Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Interdisciplinary essay
Introduction
Alzheimer’s can be extremely scary when you do not know what you are up against. This
is why I chose this topic for my paper. This topic interests me because Alzheimer’s has only been
discovered for about 100 years, and there is so much that is still unknown. Alzheimer’s affects
me greatly because my grandmother has suffered from this disease for over ten years, and is now
in the final stages. I remember when I was about nine or ten, my whole family went to my
grandmother’s doctors office and the doctor explained what Alzheimer’s was, and how they were
going to try and treat it. My grandmother had offered herself to be a guinea pig, so to speak. The
doctors did many tests on her to try and learn if there would be any way they could find a cure or
better treatment than they one they had now. Unfortunately, nothing new was found, but now my
family knows to take precautions for it, and we have slowly learned how to aid my grandmother
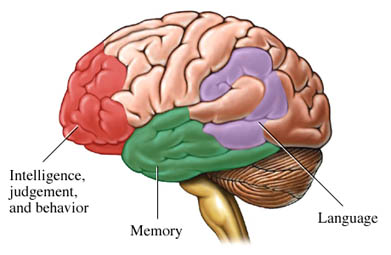
Alzheimer’s is a fairly recent discovery. It is is a memory disease- the disease affects the
section of the brain that controls memory, behavior and language.
Figure 1. Parts of the brain affected by Alzheimer’s disease
What I do know is that there are three medications that are Alzheimer’s specific (Aricept,
Reminyl, and Exelon), and that they all come with very serious side effects. As for genetics,
studies have shown that contracting Alzheimer’s is just like catching a cold - random. Heredity is
very slim in being diagnosed with Alzheimer’s, but people can be tested at age fifty to see if they
are at risk at all. My mom, for instance, is going to Yale-New Haven hospital fairly soon to test
for a genetic line of her being diagnosed with Alzheimer’s because her mother was an
In the early stages, one forgets little things, but as it progresses you forget your
grandchildren, your children’s names and even yourself. Alzheimer’s affects the elderly- mid to
late 50’s is when the earliest signs can be detected. When Alzheimer’s progresses, one
unfortunate outcome is that the patient becomes extremely hostile (my grandmother’s case is an
exception here). Alzheimer’s is a fatal disease, although it kills very slowly.
After choosing to study Alzheimer’s disease, I found the following questions: Why was it
only discovered in the early 1900’s? Is there still no cure for Alzheimer’s Disease? What role do
genetics play in Alzheimer’s? Will genetics be a possibility in the future? How has the media
affected Alzheimer’s? What are the sociological effects of Alzheimer’s disease? What are the
psychological effects of Alzheimer’s disease? What are the possible treatments and cures for
The objectives I have concluded are: To explain the background and history of
Alzheimer’s disease.To explore treatments and the reason there is no cure for the disease yet.To
learn about the studies of genetics, and why scientists believe Alzheimer’s is not hereditary. To
discover the possibility of genetics in the future of Alzheimer’s disease. To learn the possible
treatments and cures for Alzheimer’s disease. To understand why patients have struggles with
social interaction. To understand the psychological endeavors patients face. History and Background of Alzheimer’s Disease
Alzheimer’s Disease affects the brain; more specifically, the part of the brain that triggers
memory and recognition. AD patients experience symptoms early in the disease such as
forgetting directions, misplacing items, and losing train of thought quickly (Personal
Experience). Eventually, AD deepens in the brain and affects personal aspects and control. Most,
if not all AD patients forget their own names, the names of their children, grandchildren, etc.
(Personal Experience). Because the memory is lost, the person with AD loses consciousness of
personal space, motor control, and voluntary and involuntary actions (Personal Experience). The
saddest part about Alzheimer’s is that because the disease attacks the brain, it is eventually fatal.
What is hard for many people to cope with is that by the time they do die, they patient has no
idea what is happening to them and cannot remember anything. What others do not understand is
how deeply affective AD is in people, and those who do not have a loved one with AD cannot
possibly understand how dreadful the disease is.
AD has been slowly aiding to elderly deaths for many years. The disease, founded by
Alois Alzheimer (for whom the disease was named after) in 1907, was not found to be a major
disease until the 1970’s (Reger). Alzheimer sought a case of a woman in her fifties who showed
signs of lack of memory, social behavior and language, and after her death performed an autopsy
on her brain to discover an abnormal amount of senile plaques - unusual formations in the
presence of neurons - that caused the symptoms of Alzheimer’s disease (Reger). Before the
discovery, “senility and dementia were still considered part of the aging process. AD did not
become a common term, or even a large concern, until neurological research exploded in the late
1970s” (Reger). Although it was not a huge concern until decades later, once AD was starting to
be recognized as a detrimental disease, researchers started to begin finding treatments for AD.
AD develops very differently in different people. To properly diagnose and treat AD is
very hard, and while a person is alive, it cannot be properly diagnosed. AD is a slow developing
disease, which makes diagnosing it difficult (Reger). Though dementia itself is a form of
memory loss, Alzheimer’s is a very specific form of dementia, and it takes great lengths for a
doctor to properly diagnose any form of dementia, especially AD (Personal Experience). To
obtain a correct diagnosis of Alzheimer’s disease, doctors have to perform a special neurological
biopsy on the brain throughout different stages of AD, which has been deemed unethical,
therefore the only way doctors can positively diagnose AD is an autopsy after the patient has
died (Reger). Though a multitude of studies have been conducted on thousands of AD patients,
no cure has been proven efficient for the disease (Reger). For the time being, patients resort to
medication to steady the onset of new symptoms and stabilizing the illness (Personal
Experience). Researchers continue to study AD every day to find new methods of treatment and
a possible cure, but so far they have been unsuccessful.
Adult Children’s Anxieties with Alzheimer’s Disease
Going through Alzheimer’s is tough being the patient, but almost comforting because you
cannot remember what exactly is happening to you. Being the child of a parent with AD can pose
many new questions about the disease. At the University of Illinois, a study was conducted about
the effects of Alzheimer’s disease on adult children.
One of the most important things adult children should realize is that they may well be the
prominent caregivers for their parent. Found in one of the studies, “Adult children may face
uncertainty related to their position because of the likely necessity to reverse roles with the
parent. The current study examines the sources of uncertainty for adult children related to a
parent’s diagnosis of possible Alzheimer’s disease” (Stone). Because the onset of the disease
comes so fast, children barely have time to cope with what will happen in the future to their
parents and how they will be able to care for them. In many instances, such as my own, children
hire visiting nurses to help with their parent (Personal Experience). However, the uncertainty still
arises about what is going to happen to their loved one. One of the questions that arises when a
loved one is diagnosed is “could this have been prevented?” Studies have shown that it depends
on what stage of Alzheimer’s the patient is in, and that genetics may play a large role in the
outcome (Stone). Thus, children may develop anxieties about the future for their parents, and
also a future for themselves. Because of this, they find many issues and anxieties that they would
not normally think about. Medical, personal, and social issues arise in adult children and they
experience an uncertainty in their lives that they need explanation in order for them to manage
with what is happening (Stone). Once children find the right sources, such as talking to doctors,
researching the disease, etc. they will be able to handle the fact that their loved on has
Alzheimer’s and they can learn how to move forward in giving the appropriate care for them.
The Media and it’s Effect on the Portrayal of Alzheimer’s Disease
What most people know about AD are the basics: it affects elderly people from age 50
onward, and it is a disease that makes a person lose their memory (Personal Experience). Many
people may not understand that they are extremely exposed to Alzheimer’s disease in their
everyday life, regardless if they are living with a family member who is a patient. The media
affects a countless number of people, and most of them do not even realize they have been
affected. One of the most popular forms of gaining information through the media is through
One movie that is very pivotal in young adults’ lives is The Notebook, directed by Nick
Cassavetes. The movie, though about two young lovebirds in the 1950’s, shows the couple as
elderly people in a retirement home throughout the movie. Toward the end of the movie, the
main character Allie breaks through her forgetfulness and realizes that the man reading their life
story is her husband, Noah. It is at this point the viewer understands that Allie has a very serious
form of dementia, which has been named as Alzheimer’s disease in Nicholas Sparks’ book
(Sparks wrote the book inspired for the movie). Because this is such a popular movie, the
Alzheimer’s aspect of the movie has been “Hollywood-ized,” meaning that it gives Alzheimer’s
a more glamorized outlook. I have learned this because I have so much experience with a
grandmother with AD. In the movie, Hollywood first made Allie look stunning for a 70 year old
woman. Her clothes matched perfectly, she looked well cleansed, and had makeup smeared all
over her face. In actuality, AD patients forget how to match their clothes, forget how to shower,
(therefore having a visiting nurse or regular nurse bathe them) and forget what makeup is, let
alone put it on. The actual disease at some points in the movie seemed either over exaggerated or
not explained enough. In the movie, the doctors inject Allie with a tranquilizer to settle her down.
Normally, the doctors would not do this unless it were a dire emergency, which at this point it
was not. Unfortunately, most AD patients do not have breakthroughs where they remember
everything that has happened throughout there life. This gives many people false hope that
something may happen to their loved one and they will remember them even for five minutes.
The Notebook gives different characteristics to the portrayal of AD, which gives viewers a false
representation of the disease. This is the media affecting the perception of AD on the everyday
person. By watching this movie, people may think they know all they need to know about AD,
when in essence, they have no idea what they are talking about. Though they have a general gist,
they do not fully understand what happens to a patient with AD, and they are unprepared for
what it actually is when a person they love is diagnosed with AD.
Another film portrayal was a lesser known movie filmed in Canada entitled Away From Her, (directed by Sarah Polley) based on the short story featured in The New Yorker, called “The
Bear Came Over The Mountain.” I read this story my senior year of high school, so when I found
out that there was a movie based on the story, I was excited to see how parallel the two were. The
story was quite an accurate description for a patient with Alzheimer’s; Fiona, the woman with
Alzheimer’s, was described just as an Alzheimer’s patient would be, and her husband, Grant, put
up with every inconvenience he faced during her illness.
I watched the movie after rereading the story to see if there would be any difference
between the two. Thankfully, the movie matched the story to a tee. Fiona was portrayed as a free-
spirited woman who liked to ski and be with her husband Grant. In one early scene, Fiona and
Grant were washing the dishes, and after Fiona had dried a pan, instead of placing it in the
cupboard, she placed it in the freezer and walked off. In another scene, the whole kitchen was
labeled with what was in which drawer, so Fiona would know where to put the dishes when she
was finished with them. Though I was very young, I think my grandmother had done this at one
point to remember where to put everything when she was done using something. What my
grandmother does that Fiona did was during the scene when Fiona was at the doctor’s office, she
got up right in the middle of the appointment and told her husband that it was time to go. She had
no recognition of where she was, and that it was wrong to leave just then, which has been found
During the middle of the movie, Fiona and Grant make the executive decision to move
Fiona into a medical facility that caters to Alzheimer’s patients. They director tells Grant he is
not allowed to visit Fiona for 30 days for fear that she would not adjust. After the 30 days, Grant
goes to visit Fiona, but unfortunately, she does not recognize him at all, and instead thinks very
highly of one of her friends she has made, Aubrey, as her husband. This continues throughout the
movie, and it is very unfortunate for Grant as he copes with the stress of his wife’s disease. In
many cases, the spouse of the patient starts to feel under pressure to make sure that their partner
is comfortable, or is able to cope with what is happening in their mind.
This movie portrayal is an excellent example of what happens to AD patients. The
symptoms of Alzheimer’s is very clear, and when the viewer sees Fiona forgetting everything
around her, they instantly know that she is suffering from Alzheimer’s disease. Unfortunately,
this movie is little known to American viewers (the movie was set in Canada) and therefore not
popularized as one of Hollywood’s hallmark movies. For people interested in viewing the
process of Alzheimer’s disease and seeing what happens to those affected by it, Away From Her
is the perfect movie because each minute detail is exaggerated through Fiona’s movements,
language and thoughts. This film is one way the media can positively affect the general
population’s knowledge of Alzheimer’s without glamorizing the gritty details.
Public Relations and Communicating Awareness of Alzheimer’s Disease
Alzheimer’s disease is one that many people know about. They know what AD is, and
they know that it is potentially fatal, but people do not know how to respond to people with AD
or where to go to learn about it. One way to raise awareness about the seriousness of Alzheimer’s
is by going about it through Public Relations.
One of the major ways to gain public access to a cause is to broadcast through television
and cable. Recently, a Video News Release was produced to educate viewers on Alzheimer’s
disease (Barton). The picked up 4.8 million viewers, meaning the stories were broadcasted to
over 40 million people (Barton). By communicating the importance of Alzheimer’s through ways
of communication that people are bound to listen to, awareness can be raised.
Another way of awareness was a public service announcement that played on the DVD
for Away From Her. At the beginning, the audience sees many of their favorite actors and
actresses fighting for a way to make Alzheimer’s more treatable. Many of these celebrities, such
as Peter Gallagher, have family members who suffer from Alzheimer’s and admit that
Alzheimer’s has not raised enough awareness, so they are fighting to get the people to learn more
about the disease and fight for a cure. It seems that when people see someone they idolize doing
something good, something to cure a disease and raise awareness, they follow that. By getting
these big celebrities to fight for a cure for Alzheimer’s, people will finally realize how horrible
AD is and they will want to find out more about it. They will do their research and learn that
there is so much doctors do not know, and this all happens because someone they look up to
started it. The communication between celebrity and average joe is what aids the awareness.
Psychological Effects on Patients with Alzheimer’s Disease
Alzheimer’s disease, as many people know, affects the portion of the brain that controls
memory. A person’s memory coincides with their psyche, therefore making a sizable parallel to
Alzheimer’s disease and the psychological issues that stem from it.
Many behavioral issues originate from simple symptoms. Waking up at night for no
reason, and wandering the house at night are psychological issues that many AD patients have,
though it is still unexplained (Konishi). Though this appears in individuals who are at a later
stage in Alzheimer’s and their life, it has been found in Konishi’s study to be fairly frequent for
most patients. Delirium, in later stages of Alzheimer’s where the affected person is relatively
incoherent, is the most outstandingly common behavioral symptom (Konishi). In many cases,
including my grandmothers, the Alzheimer’s has taken over so much of the patient’s brain that it
causes them to have delusions and hallucinations (Personal Experience). Many times my
grandmother will walk around her house talking to herself. More often though, we find her
talking to people who are not there. She mainly references to small children, saying statements
such as “Look, the little boy over there is doing something with the doo dee doo and the da dee
da” and will walk over to where the “little boy” is and start talking to him like he is a friend. In
this case, the hallucination is the little boy, and another psychological aspect is when she says
“doo dee doo.” Because her memory is affected, she cannot remember words or what she wants
to say, so she makes up words or noises to put in place of the missing phrases.
Other forms of psychological problems come varied. Agitated depression was found to be
a major behavior issue throughout most Alzheimer’s patients (Konishi). As the Alzheimer’s
progresses into the brain, emotions become distorted for the person, and most of them end up
becoming very hostile (Personal Experience). Hostility is a surprising form that Alzheimer’s
takes. It is found that depending on the patient’s life before the diagnosis (i.e. if the person were
very happy, abused, clinically depressed) that affects the hostility of the patient (Personal
Experience). In my grandmother’s case, she was one of the sweetest, happiest ladies anyone had
met. It makes sense now that she would be constantly happy and singing and dancing all around
her house all hours of the day. For those people who feel they had a mediocre or unfulfilled life,
they tend to be much more unfriendly as the disease progresses (Personal Experience).
In one study on the psychological behaviors of Alzheimer’s patients, researchers found
that patients have personality traits that can be categorized into five groups: Neuroticism,
Extraversion, Openness to Experience, Agreeableness, and Conscientiousness (Duberstein).
Based on these five behaviors, researchers wanted to learn the different personality traits most
Alzheimer’s patients experience. High neuroticism, low conscientiousness, and low openness
were found to be the most influential personality traits of AD patients (Duberstein). This means
that many patients suffer from being extremely neurotic (experience distress and anxiety) not too
conscientious (capacity to plan ahead, and work steadfastly toward goals) and not very open
(pursue emotions, ideas, art, fantasy, etc) (Duberstein). Because of these personality defects in
Alzheimer’s patients, their psychological being is much different than that of a person without
There are many different thoughts that run rampant in an Alzheimer’s patients head. They
have so many psychological issues because their brain is a huge mess. Conversations that
Alzheimer’s patients have with other people are very frequently incoherent because their brain
cannot process what exactly they are trying to say (Personal Experience). These psychological
standbys create friction between the patient and those with whom they are trying to communicate
with, and if the person to whom they are speaking does not understand the background, many
social issues may arise from this as well.
Familial and Social Issues for Patients with Dementia
As stated before, Alzheimer’s can create much confusion for children and loved ones.
This creates many social issues for both the family and people around the patient, as well as the
patient themselves. Their social lives begin to diminish as the disease worsens, because quite
frankly they do not know how to interact with other people once the disease develops.
Many families have trouble caring for their loved ones with Alzheimer’s. My family, for
example, is one of them. My grandmother has Alzheimer’s, and my grandfather has Parkinson’s
disease. Because of this, my grandfather cannot easily take care of my grandmother. My family
is the closest to them and we live about a half and hour away. This makes it very tough on my
mother when something goes wrong with them, so now they have a visiting nurse that comes
three times a week to care for my grandparents. It was not very easy to find a nurse though. To
help the state determine that they would benefit from the help, many social workers had to come
in and make sure that the resources put in to my grandparents would be useful. Social workers,
instead of caring for children mainly, have now found that they are learning to help with the
needs of elderly clients more (Pinson). Professional care is now becoming more prevalent
mainly for elderly families who suffer from Alzheimer’s. Although this is helpful, the family
generally takes control of the care, including all expenses. “The expenses of professional
caregiving or institutional care lead many families to opt to provide care for their loved one by
themselves in the home” (Pinson). Because professional care becomes expensive, families tend
to hold off until the last possible moment for getting the help they really should be getting
To help raise awareness, and gain more assistance for people with Alzheimer’s, churches
are trying their best to help Alzheimer’s patients keep a healthy social life (Pinson). As an
example, my grandmother, regardless of her stage, always went (and still goes) to church.
Though she does not understand what is actually going on, she hums and sings along with all the
music, and the people make sure to fellowship with her after and they converse about nonsense.
The fact that the church is doing what they can to still include her is heart warming, and it shows
that the church in general is trying to extend awareness to those with dementia and Alzheimer’s
Both church and caregiving can interlink with each other. “The use of volunteers,
caregiver support teams, spousal support programs, multi-disciplinary teams, church-based older
adult teams and educational resources are avail- able in some churches” (Pinson). By having an
extra service of churchgoers, families can take a break from caregiving. The congregation helps
the patient with caring for them, and by doing this they learn how to socially interact with them.
By learning how to interact with the patient, it can help make the patient feel at ease with the
person. One way of getting more social activities for the patient is by “organizing a volunteer
schedule and matching active elderly or younger adults with frail elderly or caregivers can be an
effective first step toward learning about—and meeting—the distinctive needs of this
population” (Pinson). This way, others start to feel comfortable with Alzheimer’s patients and the
can learn how to communicate with them, regardless of how incoherent they can be.
Though Alzheimer’s patients do not react the same way normal people would when
interacting with other people, they still have conversations and interact with others the way they
normally would. It helps that families want to help give care to their loved ones. By doing this,
they can still have social interactions with people that love them and will not judge them. This
also helps the families because it is not costly, and they can still connect with their loved one,
regardless of whatever state they are in. Though it gets very hard at some parts, the families are
very beneficial to the patients. It is also beneficial for people unrelated to the family to help give
care to the patient. Visiting nurses who are trained to care for people with Alzheimer’s disease
can help the patient with medicines and major care taking when the family is unable to do so.
They also provide outside interaction for the patient. The church functions also are very
favorable for the patients. Social interaction with others can help stimulate the patient’s brain and
also keeps aggression and anxiety to a minimum.
All these effects can eventually help into the possible treatment for Alzheimer’s. The
social interaction can be considered a therapy that keeps the brain stimulated, therefore
preserving the patient’s memory for as long as possible.
Medicine, Treatments and Cures for Alzheimer’s.What are the Possibilities?
Throughout the time Alzheimer’s has been known, researchers have been trying to find a
cure for the disease. However, there is no known cure for Alzheimer’s yet, though scientists are
doing all the can to find one. In the beginning stages, there are medications a patient can take to
prolong the onset of dementia. The three main prescriptions patients take are Aricept, Exelon,
and Reminyl. The purpose of these three drugs is “to prevent an enzyme known as
acetylcholinesterase from breaking down acetylcholine in the brain. Increased concentrations of
acetylcholine lead to increased communication between the nerve cells that use acetylcholine as
a chemical messenger, which may in turn temporarily improve or stabilize the symptoms of
Alzheimer's disease” (“Drugs”). Although all of the medicines work in a similar manner, each
has it’s own side effects depending on the individual (“Drugs”).
Aricept, also known as donepezil (Ringman) was the first of the medicines to be put on
the market in the UK for Alzheimer’s disease (“Drugs”). Donepezil is also the most common
drug to be prescribed to Alzheimer’s patients (Personal Experience). Donepezil has been the
most researched treatment for Alzheimer’s, therefore aiding to fact that it is most prescribed and
thought of when doctors think of medications (Ringman). Aricept has been found to work best
on “mild-to-moderate AD patients” (Ringman). What Aricept is commonly known to help with is
slowing down memory loss (Personal Experience). Most patients take it to help keep their
memory, while it does more than just that. Other ways Aricept can help Alzheimer’s patients is
by helping other mental issues that are affected by Alzheimer’s disease, such as attention and
language abilities (Personal Experience). Though Aricept is not a cure for Alzheimer’s, it works
exceptionally well in most cases by prolonging the patient’s memory.
Exelon, or rather rivastigmine (Ringman) is very similar to donepezil. As the second
prescription to be considered safe to use in the UK, the effects are generally the same (“Drugs”).
It has been licensed specifically for Alzheimer’s disease (“Drugs”). Exelon, though it has many
benefits, has similar side effects as Aricept, except there are more effects and severe, including
nausea, vomiting, and possible weight loss (Ringman).
Reminyl, otherwise known as galantamine (Ringman), affects patients the same as the
previous drugs. Reminyl is derived differently from Aricept and Exelon. The drug is “isolated
from various plants and is a competitive and reversible inhibitor of acetylcholinesterase. It has
been used in Europe and by anesthesiologists to help reverse paralysis and was approved for use
in patients with AD in Austria prior to 1995” (Ringman). Reminyl, though probably the safest of
the three drugs, is the least prescribed because of studies finding that it takes much longer to
begin to work than any of the other drugs (Ringman). Though still very effective, it does not
quite compare to the helpfulness of Aricept and Exelon.
Although Aricept, Exelon and Reminyl are the most popular and most used medicines to
treat Alzheimer’s, there is another drug that can be added to each of these medications to further
help prevent memory loss. Ebixa, the newest of the drugs (“Drugs”), also known as memantine
(Ringman), is generally added to Aricept to help Alzheimer’s patients prevent more symptoms,
because it has been found that combining Ebixa and Aricept is more helpful than just the Aricept
because the benefits are much stronger (“Drugs”). Memantine was first used with Parkinson’s
disease patients and other neurological conditions which caused researchers to test using the
medicine on Alzheimer’s patients (Ringman). They found that, though it was not effective on its
own, it could aid in the other drugs already manufactured (Ringman). Ebixa “protects brain cells
by blocking the release of excess glutamate [a messenger chemical in the brain]” (“Drugs”).
Though Aricept, Exelon, and Reminyl are generally used for patients with mild-to-moderate
Alzheimer’s, Ebixa slows down the progression of symptoms and, combined with Aricept, can
be used in moderate-to-severe patients (“Drugs”).
No matter how much these drugs can help patients, they cannot cure Alzheimer’s. They
can only prevent the symptoms and memory loss from becoming more prevalent in the patient’s
brain. However, studies have shown that there is new research starting to come out with ways of
preventing, curing, and detecting Alzheimer’s at an earlier stage in life. While it is a stretch,
researchers are trying to perfect these drugs and have them licensed so that people may begin to
During one study, researchers had administered all medications except any psychotropic
medications throughout the six month study period (Hori). Though Hori does not specifically
mention what medications were used during the study, it [the study] is being tested for
psychological symptoms in Alzheimer’s patients. While not much is said about specific
medications being used in this study, whatever the researchers used had a significant impact. The
doctors were able to advise specific medications for patients depending on where their brains
were cognitively (Hori). This is a step forward for Alzheimer’s research- now that researchers
have found medications that can be used for psychological functioning in AD patients, as well as
medications to help prolong memory loss, hopefully soon, more in-depth study of Alzheimer’s
doctors can find a concrete cure or prevention for the disease.
One of the most surprising pieces of information found when researching cures and
treatments for Alzheimer’s disease is the fact that there is a possibility for a vaccine against
Alzheimer’s disease. Vaccination has now been found to be a therapeutic approach for
Alzheimer’s disease (Wisniewski). In model animal trials, a great success has been reported, and
in the minimal amounts of study done on humans, it has been successful for the race as well
(Wisniewski). The purpose of the vaccination, and the vaccination itself is “passive
immunization consists of an injection of pre-prepared antibodies to patients, in contrast to active
immunization, in which the immune system is stimulated to produce its own
antibodies” (Wisniewski). This means that these antibodies are made to prevent the onset of
Alzheimer’s. Trials started in December 2007, and have had a huge success rate since then
(Wisniewski). Though more studying needs to be done in this area, researchers hope this could
be a new possibility of preventing and treating Alzheimer’s at this point in time.
Finding a cure for Alzheimer’s entails a massive amount of research. Because heavy
research only started in the 1970s, there has not been a concrete cure for Alzheimer’s. With the
awareness Alzheimer’s is gaining, by the time the young generation reaches an elderly age, there
will be preventions, treatments, and cures for Alzheimer’s disease.
Biological Standpoints on Alzheimer’s Disease
Biology is one of the main ways of studying Alzheimer’s disease. As a natural science,
studies show the different variations of Alzheimer’s and the type of disease it actually is.
Throughout my research, the term “vascular disease” came up multiple times. A vascular disease
is one that affects the cardiovascular - or heart - system. I found this to be quite strange, because
Alzheimer’s is a memory disease inside one’s brain. After looking deeper into this hypothesis, I
soon understood why biologists would think of Alzheimer’s as a vascular disease.
A study performed by Massimo Musicco and others was aimed at different factors,
including vascular factors predict a decline in Alzheimer’s disease progression (Musicco). In this
study, researchers wanted to see if any of these factors would increase the decline of memory
loss in Alzheimer’s patients. In the study, it was found that the disease progressed more slowly in
Alzheimer’s patients with diabetes (which could be considered a vascular disease). When
learning more about Alzheimer’s, and treatments, biologists can keep this insight in mind.
In another study conducted by Didem Dede, these doctors also wanted to learn if
Alzheimer’s was a vascular disease, and if so, how they could treat and prevent it from
beginning. They found that endothelial function is impaired in patients with Alzheimer’s disease
(Dede). Endothelium is a thin layer of cells that line the interior of surface blood vessels
therefore making endothelial function dependent on the amount of cells that are in the blood
vessels (Dede). The reason these researchers wanted to study Alzheimer’s to see if it was a
vascular disease was because it has been found in many disease that endothelial function is
impaired, and the disease that cause endothelial function are risk factors for Alzheimer’s disease
(Dede). They found that though there are many similarities between vascular diseases and
Alzheimer’s, it is not to be considered a vascular disease.
When comparing diseases to Alzheimer’s, biologists and researchers attempted to make a
connection between Parkinson’s disease and AD. Because the two are neurodegenerative disease,
researchers wanted to connect the two to see any correlation (Song). Parkinson’s patients develop
mental dysfunctions throughout the disease, which closely relates to Alzheimer’s disease (Song).
What researchers found was that although Parkinson’s disease patients could easily develop
forms of dementia, and especially Alzheimer’s, the majority of Alzheimer’s patients would not
develop any forms of Parkinson’s disease (Song).
Alzheimer’s disease has many different angles that researchers find baffling in their
discoveries. The possibility that AD may be a vascular disease, or any other sort of disease other
than a cognitive one is mind boggling. Alzheimer’s is a tricky disease, and because something
new is found all the time about it, it is hard to researchers to try and keep up with all the new
If a Loved One has Alzheimer’s, What are the Chances of Family Members Contracting it?
One of the scariest feelings is knowing that someone you love has Alzheimer’s. Many
people worry about when their loved one will forget who they are, where they live, etc. What
immediate family members start to worry about is their chances of being diagnosed with
Alzheimer’s when they get older. Since studying Alzheimer’s became extremely prevalent,
studying genetics and the possibility of Alzheimer’s being hereditary has become very frequent.
In my family, my mother and uncle have been worried about the possibility of becoming
diagnosed with Alzheimer’s because of my grandmother’s diagnosis. Yale-New Haven Hospital
aided my grandmother in treatments, and my family found that they are conducting studies on
immediate family members from Alzheimer’s patients to see if there is any correlation in
genetics for people to contract Alzheimer’s disease. For this study, patients must have had their
fiftieth birthday, and they make an appointment with Yale-New Haven to have this study
performed. The results though are for researchers purposes only. Therefore, if my mother were
to go to the test because her mother has Alzheimer’s, she would not find out if there was a
chance she would contract the disease as well. The doctors my family has met with have said
there is not a significant difference at this point in time about family becoming ill with
Alzheimer’s because of heredity. The possibility of someone with a family member with AD
being diagnosed with it is about less than 5% different from anyone who has not had a family
In one study by Aaron McMurtray, researchers learned any genetic background for a
possibility of Alzheimer’s. In this study, “investigators found a reduced familial risk for AD with
later ages of onset of the disease” (McMurtray). This is good news for those with family
members with AD- it is not entirely based on genetics. These studies were mainly included for
first-degree relatives (FDRs). They are people directly descended from Alzheimer’s patients. It
was found in this study that these FDRs would not generally become diagnosed with AD solely
because they have a parent or sibling with Alzheimer’s (McMurtray). All of the information
shows that genetics do not play a relatively large part in the diagnosis of Alzheimer’s disease.
Conclusion
Without the right information, anyone who does not know or understand Alzheimer’s disease can
be easily misinformed. Alzheimer’s can affect anyone at any point in time, whether it be
yourself, a family member or friend. The loss of one’s memory is detrimental, and the issues AD
can cause can be tragic. When treated correctly, or diagnosed early, patients and family can
prepare themselves through research. The media, reading about behaviors, and looking into
possible treatments can greatly prevent everyone from not knowing what can happen to a loved
one. With technology today and all the extensive research going on for Alzheimer’s research, in
the near future investigators may well be able to find ways to prevent, treat, and cure
Barton, Sally Ann. "Public Relations Plays Key Role In Launch of Alzheimer's Assays." Public Relations Quarterly 41.4 (1996): 33-35. Communication & Mass Media Complete. EBSCO. Web. 15 Nov. 2010.
Cassavetes, Nick, dir. The Notebook. Perf. Ryan Gosling, Rachel McAdams, Gena Rowlands and
James Garner. New Line Cinema. 25 June 2004. New Line Cinema. DVD. 30 October 2010.
Dede, Didem Sener, et al. "Assessment of endothelial function in Alzheimer's disease: Is
Alzheimer's disease a vascular disease?." Journal of the American Geriatrics Society 55.10 (2007): 1613-1617. Biological Abstracts. EBSCO. 10/2010. Web. 1 Nov. 2010.
“Drug Treatments for Alzheimer’s Disease.” Alzheimer’s Society. Alzheimer’s Society. Web. 25
Duberstein, Paul R., et al. "Personality and risk for Alzheimer's disease in adults 72 years of age
and older: A 6-year follow-up." Psychology and Aging (2010): PsycARTICLES. EBSCO. Web. 28 Oct. 2010.
Hori, Koji, et al. "First episodes of behavioral symptoms in Alzheimer's disease patients at age
90 and over, and early-onset Alzheimer's disease: comparison with senile dementia of Alzheimer's type." Psychiatry And Clinical Neurosciences 59.6 (2005): 730-735. MEDLINE with Full Text. EBSCO. Web. 7 Nov. 2010.
Konishi, Kimiko, et al. "Effects of aging on behavioral symptoms in Alzheimer's disease."
Psychogeriatrics 9.1 (2009): 11-16. PsycINFO. EBSCO. Web. 28 Oct. 2010.
McMurtray, Aaron M., et al. "Family history of dementia in early-onset versus very late-onset
Alzheimer's disease." International Journal of Geriatric Psychiatry 21.6 (2006): 597-598. Academic Search Premier. EBSCO. Web. 2 Nov. 2010. Morgan, Kathleen. "Risks of living with Alzheimer's disease: a personal view." Journal of Adult Protection 11.3 (2009): 26-29. SocINDEX with Full Text. EBSCO. Web. 1 Nov.2010.
Musicco, Massimo, et al. "Predictors of progression of cognitive decline in Alzheimer's disease:
the role of vascular and sociodemographic factors." Journal of Neurology 256.8 (2009): Biological Abstracts. EBSCO. Web. 1 Nov. 2010.
Pinson, Susan Moore, Kristen Register, and Amelia Roberts-Lewis. "Aging, Memory Loss,
Dementia, and Alzheimer's Disease: The Role of Christian Social Workers and the Church." Social Work & Christianity 37.2 (2010): 188-203. SocINDEX with Full Text. EBSCO. Web. 28 Oct. 2010.
Polley, Sarah, dir. Away From Her. Perf. Julie Christie, Gordon Pinsent and Olympia Dukakis.
Lionsgate, 2007. Lionsgate. DVD. 3 November 2010.
Reger, Beth. “Alzheimer's Disease: A Brief History and Avenues for Current Research.” Journal of Young Investigators. August 2002. Web. 2 November 2010.
Ringman, John M., and Jeffrey L. Cummings. "Current and emerging pharmacological treatment
options for dementia." Behavioural Neurology 17.1 (2006): 5-16. Academic Search Premier. EBSCO. Web. 12 November. 2010.
Song, In-Uk, et al. "Cognitive Dysfunctions in Mild Parkinson’s Disease Dementia: Comparison
with Patients Having Mild Alzheimer’s Disease and Normal Controls." European Neurology 59.1/2 (2008): 49-54. Academic Search Premier. EBSCO. Web. 15 Nov. 2010.
Stone, Anne, and Christina Jones. "Sources of Uncertainty: Experiences of Alzheimer's Disease."
Conference Papers -- National Communication Association (2008): 1. Communication & Mass Media Complete. EBSCO. Web. 15 Nov. 2010.
Wisniewski, Thomas, and Allal Boutajangout. "Vaccination as a therapeutic approach to
Alzheimer's disease." The Mount Sinai Journal Of Medicine, New York 77.1 (2010): 17-31. MEDLINE with Full Text. EBSCO. Web. 7 Nov. 2010.
Boletim do Serviço de Difusão - Nº 91 17 de Junho de 2013 Outros links: Sumário: JURISPRUDÊNCIA DO TJERJ: EDIÇÃO DE LEGISLAÇÃO* - Institui o Programa Estadual de Proteção da Criança e do Adolescente inseridos nas chamadas “Escolinhas de Futebol” e Atletas das Divisões de Base do Estado do Rio de Janeiro, e dá outras providências. Fonte: site da
Título: VARIANTE DIDÁCTICA DEL EXPERIMENTO DOCENTE EN LAS CIENCIAS NATURALES EXPERIMENTALES SUSTENTADO EN UN MODELO DIDÁCTICO INTEGRADOR PARA LA FORMACIÓN DE PROFESORES GENERALES INTEGRALES. Dr. C. Rolando Márquez Lizaso Profesor asistente de la facultad de Formación de Profesores Generales Integrales de Secundaria Básica del Instituto Superior Pedagógico "José Martí" d
 Introduction
Introduction