Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Microsoft word - 3 - therapeutic properties of periodontal cement packs.doc
The Therapeutic Properties of Periodontal Cement
by W J. LINGHORNE, D.D.S., Department of Physiology
D. C. O'CONNELL, M.S.A., Banting and Best Department of Medical Research,
experiments that may be of interest to the
Ipa cks have been increasingly used in the clinician are reported in this paper.
treatment of periodontal disease. Aided by
a grant to Dr. H. K. Box, Research Professor
together to form a paste. In the presence of
University of Toronto, from the Associate
moisture the paste sets, forming fairly hard
cement. Three formulae (see Appendix I),
National Research Council, an investigation
were selected as suitable for the various
of the therapeutic properties of periodontal
cement packs and their use in the treatment
periodontal case management. The products
of periodontal disease has been conducted in
differed mainly in the physical character of
the Banting and Best Department of Medical
Research, University of Toronto. It is hoped
through this study will result in a more
powders-zinc oxide, tannic acid, asbestos,
intelligent and effective clinical use of
properties of each were studied singly and in
therapeutic properties of periodontal cement
combination using the agar - plate - with -
packs and does not discuss the relationship
of this method of therapy to the various
sensitivity tests.1 (See Appendix II). The
tests were carried out against staphylococcus
application of the packing procedure to such
conditions as necrotic gingivitis, necrotic
of the test of the various ingredients in the
asbestos as a binder. The incubation period
rather than to attempt to describe any exact
clinical techniques based on the results of
the investigation, with the hope that the
specific information will be helpful to the
reader in evaluating and developing his own
materials. However, the three methods de-
scribed in the in- vivo studies were found to
be adequate in meeting most of the packing
problems encountered in periodontal case
was omitted but. asbestos was again used as
results when eugenol alone was used as the
then, upon further diffusion, may have been
subsequently killed. Accordingly, after two days
at room temperature following the initial 24'
Asbestos + Zinc Oxide + Eugenol. …………. 8
hours incubation at 37° C, five plates and one
control were re-inoculated with staphylococcus
aureus and re-incubated. No growth occurred in
any portion of any plate except the control plate.
Evidently diffusion had continued through-out
Acid + Resin + Eugenol ……………. 13
In order to ascertain for what length of
The next chart gives results using eugenol
time the active agent continued to diffuse from
15 parts and sweet almond oil 25 parts as. the
the pack, and whether the setting interfered with
the bacteriostatic action, the following studies
sweet almond oil and the same amount with
Asbestos + Zinc Oxide + Liquid . …………. 21
eugenol and thymol were placed on swab sticks,
(see Appendix IV), and dropped into 5 c.c. of
After one half-hour in the first tube the
pack had set and was transferred from tube to
Asbestos + Sweet Almond Oil gave an inhibition
eugenol and thymol (98 parts eugenol and 2 -
staphylococcus aureus and incubated at 37 Co for
24 and 28 hours. No growth occurred in any
The next question was whether the result
Asbestos + Zinc Oxide + liquid …….27
obtained was due to an agent on the surface or to
actual diffusion from the core of the pack.
Therefore in the next test, after the pack had been
allowed to harden in the first tube for 1/2 hour, it
was carried through a series of six washes in one
In all the plates showing inhibition there
hour, ten minutes in each tube and then carried
seemed to be two processes going on at the same
through two 1/2 hour tubes, two 1 hour tubes and
time, namely the diffusion of the bacteriostatic
one 24 hour tube. No growth appeared in any
agent through the agar and the growth of the
tube after 24 hours incubation. On 72 hours
organisms. Thus the question arose whether the
incubation, only the last four of the six wash
tubes showed evidence of growth. It appears,
bacteriostatic agent had diffused in the area and
then, that time for diffusion is necessary since a
10 minute interval is not always sufficient time
inhibited only, four tubes of fresh sterile broth
to ensure a bacteriostatic concentration.
coccus aureus had been killed or its growth
one of the half hour tubes in the dif-fusion series
and incubated at 37° C for 48 hours. No growth
occurred in any tube indicating that the
determine how long the pack would continue to
diffuse the active agent. It was carried out in
duplicate according to the method described
incubated for 24 hours, then removed and placed
in the next broth tube and incubated for 1 hour.
Following this, it was transferred to another tube
procedure was continued each day. Day by day
the tubes from which the pack had been removed
were seeded with staphylococcus organisms and
incubated for 24 hours. Up to the 35th day, no
growth occurred in either the 1 hour or the 24
hour tubes. This same pack in broth was set aside
in the laboratory for one year, during which time
the broth had evaporated to dryness. When the
pack was placed in broth for 1 hour, once again
In addition to the tests carried out against
sufficient of the bacteriostatic agent had diffused
the above pathogenic bacteria, a similar test was
made against candida albicans, the micro-
organism concerned in thrush. The zone of
inhibition produced against C, albicans was 20
bacteriostatic effect of the pack against other
mm, indicating that the pack has considerable
organisms. Using the agar-plate-with-well
technique (see Appendix III) the effect of the
Studies were carried out to investigate the
crococcus catarrhalis, staphylococcus aureus,
effect of packing periodontal pockets in humans
streptococcus viridans and streptococcus
teriostatic effect of the pack with that of pack +
periodontal pockets was placed on slides, care
sulphathiazole and pack + penicillin was made.
being taken to prevent maceration of the
The following chart gives the results of
organisms and it was allowed to dry in air. After
drying, the smears were examined under oil, at
least 30 fields being considered in thin
from the pocket were investigated: (1) using a
suitably shaped wooden toothpick, (2) a metal
probe and (3) a capillary tube pipette. The first
pack. The pack was again removed in 24 or 48
was the method selected and used throughout
hours. In a limited number of cases the pack was
these experiments. In each case the pocket area
allowed to remain in place for 4 to 7 days.
was isolated with cotton rolls, excess moisture
re-moved by blast of air, the toothpick was
suitably shaped and lightly scraped along the
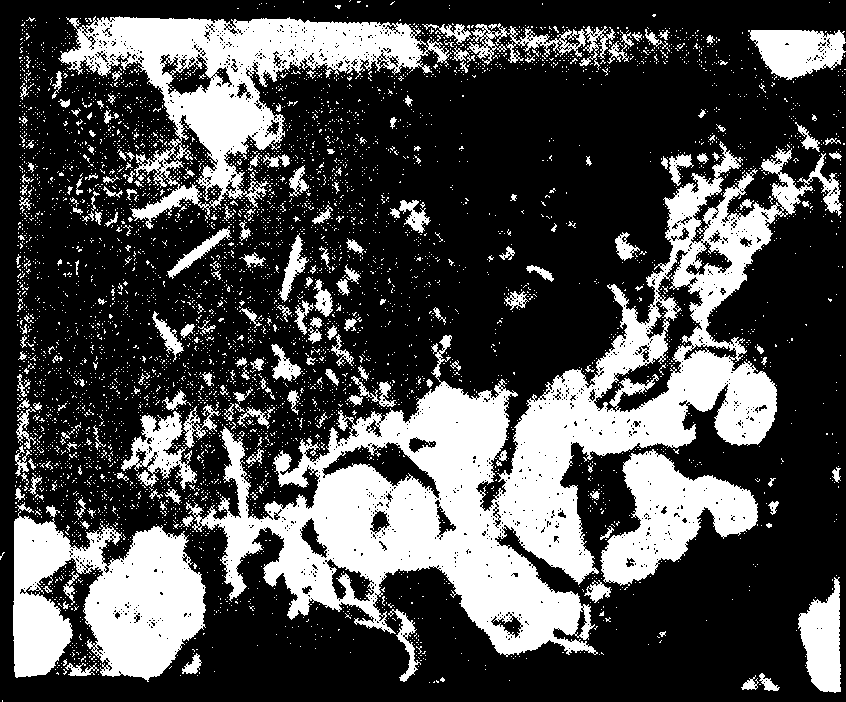
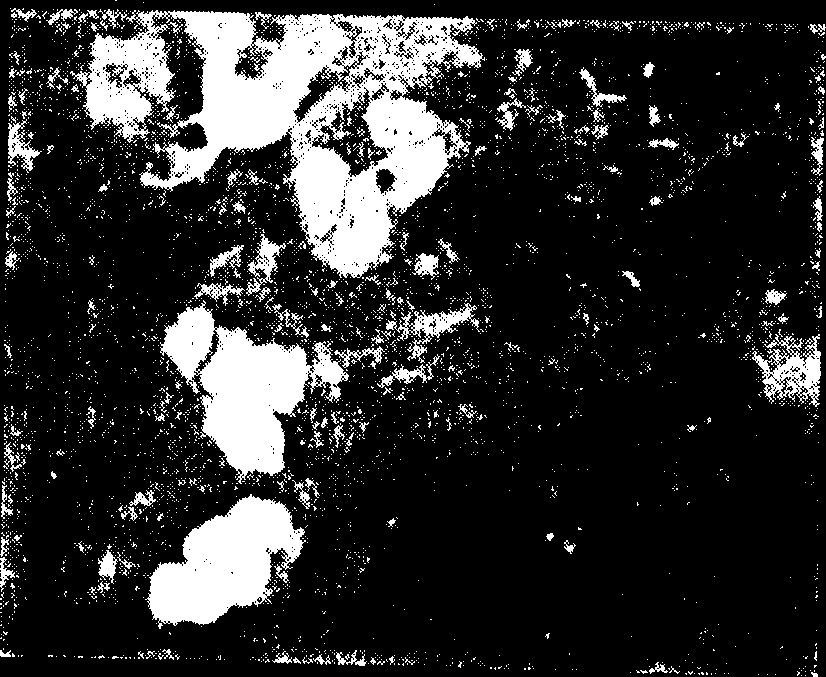
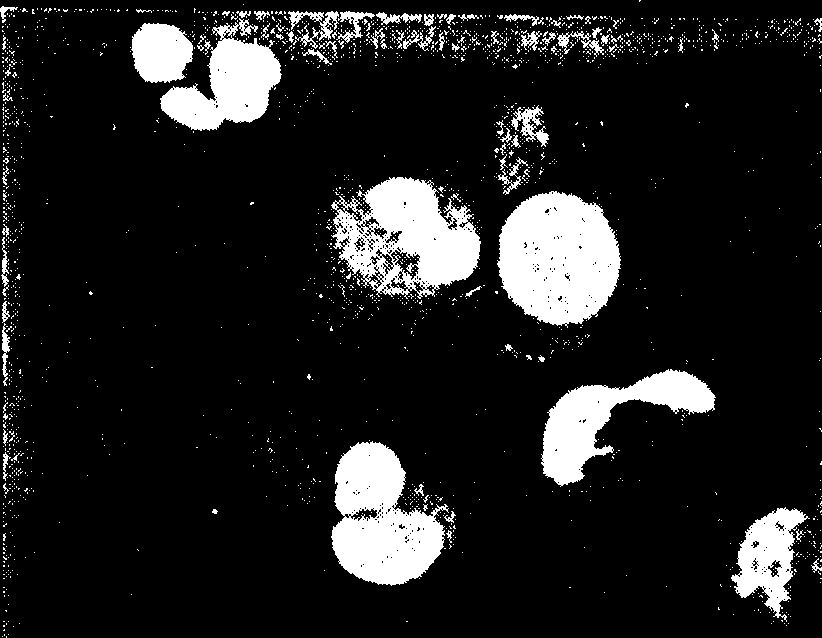
For practical purposes the microscopic findings
were divided into three groupings. Those smears
organisms of the fuso-spirochetal group were
found were called clinically sterile; those
showing one or two organisms per field were
called almost clinically sterile; and those smears
showing any of the group organisms in fair
numbers were called clinically septic. (See
photomicrograph 1, 2; and 3.) Smears were taken
before packing, after the pack had been in place
for various lengths of time and after the pocket
had been packed several times. Only those series
considered to have a bearing on clinical
determined by means of a probe graduated in
techniques for applying the pack were tried. .
Three were selected and used according to the
depth and course of the pocket and the nature of
Where it was possible to retract the soft
tissue wall to the base, Method I was used. A
mix of Formula 3 (See Appendix I) was made
introduced, a portion at a time, gradually, over-
filling the pocket. Each portion of pack was
sealed to the tooth and to the pack already
inserted, avoiding direct pressure on the soft
tissues. Finger pressure was used to mould the
overfilled portion to the tooth and to seal the
pocket. Only half of the mouth was packed at
one time and the patient was requested to avoid
chewing food where the teeth were packed. The
pack was removed in 24-48 hours, at which time
tuous, deep (over 6 mm.) or where the soft tissue
the pocket wall was often retracted to the base.
was dense and fibrous, Method II was used. A
Where considered necessary the pocket was
thin creamy mix of Formula I was made into
repacked, this operation being greatly facilitated
which shreds of -absorbent cotton were mixed.
by the opening up of the pocket by the preceding
Then, with a suitable instrument, this saturated
cotton was introduced into the pocket and very
Leaving the pack in place longer than 24
hours at a time made little difference. When the
lightly tamped until the, pocket was three
longer than 48 hours it was often loosened or
quarters filled. The y pocket was then overfilled
with a stiffer mix of formula III which was
The following table gives the results of
moulded around the tooth using finger pressure
packing experimentally produced periodontal
into place using finger pressure and instruments,
a mix of Formula II, which would flow under
active agent in the pack into close contact with,
the bacteria at the base of the pocket. Box, in his
paper "Necrotic Gingivitis' 2' pointed out that
All pockets were clinically septic before,
taking into account the questions of extreme
pocket thinness, viscosity of the pocket fluids
and the presence of calcific deposits which, serve
The in vivo studies indicated 'that the cement
to interfere with great mass movements through
packs selected are highly effective in combating
constrictions etc., it wcu1d appear that
the organisms of the periodontal pocket. The an
convection currents have little bearing on the
vitro studies show that the pack is bacteriostatic
oxygen distribution in the pocket. Constrictions
would slow the rate of penetration of the pocket
organisms and that under certain conditions this
by diffusion also. Thus in order to permit the
effect is maintained for a far longer time than is
diffusion through-out the pocket of the, active
required clinically in pocket therapy. Thus the
agent in, the pack, either the soft tissue wall must
pocket can be kept clinically sterile for at least a
be retracted to the base, or the pocket must be
However, as pointed out before in this paper, in
The following table gives the results of
order that the active agent be brought into
packing periodontal pockets in humans. Only,
contact with all the organisms in sufficient
those cases where the pack remained firmly in
concentration for the required time, it appears
place were included. All pockets were found to
necessary that either the pocket be packed in
such a way that the soft tissue wall is retracted to
the base, or that the pocket be filled to the base
conditions were such that the pockets could be
packed to the base, all were found to be clinically
sterile in 24 hours. Also, in human periodontal
pockets a much higher percentage was found to
be clinically sterile following second packing
than when only one pack was used. This is to be
expected as the opening up of the pocket by the
first pack greatly facilitated the, second packing.
In order to meet the various requirements in
formulae, varying mainly in the physical
mix, are suggested. The mix of Formula I is thick
and creamy and might be described as a paint. It
is sticky and adheres well to the teeth and
mucous membrane. The mix of Formula II is
stiffer and more fibrous but will flow under
finger pressure. It is less sticky than that of
(1) In vitro studies indicate that the periodontal
Formula I. The mix of Formula III might be
packing material studied is an effective
compared to the consistency of putty. When
bacteriostatic agent against staphylococcus
applied it will displace the tissues and hold them
aureus, streptococcus viridans, streptococcus
displaced until setting of the pack occurs. It is
hemolyticus, and micrococcus catarrhalis.
not sticky but can be made to adhere to the tooth
(2) In vivo studies indicate that the pack is an
and to other portions of pack. When set it is
softer and less brittle than the mix of either of the
(3) Diffusion of the bacteriostatic agent from the
pack into the surrounding media will continue
for a far longer time than is required in perio-
appears to be largely due to the eugenol and
thymol. The addition of thymol seems to increase
(4) The periodontal pack acts as a stimulant and
the bacteriostatic effect. - Sweet almond oil
slows the setting time and reduces stickiness. It
(5) The addition of 5% sulphathiazole or of
is omitted in Formula I and I as stickiness and
penicillin (5000 units to 5 grams of pack) does
quick setting are desirable properties when used
(6) The pack is an effective fungicide against
eugenol and thymol are stimulants and local
candida albicans, the organism concerned in
analgesics. When the pack is applied to tender or
painful surfaces, the patient experiences almost
immediate relief, also, there is a marked
beneficial effect on the tissues observed
clinically within 24 hours of the application of
The pack is fairly insoluble in water but
dissolves readily in alcohol. This fact is made
The addition of 5% sulphathiazole or penicillin
(5000 units to 5 grams of pack) does not appear
to enhance the bacteriostatic effects of the pack
The in vitro test against candida albicans, the
fungus concerned in thrush, suggests that the
This technique consists of cutting a well
in the centre of a poured agar plate which has
been previously inoculated with the test
organism and then filling the well with the
plate is incubated at 37° C for 24 to 48 hours.
The inhibition produced is the width of the
annulus obtained, measured in millimetres
(distance from edge of well to bacterial growth
just beyond zone of no growth). Beyond the zone
of inhibition, the test organism should grow well
and there by provide a control for the test.
tested by this technique and duplica-tion requires
determination of inhibition produced by cement
Swab stick technique for the determination of the
or paste-like materials against bacteria.
effects of setting and time for diffusion on the
narrow trough or gutter through the centre of a
poured agar plate and then filling this cut with
batch of pack (5 gms.) and placing it around the
end of a medium sized swab stick, and then
The test organisms are then streak-ed up
placing it in a culture tube containing 5 c.c. of a
to, but not across the edge of the gutter. After
inoculation the plates are incubated at 37° C for
The pack will harden in about one hour in
liquid and will continue to dif-fuse the active
The inhibition produced is the distance in
ingredient for considerable lengths of time. Once
millimetres measured from the edge of the
the pack has hardened on the stick it may be
trough out to the first pin point colonies growing
transferred from tube to tube as required, making
along the line of inoculation. Beyond the zone of
it possible to study rates of diffusion of the active
inhibition the test organism should grow well
agent from the pack into the surrounding culture
and by so doing provides a control for the test.
close together, one organism may be streaked
the tubed and treated medium may be inoculated
several times on one plate or several organisms
may be streaked on the same plate, thereby
(1) Fleming, A. 1929. Brit. J. Exp. Path. 10-226.
(2) Box, Harold Keith. D.D.S. Ph.D. Necrotic Gingivitis,
(3) Zinsser, H. and Bayne-Jones, S. Text book of
determination of inhibition produced by cement
Bacteriology Chapter LXXIII. 8th ed. 1989.
or paste-like materials against a single
This work was initiated am a result of the conception of the pathogenesis of periodontal disease
recently presented by Dr. S. K. Box, in which the importance of pocket therapy even in the early
stages of periodontal disease, is emphasized. The authors owe a debt of gratitude to Dr. Box for
valuable Information on this problem an it relates to periodontal disease.
The authors also wish to acknowledge their Indebtedness to Dr. C. H. Best and to Dr, C. C. Lucas
for helpful suggestions and advice on certain phases of the problem.
 probe and (3) a capillary tube pipette. The first
pack. The pack was again removed in 24 or 48
was the method selected and used throughout
hours. In a limited number of cases the pack was
these experiments. In each case the pocket area
allowed to remain in place for 4 to 7 days.
was isolated with cotton rolls, excess moisture
re-moved by blast of air, the toothpick was
suitably shaped and lightly scraped along the
For practical purposes the microscopic findings
were divided into three groupings. Those smears
organisms of the fuso-spirochetal group were
found were called clinically sterile; those
showing one or two organisms per field were
called almost clinically sterile; and those smears
showing any of the group organisms in fair
numbers were called clinically septic. (See
photomicrograph 1, 2; and 3.) Smears were taken
before packing, after the pack had been in place
for various lengths of time and after the pocket
had been packed several times. Only those series
considered to have a bearing on clinical
determined by means of a probe graduated in
techniques for applying the pack were tried. .
Three were selected and used according to the
depth and course of the pocket and the nature of
Where it was possible to retract the soft
tissue wall to the base, Method I was used. A
mix of Formula 3 (See Appendix I) was made
introduced, a portion at a time, gradually, over-
filling the pocket. Each portion of pack was
sealed to the tooth and to the pack already
inserted, avoiding direct pressure on the soft
tissues. Finger pressure was used to mould the
overfilled portion to the tooth and to seal the
pocket. Only half of the mouth was packed at
one time and the patient was requested to avoid
chewing food where the teeth were packed. The
pack was removed in 24-48 hours, at which time
tuous, deep (over 6 mm.) or where the soft tissue
the pocket wall was often retracted to the base.
was dense and fibrous, Method II was used. A
Where considered necessary the pocket was
thin creamy mix of Formula I was made into
repacked, this operation being greatly facilitated
which shreds of -absorbent cotton were mixed.
by the opening up of the pocket by the preceding
Then, with a suitable instrument, this saturated
cotton was introduced into the pocket and very
Leaving the pack in place longer than 24
hours at a time made little difference. When the
lightly tamped until the, pocket was three
longer than 48 hours it was often loosened or
quarters filled. The y pocket was then overfilled
with a stiffer mix of formula III which was
The following table gives the results of
moulded around the tooth using finger pressure
packing experimentally produced periodontal
into place using finger pressure and instruments,
a mix of Formula II, which would flow under
active agent in the pack into close contact with,
the bacteria at the base of the pocket. Box, in his
paper "Necrotic Gingivitis' 2' pointed out that
All pockets were clinically septic before,
taking into account the questions of extreme
pocket thinness, viscosity of the pocket fluids
and the presence of calcific deposits which, serve
The in vivo studies indicated 'that the cement
to interfere with great mass movements through
packs selected are highly effective in combating
constrictions etc., it wcu1d appear that
the organisms of the periodontal pocket. The an
convection currents have little bearing on the
vitro studies show that the pack is bacteriostatic
oxygen distribution in the pocket. Constrictions
would slow the rate of penetration of the pocket
organisms and that under certain conditions this
by diffusion also. Thus in order to permit the
effect is maintained for a far longer time than is
diffusion through-out the pocket of the, active
required clinically in pocket therapy. Thus the
agent in, the pack, either the soft tissue wall must
pocket can be kept clinically sterile for at least a
be retracted to the base, or the pocket must be
However, as pointed out before in this paper, in
The following table gives the results of
order that the active agent be brought into
packing periodontal pockets in humans. Only,
contact with all the organisms in sufficient
those cases where the pack remained firmly in
concentration for the required time, it appears
place were included. All pockets were found to
necessary that either the pocket be packed in
such a way that the soft tissue wall is retracted to
the base, or that the pocket be filled to the base
conditions were such that the pockets could be
packed to the base, all were found to be clinically
sterile in 24 hours. Also, in human periodontal
pockets a much higher percentage was found to
be clinically sterile following second packing
than when only one pack was used. This is to be
expected as the opening up of the pocket by the
first pack greatly facilitated the, second packing.
In order to meet the various requirements in
formulae, varying mainly in the physical
mix, are suggested. The mix of Formula I is thick
and creamy and might be described as a paint. It
is sticky and adheres well to the teeth and
mucous membrane. The mix of Formula II is
stiffer and more fibrous but will flow under
finger pressure. It is less sticky than that of
(1) In vitro studies indicate that the periodontal
Formula I. The mix of Formula III might be
packing material studied is an effective
compared to the consistency of putty. When
bacteriostatic agent against staphylococcus
applied it will displace the tissues and hold them
aureus, streptococcus viridans, streptococcus
displaced until setting of the pack occurs. It is
hemolyticus, and micrococcus catarrhalis.
not sticky but can be made to adhere to the tooth
(2) In vivo studies indicate that the pack is an
and to other portions of pack. When set it is
softer and less brittle than the mix of either of the
(3) Diffusion of the bacteriostatic agent from the
pack into the surrounding media will continue
for a far longer time than is required in perio-
appears to be largely due to the eugenol and
thymol. The addition of thymol seems to increase
(4) The periodontal pack acts as a stimulant and
the bacteriostatic effect. - Sweet almond oil
slows the setting time and reduces stickiness. It
(5) The addition of 5% sulphathiazole or of
is omitted in Formula I and I as stickiness and
penicillin (5000 units to 5 grams of pack) does
quick setting are desirable properties when used
(6) The pack is an effective fungicide against
eugenol and thymol are stimulants and local
candida albicans, the organism concerned in
analgesics. When the pack is applied to tender or
painful surfaces, the patient experiences almost
immediate relief, also, there is a marked
beneficial effect on the tissues observed
clinically within 24 hours of the application of
The pack is fairly insoluble in water but
dissolves readily in alcohol. This fact is made
The addition of 5% sulphathiazole or penicillin
(5000 units to 5 grams of pack) does not appear
to enhance the bacteriostatic effects of the pack
The in vitro test against candida albicans, the
fungus concerned in thrush, suggests that the
This technique consists of cutting a well
in the centre of a poured agar plate which has
been previously inoculated with the test
organism and then filling the well with the
plate is incubated at 37° C for 24 to 48 hours.
The inhibition produced is the width of the
annulus obtained, measured in millimetres
(distance from edge of well to bacterial growth
just beyond zone of no growth). Beyond the zone
of inhibition, the test organism should grow well
and there by provide a control for the test.
tested by this technique and duplica-tion requires
determination of inhibition produced by cement
Swab stick technique for the determination of the
or paste-like materials against bacteria.
effects of setting and time for diffusion on the
narrow trough or gutter through the centre of a
poured agar plate and then filling this cut with
batch of pack (5 gms.) and placing it around the
end of a medium sized swab stick, and then
The test organisms are then streak-ed up
placing it in a culture tube containing 5 c.c. of a
to, but not across the edge of the gutter. After
inoculation the plates are incubated at 37° C for
The pack will harden in about one hour in
liquid and will continue to dif-fuse the active
The inhibition produced is the distance in
ingredient for considerable lengths of time. Once
millimetres measured from the edge of the
the pack has hardened on the stick it may be
trough out to the first pin point colonies growing
transferred from tube to tube as required, making
along the line of inoculation. Beyond the zone of
it possible to study rates of diffusion of the active
inhibition the test organism should grow well
agent from the pack into the surrounding culture
and by so doing provides a control for the test.
close together, one organism may be streaked
the tubed and treated medium may be inoculated
several times on one plate or several organisms
may be streaked on the same plate, thereby
(1) Fleming, A. 1929. Brit. J. Exp. Path. 10-226.
(2) Box, Harold Keith. D.D.S. Ph.D. Necrotic Gingivitis,
(3) Zinsser, H. and Bayne-Jones, S. Text book of
determination of inhibition produced by cement
Bacteriology Chapter LXXIII. 8th ed. 1989.
or paste-like materials against a single
This work was initiated am a result of the conception of the pathogenesis of periodontal disease
recently presented by Dr. S. K. Box, in which the importance of pocket therapy even in the early
stages of periodontal disease, is emphasized. The authors owe a debt of gratitude to Dr. Box for
valuable Information on this problem an it relates to periodontal disease.
The authors also wish to acknowledge their Indebtedness to Dr. C. H. Best and to Dr, C. C. Lucas
for helpful suggestions and advice on certain phases of the problem.
probe and (3) a capillary tube pipette. The first
pack. The pack was again removed in 24 or 48
was the method selected and used throughout
hours. In a limited number of cases the pack was
these experiments. In each case the pocket area
allowed to remain in place for 4 to 7 days.
was isolated with cotton rolls, excess moisture
re-moved by blast of air, the toothpick was
suitably shaped and lightly scraped along the
For practical purposes the microscopic findings
were divided into three groupings. Those smears
organisms of the fuso-spirochetal group were
found were called clinically sterile; those
showing one or two organisms per field were
called almost clinically sterile; and those smears
showing any of the group organisms in fair
numbers were called clinically septic. (See
photomicrograph 1, 2; and 3.) Smears were taken
before packing, after the pack had been in place
for various lengths of time and after the pocket
had been packed several times. Only those series
considered to have a bearing on clinical
determined by means of a probe graduated in
techniques for applying the pack were tried. .
Three were selected and used according to the
depth and course of the pocket and the nature of
Where it was possible to retract the soft
tissue wall to the base, Method I was used. A
mix of Formula 3 (See Appendix I) was made
introduced, a portion at a time, gradually, over-
filling the pocket. Each portion of pack was
sealed to the tooth and to the pack already
inserted, avoiding direct pressure on the soft
tissues. Finger pressure was used to mould the
overfilled portion to the tooth and to seal the
pocket. Only half of the mouth was packed at
one time and the patient was requested to avoid
chewing food where the teeth were packed. The
pack was removed in 24-48 hours, at which time
tuous, deep (over 6 mm.) or where the soft tissue
the pocket wall was often retracted to the base.
was dense and fibrous, Method II was used. A
Where considered necessary the pocket was
thin creamy mix of Formula I was made into
repacked, this operation being greatly facilitated
which shreds of -absorbent cotton were mixed.
by the opening up of the pocket by the preceding
Then, with a suitable instrument, this saturated
cotton was introduced into the pocket and very
Leaving the pack in place longer than 24
hours at a time made little difference. When the
lightly tamped until the, pocket was three
longer than 48 hours it was often loosened or
quarters filled. The y pocket was then overfilled
with a stiffer mix of formula III which was
The following table gives the results of
moulded around the tooth using finger pressure
packing experimentally produced periodontal
into place using finger pressure and instruments,
a mix of Formula II, which would flow under
active agent in the pack into close contact with,
the bacteria at the base of the pocket. Box, in his
paper "Necrotic Gingivitis' 2' pointed out that
All pockets were clinically septic before,
taking into account the questions of extreme
pocket thinness, viscosity of the pocket fluids
and the presence of calcific deposits which, serve
The in vivo studies indicated 'that the cement
to interfere with great mass movements through
packs selected are highly effective in combating
constrictions etc., it wcu1d appear that
the organisms of the periodontal pocket. The an
convection currents have little bearing on the
vitro studies show that the pack is bacteriostatic
oxygen distribution in the pocket. Constrictions
would slow the rate of penetration of the pocket
organisms and that under certain conditions this
by diffusion also. Thus in order to permit the
effect is maintained for a far longer time than is
diffusion through-out the pocket of the, active
required clinically in pocket therapy. Thus the
agent in, the pack, either the soft tissue wall must
pocket can be kept clinically sterile for at least a
be retracted to the base, or the pocket must be
However, as pointed out before in this paper, in
The following table gives the results of
order that the active agent be brought into
packing periodontal pockets in humans. Only,
contact with all the organisms in sufficient
those cases where the pack remained firmly in
concentration for the required time, it appears
place were included. All pockets were found to
necessary that either the pocket be packed in
such a way that the soft tissue wall is retracted to
the base, or that the pocket be filled to the base
conditions were such that the pockets could be
packed to the base, all were found to be clinically
sterile in 24 hours. Also, in human periodontal
pockets a much higher percentage was found to
be clinically sterile following second packing
than when only one pack was used. This is to be
expected as the opening up of the pocket by the
first pack greatly facilitated the, second packing.
In order to meet the various requirements in
formulae, varying mainly in the physical
mix, are suggested. The mix of Formula I is thick
and creamy and might be described as a paint. It
is sticky and adheres well to the teeth and
mucous membrane. The mix of Formula II is
stiffer and more fibrous but will flow under
finger pressure. It is less sticky than that of
(1) In vitro studies indicate that the periodontal
Formula I. The mix of Formula III might be
packing material studied is an effective
compared to the consistency of putty. When
bacteriostatic agent against staphylococcus
applied it will displace the tissues and hold them
aureus, streptococcus viridans, streptococcus
displaced until setting of the pack occurs. It is
hemolyticus, and micrococcus catarrhalis.
not sticky but can be made to adhere to the tooth
(2) In vivo studies indicate that the pack is an
and to other portions of pack. When set it is
softer and less brittle than the mix of either of the
(3) Diffusion of the bacteriostatic agent from the
pack into the surrounding media will continue
for a far longer time than is required in perio-
appears to be largely due to the eugenol and
thymol. The addition of thymol seems to increase
(4) The periodontal pack acts as a stimulant and
the bacteriostatic effect. - Sweet almond oil
slows the setting time and reduces stickiness. It
(5) The addition of 5% sulphathiazole or of
is omitted in Formula I and I as stickiness and
penicillin (5000 units to 5 grams of pack) does
quick setting are desirable properties when used
(6) The pack is an effective fungicide against
eugenol and thymol are stimulants and local
candida albicans, the organism concerned in
analgesics. When the pack is applied to tender or
painful surfaces, the patient experiences almost
immediate relief, also, there is a marked
beneficial effect on the tissues observed
clinically within 24 hours of the application of
The pack is fairly insoluble in water but
dissolves readily in alcohol. This fact is made
The addition of 5% sulphathiazole or penicillin
(5000 units to 5 grams of pack) does not appear
to enhance the bacteriostatic effects of the pack
The in vitro test against candida albicans, the
fungus concerned in thrush, suggests that the
This technique consists of cutting a well
in the centre of a poured agar plate which has
been previously inoculated with the test
organism and then filling the well with the
plate is incubated at 37° C for 24 to 48 hours.
The inhibition produced is the width of the
annulus obtained, measured in millimetres
(distance from edge of well to bacterial growth
just beyond zone of no growth). Beyond the zone
of inhibition, the test organism should grow well
and there by provide a control for the test.
tested by this technique and duplica-tion requires
determination of inhibition produced by cement
Swab stick technique for the determination of the
or paste-like materials against bacteria.
effects of setting and time for diffusion on the
narrow trough or gutter through the centre of a
poured agar plate and then filling this cut with
batch of pack (5 gms.) and placing it around the
end of a medium sized swab stick, and then
The test organisms are then streak-ed up
placing it in a culture tube containing 5 c.c. of a
to, but not across the edge of the gutter. After
inoculation the plates are incubated at 37° C for
The pack will harden in about one hour in
liquid and will continue to dif-fuse the active
The inhibition produced is the distance in
ingredient for considerable lengths of time. Once
millimetres measured from the edge of the
the pack has hardened on the stick it may be
trough out to the first pin point colonies growing
transferred from tube to tube as required, making
along the line of inoculation. Beyond the zone of
it possible to study rates of diffusion of the active
inhibition the test organism should grow well
agent from the pack into the surrounding culture
and by so doing provides a control for the test.
close together, one organism may be streaked
the tubed and treated medium may be inoculated
several times on one plate or several organisms
may be streaked on the same plate, thereby
(1) Fleming, A. 1929. Brit. J. Exp. Path. 10-226.
(2) Box, Harold Keith. D.D.S. Ph.D. Necrotic Gingivitis,
(3) Zinsser, H. and Bayne-Jones, S. Text book of
determination of inhibition produced by cement
Bacteriology Chapter LXXIII. 8th ed. 1989.
or paste-like materials against a single
This work was initiated am a result of the conception of the pathogenesis of periodontal disease
recently presented by Dr. S. K. Box, in which the importance of pocket therapy even in the early
stages of periodontal disease, is emphasized. The authors owe a debt of gratitude to Dr. Box for
valuable Information on this problem an it relates to periodontal disease.
The authors also wish to acknowledge their Indebtedness to Dr. C. H. Best and to Dr, C. C. Lucas
for helpful suggestions and advice on certain phases of the problem.