all questions.
Pain Related Information. Please answer all questions.