Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Mypcos.info
P a t h o p h y s i o l o g y / C o m p l i c a t i o n s O R I G I N A L Altered D-Chiro-Inositol Urinary Clearance in Women With Polycystic Ovary Syndrome EAN-PATRICE BAILLARGEON, MD, MSC TEIMURAZ APRIDONIDZE, MD VANTHIA DIAMANTI-KANDARAKIS, MD MARIA J. IUORNO, MD ICHARD E. OSTLUND, JR., MD JOHN E. NESTLER, MD
zone (3), and D-chiro-inositol (DCI)(10 –12), to both obese and lean womenwith the syndrome increases the fre-
OBJECTIVE — Evidence suggests that some actions of insulin are effected by inositolphos-
phoglycan (IPG) mediators. We hypothesize that a deficiency in D-chiro-inositol (DCI) and/or a
DCI-containing IPG (DCI-IPG) may contribute to insulin resistance in humans. RESEARCH DESIGN AND METHODS — To assess this possibility in polycystic ovary
(IPG) mediators of insulin action (13,14),
syndrome (PCOS), we determined insulin sensitivity (S by frequently sampled intravenous
and evidence suggests that a deficiency in
glucose tolerance test), plasma and urinary DCI and myo-inositol (MYO) levels (by gas chroma-tography/mass spectrometry), and the release of insulin and DCI-IPG during the oral glucose
tolerance test (area under the curve [AUC]) in 23 women with PCOS and 26 normal women.
phoglycan (DCI-IPG) may contribute toinsulin resistance in individuals with im-
RESULTS — Women with PCOS were heavier than control subjects (P ϭ 0.002 for BMI), but
paired glucose tolerance or type 2 diabe-
also had decreased S (P Ͻ 0.001) and increased AUC
women, even when corrected for BMI. The urinary clearance of DCI (uCl
suggest that a deficiency in DCI-IPG con-
almost sixfold in PCOS compared with normal women (P ϭ 0.001), but not MYO clearance (P ϭ
tributes to insulin resistance in PCOS as
correlated inversely with S when all women were analyzed together (n ϭ 49, r ϭ
0.50, P Ͻ 0.001) and was one of the three best independent parameters predicting S . Finally,
was decreased threefold in women with PCOS (P Ͻ 0.001). CONCLUSIONS — uCl
is inversely correlated with insulin sensitivity in women and is a
strong independent predictor of insulin resistance in multivariate models. PCOS, which is
characterized by insulin resistance, is associated with a selective increase in uCl
DCI-IPG release in response to insulin. These findings are consistent with a defect in tissue
availability or utilization of DCI in PCOS that may contribute to the insulin resistance of the
tion. The idea that a deficiency in DCI-IPG, related perhaps to an actual or
Diabetes Care 29:300 –305, 2006
functional deficiency of the precursorDCI, contributes to the insulin resistance
Polycysticovarysyndrome(PCOS)is oping cancer, hypertension, dyslipide- ofPCOSisfurthersupportedbyevidence
mia, impaired glucose tolerance or type 2
P C O S w o m e n e n h a n c e s i n s u l i n -
evidence supports the central role of in-
sized that a defect in an alternative insu-
6 –10% of women of childbearing age (3–
acts as a mediator of insulin action, con-
tributes to the pathophysiology of the in-
anovulatory infertility in the U.S. and is
associated with an increased risk of devel-
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
From the 1Department of Medicine, Universite´ de Sherbrooke, Sherbrooke, Canada; the 2First Department
of Medicine–Endocrine Section, University of Athens Medical School, Athens, Greece; the 3Department of
Medicine, Washington University School of Medicine, St. Louis, Missouri; the 4Department of Medicine,
release of the putative DCI-IPG mediator.
Virginia Commonwealth University, Richmond, Virginia; and the 5Department of Obstetrics and Gynecol-
ogy, Virginia Commonwealth University, Richmond, Virginia.
Address correspondence and reprint requests to Jean-Patrice Baillargeon, MD, MSc, Universite´ de Sher-
brooke, Sherbrooke, QC J1H 5N4, Canada. E-mail: jp.baillargeon@usherbrooke.ca.
Received for publication 10 June 2005 and accepted in revised form 23 October 2005. Abbreviations: AUC
, area under the bioactivity curve for DCI-IPG during OGTT; AUC
under the insulin curve during OGTT; DCI, D-chiro-inositol; DCI-IPG, DCI-containing inositolphosphogly-
can; IPG, inositolphosphoglycan; MYO, myo-inositol; OGTT, oral glucose tolerance test; PCOS, polycysticovary syndrome; uCl
, urinary clearance of D-chiro-inositol; WHR, waist-to-hip ratio.
A table elsewhere in this issue shows conventional and Syste`me International (SI) units and conversion
technique. As a control, we also assessed
the urinary clearance of myo-inositol
2006 by the American Diabetes Association.
(MYO), an inositol not believed to influ-
The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be herebymarked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
ence insulin sensitivity. The findings indi-
DIABETES CARE, VOLUME 29, NUMBER 2, FEBRUARY 2006
Baillargeon and Associates
the specific activation of phosphate dehy-
clearance and deficient insulin-stimulated
intravenous glucose tolerance test as de-
drogenase phosphatase, as previously val-
scribed by Bergman and colleagues (18 –
20). At time zero, 300 mg/kg dextrose was
RESEARCH DESIGN AND
venously 20 min later. A total of 27 blood
METHODS — A total of 23 women
glucose were collected over the 3-h dura-
8.5%, respectively, for the absolute values
jects were evaluated at the General Clini-
of basal and peak DCI-IPG bioactivity.
Commonwealth University Health System.
assay to the other, and therefore from sub-
nation of tissue insulin sensitivity (Si).
ject to subject, the water-blank activity
(elevated serum total or free testosterone
ately, and sera were stored at Ϫ70°C until
percentage of its bioactivity at baseline (0
previously described (22–24). Serum free
known to affect insulin sensitivity for at
lin concentrations and relative bioactivi-
(40 g/l). To avoid interassay variation, all
ties of DCI-IPG to the oral administration
of glucose by calculating the areas under
strual cycles, normal androgen levels, and
single assay for each hormone. The intra-
assay coefficient of variation (CV) for the
trapezoidal rule. Results not normally dis-
have any history of gestational diabetes or
family history of a first-degree relative
with diabetes. They were free of disorders
tance, such as hypertension or dyslipide-
results are reported as means, or geomet-
with 95% CIs. P values Ͻ0.05 were con-
[2H6]racemic chiro-inositol and [2H6]myo-
sidered significant. All analyses were per-
woman gave written informed consent.
inositol were added to plasma or urine as
then purified, derivatized with pentaflu-
groups were made with the Student’s two-
diet high in legumes or fruits, the women
tailed t test, and equalities of variances
State College, PA), and analyzed in a neg-
were tested with the Brown-Forsythe test.
anced mixed diet for at least 3 days before
P values of Welch ANOVA tests were re-
studied during the equivalent of the fol-
ported, as indicated. Correlation analysis
ane as the reagent gas, as previously re-
tion test. Correction for BMI and/or Si was
performed with multiple linear regression
lieu of anovulatory women with PCOS.
ately, and sera were stored at Ϫ70°C until
scribed (17). To date, it has not been pos-
both. BMI status was categorized as obese
sible to measure the content of extracted
to collect all their urine for the next 24 h.
first one, the dependant variable was DCI
urinary clearance, the exposition variable
DIABETES CARE, VOLUME 29, NUMBER 2, FEBRUARY 2006
Altered DCI urinary clearance in PCOS Table 1 —Clinical and biochemical characteristics of women with PCOS and normal control women
Data are means (95% CIs) unless otherwise indicated. To convert values for total testosterone to nanomoles per liter, multiply by 0.0347; to convert values for freetestosterone to picomoles per liter, multiply by 34.7; and to convert values for insulin to picomoles per liter, multiply by 6.9. Note that only significant partial P values(‡, §, or ʈ) after correction for BMI and/or S are reported (multiple linear regression analyses). FSIVGGT, frequently sampled intravenous glucose tolerance test.
*Unequal variance t test. †Geometric means. ‡P Ͻ 0.05 when corrected for BMI and S . §P Ͻ 0.05 when corrected for BMI. ʈP Ͻ 0.05 when corrected for S .
significantly to the model (partial P Ͻ
with normal control subjects (P ϭ 0.035),
significantly higher (P ϭ 0.043) (Table 1).
testosterone, and Si. These confounders
were selected based on scientific literature
and because they were significantly asso-
was highly significant (P Ͻ 0.001). This
ciated with the dependant variable in uni-
statistical significance persisted even after
variate analyses. To assess the effect of
correction for BMI (P ϭ 0.015). In con-
on next highest partial F test (forward
tested with each new variables added into
concentrations, 24-h urinary excretion of
MYO, and urinary clearance of MYO (P Ն
levels were significantly higher in women
analysis, the dependant variable was S
with PCOS than in control women (P Ͻ
0.001), even after correction for BMI and
Si (P ϭ 0.006 and P Ͻ 0.001, respec-
tively). Furthermore, fasting insulin levels
independently of obesity (P ϭ 0.006), a
and total testosterone. These confounders
(P ϭ 0.047) and areas under the insulin
were also significantly associated with the
curves during OGTT (AUCinsulin) (P Ͻ
dependant variable in univariate analyses.
PCOS status (P ϭ 0.02), and a significant
in normal control subjects, and Si values
were significantly lower (P Ͻ 0.001).
obesity (P ϭ 0.005). To illustrate this in-
AUCinsulin and Si remained significantly
different between groups after correction
analysis, the best model to predict S
for BMI (P ϭ 0.001 and P ϭ 0.002, re-
significantly increased by 14-fold in obese
assessed using all variables of Table 1.
found with the first two stepwise regres-
[13.1–77.2] vs. 2.2 [0.7–7.3], P Ͻ
0.001), even after correction for Si and
Plasma concentrations of DCI were signif-
total testosterone (partial P ϭ 0.003). No
DIABETES CARE, VOLUME 29, NUMBER 2, FEBRUARY 2006
Baillargeon and Associates
(partial P ϭ 0.001). This interaction hasalready been explained above. CONCLUSIONS — The aim of this study was to test the hypothesis that women with PCOS would exhibit abnor- mal metabolism of DCI and deficient in- sulin-stimulated release of DCI-IPG, which would correlate with their de- creased sensitivity to insulin. Indeed, we found that women with PCOS, when compared with normal control women, had a greater than fivefold increase in uClDCI and a circulating concentration of DCI that was reduced by half. These ab- normalities persisted even when cor- rected for differences in BMI between the
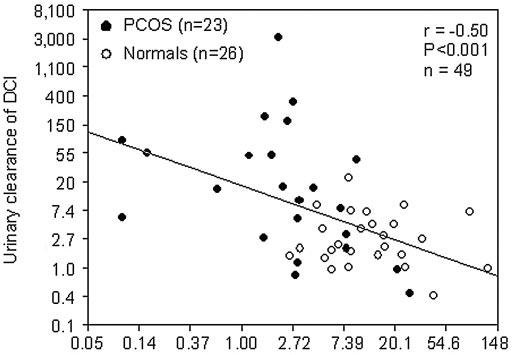
Figure 1—Correlation between urinary clearance of DCI and S when women with PCOS andnormal women were analyzed together. Results are represented back-transformed in their original
firmed with two-way ANOVA. Further-more, insulin sensitivity correlatedinversely and robustly with uClDCI, and
women (2.9 [1.1–7.3] vs. 2.9 [1.6 –5.3],
levels (partial P ϭ 0.02). This first inter-
action has already been detailed above.
insulin-stimulated release of the putative
tween uClDCI and Si identified in the en-
serve as an internal control, the parame-
tire group by univariate analysis (Fig. 1)
ters of a different inositol, MYO, were also
than in normal control subjects (P ϭ
assessed. The levels and urinary clearance
0.025) (Table 1). Because insulin released
the effect of uClDCI (partial P ϭ 0.002)
was adjusted successively for total testos-
tus (adjusted R2 ϭ 0.55 and P Ͻ 0.001 for
[37.8 nmol ⅐ minϪ1 ⅐ lϪ1] vs. 2,312 IU ⅐
minϪ1 ⅐ mlϪ1 [16.0 nmol ⅐ minϪ1 ⅐ lϪ1],
the relationship between uClDCI and Si
significant interaction was found between
total testosterone levels and uClDCI (par-
testosterone and Si. Furthermore, uClDCI
tial P ϭ 0.04), which means that total tes-
remained strongly associated with insulin
resistance after correction for potential
was an inverse correlation between S
DCI) (r ϭ Ϫ0.60, P ϭ 0.002, n ϭ 24).
DCI, which was relatively strong (r ϭ
This association in subgroup analysis was
tional predictors of insulin sensitivity and
0.50) and highly significant (P Ͻ
stronger after correction for BMI (partial
0.001) (Fig. 1). Correlation between SP Ͻ 0.001). No association between total
women (n ϭ 23, r ϭ Ϫ0.39, P ϭ 0.07),
Ͻ3.9 ml/min (P ϭ 0.51, predictors of insulin resistance, along
but not in control subjects (P ϭ 0.63). n ϭ 24), even after correction for BMI.
These results might be related to the lim-
ited numbers of women in each group.
above were considered was S ϭ ␣ ϩ
strongly suggest a contribution of abnor-
mal handling of DCI to the insulin resis-
tivariate analysis when the effect of group
R2 ϭ 0.73, P Ͻ 0.001). The three pa-
status (partial P ϭ 0.14) was adjusted suc-
cessively for BMI, Si, total testosterone
dently predicting Si were therefore
PCOS or not) was not a predictor of insu-
levels, and WHR (adjusted R2 ϭ 0.49 and
AUCinsulin (negative association, partial
P Ͻ 0.001 for model). However, signifi-
P Ͻ 0.001), uClDCI (negative associa-
tion, partial P ϭ 0.01), and the interac-
BMI and group status (partial P Ͻ 0.001)
tion between uClDCI and total testosterone
DIABETES CARE, VOLUME 29, NUMBER 2, FEBRUARY 2006
Altered DCI urinary clearance in PCOS
tissues. The consequence is an intracellu-
lar deficiency of DCI and, ultimately, of
the DCI-IPG mediator of insulin action.
which suggests a role of insulin resistance
sponse to stimulation by insulin results in
a further decrease in insulin sensitivity
ported that the relative increase in the bio-
(i.e., aggravation of insulin resistance).
Hence, a “vicious cycle” is initiated
whereby insulin resistance is amplified in
and diabetic subjects. Urinary DCI excre-
PCOS through the induction of a defect in
ulations, ranging from 2.1 to 96.0 mol/
suffers from the lack of direct evidence for
mean 24-h urinary excretion of DCI of 3.7
mol/day (Table 1 reports geometric opposed to undetectable levels through- tion in our study. This is because it is dif-means), which was comparable to the 2.1
out the clamp in patients with type 2 di-
mol/day reported by Ostlund et al. (26) abetes (16). Finally, a recent study pathway in vivo. using the identical gas chromatography/
the action of insulin in obese women with
icant results, even in multivariate analy-
multiple linear regression models built for
several purification steps and did not use
sumed in the diet, and it is unlikely that a
stability. Such validation in another pop-
dietary deficiency could substantially al-
ulation would be of great interest. Second,
ute in part to these differences (29).
are also possible, such as an abnormality
ditions associated with insulin resistance,
in tissue/cellular uptake of DCI and/or in-
such as diabetes, impaired glucose toler-
ance, and familial history of diabetes.
these latter mechanisms should be associ-
uClDCI is inversely correlated with insulin
Ostlund et al. (26), however, reported an
ated with a normal or increased circulat-
sensitivity in women, and this correlation
observe. Finally, it is possible that more
than one metabolic abnormality is present
also one of only three variables that best
predicted insulin sensitivity in our study.
sistent with a defect in tissue availability
PCOS, which correlates inversely with in-
findings and the findings of Ostlund et al.
sulin sensitivity, is consistent with two
contribute to the insulin resistance of the
possible scenarios. One is that the defect
causes insulin resistance. The other is that
of insulin action. These findings offer a
chiro-inositol confounds interpretation of
insulin resistance, or more likely the hy-
the studies of diabetic individuals, espe-
(10 –12), which reported that oral admin-
cially if diabetes was not well controlled.
clearance of DCI. It is also possible that
other salutary effects consistent with an
lease of bioactive DCI-IPG per unit of in-
environmental “insult” causing insulin re-
relevant to other disorders characterized
sistance leads to a compensatory hyperin-
lease is coupled with the release of insulin
induces a defect that increases renal clear-
ance of DCI, and this leads to a reduction
Acknowledgments — This study was sup-
AUCDCI-IPG-to-AUCinsulin is likely a more
in circulating DCI and its availability to
ported in part by National Institutes of Health
DIABETES CARE, VOLUME 29, NUMBER 2, FEBRUARY 2006
Baillargeon and Associates
Grants R01HD35629 (to J.E.N.), K24HD40237
(to J.E.N.), and R01DK58698 (to R.E.O.) and
the Fond de Recherche en Sante´ du Que´bec (to
puter program to calculate insulin sensi-
polycystic ovary syndrome. N Engl J Med
11. Iuorno MJ, Jakubowicz DJ, Baillargeon JP,
cose tolerance test. Comput Methods Pro-References
Effects of D-chiro-inositol in lean women
with the polycystic ovary syndrome. En-
vised 2003 consensus on diagnostic crite-
ria and long-term health risks related to
12. Gerli S, Mignosa M, Di Renzo GC: Effects
polycystic ovary syndrome (PCOS). Hum
of inositol on ovarian function and meta-
polycystic ovary syndrome. JCEM 68:
2. Zawadsky JK, Dunaif A: Diagnostic crite-
trial. Eur Rev Med Pharmacol Sci 7:151–
23. Nestler JE, Powers LP, Matt DW, Stein-
wards a rational approach. In Current
gold KA, Plymate SR, Rittmaster RS, Clore
Issues in Endocrinology and Metabolism:
13. Romero G, Larner J: Insulin mediators
JN, Blackard WG: A direct effect of hyper-
Polycystic Ovary Syndrome. Dunaif A, Giv-
and the mechanism of insulin action. Adv
ens JR, Haseltine FP, Merriam GR, Eds.
14. Saltiel AR: Second messengers of insulin
the polycystic ovary syndrome. JCEM 72:
action. Diabetes Care 13:244 –256, 1990
3. Baillargeon JP, Iuorno MJ, Nestler JE: In-
15. Asplin I, Galasko G, Larner J: Chiro-ino-
24. Nestler JE, Beer NA, Jakubowicz DJ, Beer
sulin sensitizers for polycystic ovary syn-
sitol deficiency and insulin resistance: a
RM: Effects of a reduction in circulating
drome. Clin Obstet Gynecol 46:325–340,
comparison of the chiro-inositol- and the
4. Baillargeon JP, Iuorno MJ, Nestler JE:
and muscle of control and type II diabetic
25. Sodergard R, Backstrom T, Shanbhag V,
subjects. Proc Natl Acad Sci U S A
polycystic ovary syndrome. Curr Opin En-
bound fractions of testosterone and estra-
docrinol Diabetes 9:303–311, 2002
16. Kennington AS, Hill CR, Craig J, Bogar-
body temperature. J Steroid Biochem 16:
26. Ostlund REJ, McGill JB, Herskowitz I,
dent diabetes mellitus. N Engl J Med 323:
metabolic profile. JCEM 84:4006 – 4011,
17. Baillargeon JP, Iuorno MJ, Jakubowicz DJ,
mellitus. Proc Natl Acad Sci U S A 90:
6. Cattrall FR, Healy DL: Long-term meta-
27. Craig JW, Larner J, Asplin CM: Chiro-ino-
bolic, cardiovascular and neoplastic risks
lated release of D-chiro-inositol-containing
sitol deficiency and insulin resistance. In
with polycystic ovary syndrome. BestMolecular Biology of Diabetes II. Draznin B,
Pract Res Clin Obstet Gynecol 18:803– 812,
with polycystic ovary syndrome. JCEM
7. Nestler JE: Role of hyperinsulinemia in
18. Bergman RN, Phillips LS, Cobelli C: Phys-
28. Suzuki S, Kawasaki H, Satoh Y, Ohtomo
iologic evaluation of factors controlling
syndrome, and its clinical implications. Semin Reprod Endocrinol 15:111–122,
insulin sensitivity and beta-cell glucose
sensitivity from the response to intrave-
insulin sensitivity in Japanese type II dia-
8. De Leo V, la Marca A, Petraglia F: Insulin-
nous glucose. J Clin Invest 68:1456 –1467,
betes. Diabetes Care 17:1465–1468, 1994
29. Larner J, Craig JW: Urinary myo-inositol-
polycystic ovary syndrome. Endocr Rev
19. Yang YJ, Youn JH, Bergman RN: Modified
to-chiro-inositol ratios and insulin resis-
protocols improve insulin sensitivity esti-
tance. Diabetes Care 19:76 –78, 1996
mation using the minimal model. Am J
30. Shashkin PN, Shashkina EF, Fernqvist-
Forbes E, Zhou YP, Grill V, Katz A: Insulin
20. Bergman RN: Lilly lecture 1989: Toward
mediators in man: effects of glucose inges-
polycystic ovary syndrome. Diabetes 38:
tion and insulin resistance. Diabetologia
tolerance: minimal-model approach. Dia-
DIABETES CARE, VOLUME 29, NUMBER 2, FEBRUARY 2006
ADHD (Attention Deficit Hyperactivity Disorder) ADHD, vroeger ook wel MBD (Minimal Brain Dysfunction) genoemd, valt in de DSM-IV uiteen in de volgende drie groepen: • Het onoplettende type. Dit is het type waarbij er vooral sprake is van ernstige en aanhoudende aandachtszwakte (moeite om de aandacht in het hier-en-nu te houden). Dit wordt ook wel het ADD-type genoemd. • Het hyperactieve/im
National Parks of Otago and Southland Neville Peat The two national parks in Otago and Southland – Fiordland and Mount Aspiring –contain the remotest, wildest landscapes in New Zealand. The parks meet in the region of the Hollyford Valley. To the south lies a vast region of fiords and jumbled topography; to the north is Aspiring country, a mountainous and glaciated region that embraces the
 Baillargeon and Associates
Baillargeon and Associates