Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Microsoft word - bowel 1207.doc
Bowel management
Spirella Building, Letchworth, SG6 4ET 01462 476700 www.mstrust.org.uk reg charity no. 1088353
We hope you find the information in this factsheet helpful. If you would like to speak with someone about any aspect of MS, contact the MS Trust information team and they will help find answers to your questions. This factsheet has been provided free by the Multiple Sclerosis Trust, a small UK charity which works to improve the lives of people affected by MS. We rely on donations, fundraising and gifts in wills to be able to fund our services and are extremely grateful for every donation received, no matter what size. MS Trust information service Helping you find the information you need The MS Trust offers a wide range of publications, including a newsletter Open Door, which provides an ongoing update on research and developments in MS management. In addition it contains articles from people with MS and health professionals. For a full list of MS Trust publications, to sign up for Open Door and much more visit our website at www.mstrust.org.uk Freephone 0800 032 3839 (Lines are open Monday – Friday 9am-5pm) email Bowel management
Date of issue: July 2012 This factsheet will be updated within three years Contents
1. Introduction 2. How the bowel works 3. Common bowel problems in MS 3.1 Constipation Causes of constipation Management of constipation 3.2 Faecal incontinence Causes of faecal incontinence Management of faecal incontinence 3.3 Additional factors concerning bowel problems 4. Useful resources 5. References 1. Introduction
Bowel problems are commonly experienced by people with MS. Estimates
vary about the number of people affected and the problem is thought to be
under-reported. However, it is believed that around half of all people with MS
experience bowel problems at some stage1,2. Bowel symptoms can be a
source of considerable distress in MS, having an impact on quality of life,
including self-esteem, sexuality and limiting ability to work.
constipation and difficulty in emptying the bowel
faecal incontinence and lack of control over bowel opening.
It is not uncommon for people with MS to experience both constipation and
Bowel control is an extremely complex process that involves the coordination
of many different nerves and muscles. For people with MS, bowel problems
are often accompanied by problems with mobility, spasticity and fatigue, which
can present additional management difficulties. However, with the right
information and support, the majority of bowel problems can be managed
Though bowel problems are often difficult to talk about and can cause some
embarrassment, there are teams of health professionals dedicated to the
management of problems and support for people who experience them. It is
important for people to know that they are not alone. The sooner help is
sought, the sooner the focus can shift from the problem to the solution.
Many hospitals, Primary Care Trusts (PCT), Clinical Commissioning Groups
(CCG) and Health Boards now have a continence advisor, or continence
nursing service, that deals specifically with bladder and bowel problems. To
find these services, contact NHS Choices, or the Bladder and Bowel
Foundation (see Section 4 - Useful resources). In some areas, people may be
able to refer themselves to continence services, or MS specialist nurses and
While bowel problems are a common symptom of MS, there can be other
causes such as medication or other underlying conditions. It is therefore
essential that any bowel problems are properly assessed by a continence
2. How the bowel works
In normal bowel function, digested food passes from the stomach into the
small intestine where essential nutrients are absorbed into the body. The
waste left after this process passes into the colon, where water is extracted
before the waste is passed to the rectum to be expelled. When waste moves
into the rectum, it stretches the rectum, triggering messages to the brain, thus
causing an awareness of the need to evacuate - known as the 'call to stool'.
The rectum is filled with sensitive nerve endings which can tell the difference
between solid or liquid stool, or wind. In MS, these messages may be
interrupted, affecting awareness of bowel movements3. Other bowel problems
in MS may arise as a result of disruption between messages from the brain to
Diagram of the bowel 3. Common bowel problems in MS 3.1 Constipation
Constipation can be defined as: "the passage of hard stools, less frequently
than the patient's usual bowel pattern" 4.
Constipation is common in the developed world. It is estimated that as much
as one fifth of the adult population who consume a western diet, experiences
constipation at some stage in their lives5.
Although it is not fully understood how and why constipation happens in MS,
research has identified a number of contributing factors, which may, or may
Causes of constipation
Sluggish bowel/slow transit bowel
In some people with MS, waste travels through the colon more slowly than in
those without MS6. This slower transit time is most likely explained by the
disruption of messages from the bowel to the brain that occurs in MS, a
lessening of general physical activity, lack of fibre in the diet and the use of
multiple medications. As digested food moves through the colon, the slow
transit of stools increases the amount of water that will be reabsorbed from
the waste, making stools much harder, smaller, and more difficult to pass.
Reduced sensation in the back passage (rectum)
Some people with MS have reduced sensation in the rectum. This can lead to
a loss in awareness of the need to empty the bowel, so that stool remains in
the rectum for longer, allowing more water to be reabsorbed. This results in
harder, smaller stools that are more difficult to pass.
Evacuation difficulties
Some people with MS have difficulty passing stool out of the rectum, although
it may have travelled normally through the colon. This can mean that the stool
stays longer in the rectum leading to constipation, or the rectum may become
loaded with soft-formed stool. This can be caused by a lack of coordination of
the muscles around the pelvic floor which control bowel emptying.
Lack of fibre in the diet
Dietary fibre is found in wholegrain foods such as wholemeal bread, weetabix,
bran flakes and in fruits and vegetables. Fibre is not digested during its
passage through the gut. It absorbs liquid and provides bulk for the stool. A
bulky soft-formed stool stimulates the natural movements of the gut and helps
to prevent constipation. Many people do not eat enough fibre in their diet and
this contributes to constipation. However, individuals with slow colonic transit
should not eat very large amounts of fibre as this can lead to even slower
Inadequate fluid intake
Some people with MS try to manage their bladder problems by reducing the
amount of fluids they drink. This can lead to dehydration. To compensate, the
body will try to reabsorb as much water as possible from food waste, leading
to harder stools and increased likelihood of constipation.
It is important to drink enough fluid. Current recommendations are 1.5-2.5
litres of fluid a day - about eight full glasses. The exact amount will vary
according to weight and height, as the calculation is based on 30ml of fluid per
1kg of body weight7. Pale, straw coloured urine indicates an adequate intake
It is worth discussing the amount of fluid needed with a continence advisor or
MS specialist nurse, particularly if it causes, or increases, bladder problems.
Reduced mobility
Reduced mobility can lead to lack of exercise and, sometimes, weaker
muscles. Exercise and muscle strength are thought to be important as they
help increase the muscle contractions within the gut, promoting gut transit and
Reduced mobility may create difficulty in getting to a toilet promptly, which can
Needing help with toileting - 'performing' at the convenience of carers - can
also create constipation problems, which need to be managed.
Medication
Many common MS medications list constipation as a possible side effect,
drugs used for bladder problems such as tolterodine (Detrusitol) and
drugs for pain management such as carbamazepine (Tegretol)
anti-depressants, such as amitriptyline (Triptafen) or imipramine
(Tofranil), which may be prescribed for pain relief, and the selective
serotonin reuptake inhibitors (SSRI) such as fluoxetine (Prozac) and
some dietary supplements such as iron and calcium tablets.
Other causes
There may be other causes of constipation. For example, many women
experience changes in bowel pattern at times of hormonal fluctuation such as
menstruation, pregnancy, or after the menopause.
Management of constipation
There has been very little research into which management strategies for
bowel problems are most successful in multiple sclerosis. Consequently,
management is based on the experience of people with MS, as well as
continence advisors. The experience of individuals with very similar problems
due to other neurological problems, like spinal cord injury, can be helpful8.
The main steps for managing constipation are:
Assessment of daily diet
This will particularly look at fibre and fluid intake and may involve keeping a
food diary to record the effect of any dietary changes on symptoms.
Fibre:Adequate amounts of fibre are necessary to maintain soft-formed
stools. However, the right type of fibre is important. For people with a sluggish
bowel, too much wheat-based fibre (eg bran-based breakfast cereals) can
slow down the gut even further. Fibre from the recommended five portions of
fruit and vegetables per day, with one or two portions of wholegrain foods,
should help with constipation. Increases in fibre should be introduced
gradually, to minimise unwanted side effects such as bloating and wind, and
should be accompanied by sufficient fluids.
Fluid:Sufficient fluid intake is important. As discussed, exact amounts vary
from person to person. However, drinking enough to produce pale straw
coloured urine throughout the day is a good indication of sufficient fluid intake.
Remember, additional fluid is needed in warm weather.
Regular bowel habit
It is important that a continence advisor provides advice on how to develop
and practise regular bowel routine. Often people will learn to open their
bowels at a specific time of day. The most active time for the reflexes that help
empty the bowel is around half an hour after a meal; the response is strongest
Give it time
It is important that people are not rushed when trying to open their bowel. If,
after twenty minutes, nothing has happened, the person should stop and try
again after the next meal (eating and drinking will stimulate bowel movement),
Posture during bowel opening
The human body's natural posture for bowel opening is to squat. However,
this is no longer common in the western world. The nearest approximation is
the 'brace and bulge' technique as shown in the diagram below:
Whilst sitting on the toilet, the knees are raised so they are higher than the
hips (this can be helped by using a footstool, a pile of telephone directories, or
something similar); lean forward, resting the elbows on knees, if possible;
movement of stools can then be helped by bracing the abdominal muscles
and bulging the abdominal wall outwards.
Knees higher than hips Lean forward Put elbows on knees Bulge
Abdominal massage
Abdominal massage can help to encourage movement of waste through the
gut3. Abdominal massage techniques can be used with the 'brace and bulge'
position during evacuation, as some people find 'brace and bulge' does not
work on its own; this technique should be taught by an MS specialist nurse, a
continence advisor, or other trained person. Regular use of an abdominal
massage technique with the person lying on their back, can also be beneficial;
this can either be carried out by a health professional, a partner, or the person
Review of existing medication and dietary supplements
It is possible that existing medication, or dietary supplements, are causing, or
contributing to, symptoms. It is therefore important to identify any of these
potential factors and to consider alternatives where available.
Some, or all, of these steps should enable many people to manage
constipation. For some people, additional help may be needed. There are
treatments and medicines which can help with different problems. These
should be discussed with the MS specialist nurse, or continence advisor, to
Bulk forming laxatives eg ispaghula (Fybogel,Isogel), methylcellulose
(Celevac), sterculia (Normacol). These may be useful where dietary fibre
cannot be increased and are used daily, at regular times; a good fluid
Stool softeners eg docusate (Docusol, Norgalax) soften stool, making it
Osmotic laxatives eg macrogol (Movicol) or lactulose (Duphalac,
Lactugal) work by drawing water from the lining of the gut to smooth out
Enemas are fluids inserted into the rectum. Mini enemas can be inserted
by an individual on a regular basis to help the bowel to empty. Larger
volume enemas are usually given by a health professional and are used
Stimulant laxatives eg senna and Bisacodyl. A stool softener used on its
own may not always be sufficient and a stimulant laxative may also be
needed, especially in the case of a sluggish bowel. Senna and Bisacodyl
cause the muscles of the colon to contract more often, and with greater
force. When the colon contracts, it moves the gut contents along more
effectively, thereby alleviating constipation. Stimulant laxatives take
between eight and 12 hours to work. If assistance is needed with getting to
the toilet it is important to plan the right time to use stimulant laxatives, as
difficulties may arise with controlling the bowel.
Suppositories are capsules inserted into the rectum to help lubricate the
stool and to stimulate the back passage to expel the stool.
Trans anal irrigation (also known as anal irrigation or rectal irrigation) eg
Peristeen or Qufora. Trans anal irrigation is a system that can be used in
the management of both constipation and faecal incontinence. The system
works by introducing warm tap water into the bowel using a catheter or
cone whilst the person sits on the toilet. This encourages the muscles in
the bowel to contract and push the stool out. The system is only available
after assessment by a qualified health professional, who will also teach the
method of administration. (For further information see Section 4 - Useful
3.2 Faecal incontinence
Faecal incontinence - having no control over when the bowel opens - can
happen in MS for a variety of reasons. This most embarrassing of symptoms
is normally treatable, but needs proper assessment and management by a
continence advisor or MS specialist nurse.
Causes of faecal incontinence
Reduced sensation
Loss of or limited sensation can result in a lack of awareness of the need
to empty the bowel. The first line of treatment is to establish a regular
bowel habit. Further treatment will depend on the success of this
Constipation
Constipation that causes faecal incontinence is known as 'faecal impaction
with overflow'. The rectum fills with hard impacted stools. Watery matter
may leak round the sides, causing diarrhoea.
Normal treatment is to clear the impaction first, usually with some form of
laxative, suppository, or enema. Regular effective emptying of the bowel
will help avoid build up of constipated stools and development of faecal
impaction. However, this is not always successful. The MS specialist
nurse, or continence advisor, may suggest a long-term management plan
involving a combination of medicines and other techniques.
Other causes
When bowel control is impaired, excessive fibre in the diet or too much
stimulant laxative can result in incontinence. When stool is loose the risk of
incontinence is much greater, and gastrointestinal viruses can cause
faecal incontinence. It is very important that the cause of any sudden
episode of incontinence is correctly identified. Diarrhoea caused by a
gastrointestinal virus may, or may not, need medical treatment, but should
always be assessed by a GP. Here again, changes to diet and establishing
a predictable bowel routine may help. Medication, such as loperamide (see
below), may be helpful where all other causes of diarrhoea have been
Management of faecal incontinence
Pelvic floor exercises, practised over a period of time, may help
strengthen the muscles around the anus and allow the individual greater
control. These exercises are typically taught by a continence advisor.
Loperamide (Imodium) isa medicine that slows down the movement of
the intestine. Loperamide works by making the stools more solid and less
frequent. It is essential to follow the advice of a continence specialist or
Trans anal irrigation eg Peristeen, Qufora (see p9)
Biofeedback retraining is a technique available in some specialist
centres. It aims to retrain individual awareness about bowel opening, diet
and fluid intake. Biofeedback may be useful for individuals with relapsing
Surgeryis an option for a few people with severe bowel incontinence that
cannot be managed in any other way. Surgery offered is normally a
colostomy, which involves bringing the end of the bowel out through the
wall of the abdomen, so waste is collected in a special bag. While for some
people this can be a positive decision, it needs to be carefully discussed
with the surgeon and continence advisor or MS specialist nurse.
3.3 Additional factors concerning bowel problems
There are a number of other factors that deserve consideration by people
Skin care
Caring for the skin around the anus is important. Barrier creams, such as
Cavilon, can be useful in preventing discomfort if incontinence is a
problem. Carefully washing and drying the area if the skin is soiled after a
bowel movement, wearing loose cotton underwear that allows skin to
breathe and avoiding perfumed soaps, creams and lotions, can all help. A
continence advisor or MS specialist nurse will be able to advise.
Containing the problem
When all other ways of improving continence have been tried, pads and
pants can help to deal with faecal incontinence. The Peristeen anal plug
may help some individuals to retain stool. A continence advisor and
organisations, such as Promocon, will offer guidance on the most
appropriate continence products (see Section 4 - Useful resources).
Commodes and bedpansare worth considering if urgency is a problem.
National Key card scheme
Disability Rights UK operates the National Key Scheme (NKS) that was
previously run by RADAR. The NKS allows people with disability to use
around 9,000 accessible toilets throughout the country. Keys are available,
for a small charge, directly from Disability Rights UK (see Section 4 -
Useful resources), or in some cases from local authorities. A guide of NKS
toilet locations is also available to purchase via the Disability Rights UK
Urgency cards
Urgency cards may prove useful as they explain why a person may need
to use a toilet quickly. The 'Just Can't Wait' cards can be presented to give
immediate access to a toilet when there are long queues, or if an individual
needs to use a shop's facilities. Cards are available from the Bladder and
Bowel Foundation (see Section 4 - Useful resources).
Mobile phone apps
Mobile phone apps have been developed to help locate the nearest toilet.
For example, the National Key Scheme (NKS) app can show the location
of the nearest NKS toilet. Coloplast provide a free app to help locate the
nearest wheelchair accessible facilities. See Section 4 - Useful resources
4. Useful resources Bladder and Bowel Foundation is a charity providing information and
support for all types of bladder and bowel related problems, for individuals,
their families, carers and health professionals. They have a confidential
helpline (0845 345 0165) staffed by specialist continence nurses and
Website: www.bladderandbowelfoundation.org
email: info@bladderandbowelfoundation.org
Coloplast Limited. Manufacturer of Peristeen and other healthcare products
and services. For further information about Peristeen Anal Irrigation, call 0800
Colostomy Association. Charity offering support and care for people
contemplating or having undergone an operation, such as a colostomy. It
provides a helpline (0800 328 4257) and has a network of regional support
Website: www.colostomyassociation.org.uk
Disability Rights UK, formed through a merger of RADAR, Disability Alliance
and National Centre for Independent Living, is a national organisation led by
disabled people. They operate the National Key Scheme (NKS) that was
NHS Choices. Website operated by the NHS, providing information on
medical conditions, healthy living, health news and regional health services.
PromoCon. A national service, working as part of the Disabled Living charity,
offering product information, advice and practical solutions to both
professionals and people affected by bladder or bowel problems, including a
5. References
1. Wiesel P, et al. Pathophysiology of bowel dysfunction in multiple sclerosis. European
Journal of Gastroenterology and Hepatology 2001;13(4):441-448.
2. Bakke A, et al. Bladder, bowel and sexual dysfunction in patients with multiple sclerosis: a
cohort study. Scandinavian Journal of Urology and Nephrology 1996; (Suppl) 179: 61-66.
3. MS Trust. Bowel dysfunction. In: MS Trust: Multiple sclerosis: information for health and
social care professionals. Letchworth Garden City: MS Trust; 2011.
4. National Prescribing Centre. The management of constipation. Prescribing Nurse Bulletin
5. Cook T, et al. The conservative management of constipation in adults. Journal of the
Association of Chartered Physiotherapists in Women’s Health1999;85:24-8.
6. Norton C. Bowel management in multiple sclerosis. Gastrointestinal Nursing 2004;2(6):31-
7. British Dietetic Association 2007. Fluid – why you need it and how to get enough.
www.bda.uk.com/foodfacts/fluid.pdf [cited July 2012].
8. Multidisciplinary Association of Spinal Cord Injury Professionals. Guidelines for
Management of Neurogenic Bowel Dysfunction after Spinal Cord Injury. MASCIP: Middlesex; April 2009.
9. McClurg D, et al. Abdominal massage for the alleviation of constipation symptoms in
people with multiple sclerosis: a randomized controlled feasibility study. Multiple Sclerosis 2011;17(2);223-33.
10. Wiesel P, et al. Gut focused behavioural treatment (biofeedback) for constipation and
faecal incontinence in multiple sclerosis. Journal of Neurology, Neurosurgery and Psychiatry 2000; 69(2):240-243.
Please contact the MS Trust Information Team if you would like any further information about reference sources used in the production of this publication.
WHAT IS IT THAT SETS OUR SUPER JUICE APART FROM OTHER EXOTIC JUICES? !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!"#$!%&'#!()*&+,-.!/,'0,-#12334! Well, first and foremost, I invite each and every one of you reading this to get on the Internet and see if you can find IONIC ALFALFA. Alfalfa is not just for horses and cows any more! You are not going to find it! I
Cost-effective drugs — WINTER 2010 what’s available? As more prescription drugs hit the Cost-effective drugs by health condition: A convenient chart for you Take control of your holiday stress level Just say “no” to pneumonia and the flu HIGH CHOLESTEROL HIGH BLOOD PRESSURE bad cholesterol as well astriglycerides — fats in the blood —and is a
 Bowel management
Bowel management  We hope you find the information in this factsheet helpful. If you would like to
We hope you find the information in this factsheet helpful. If you would like to 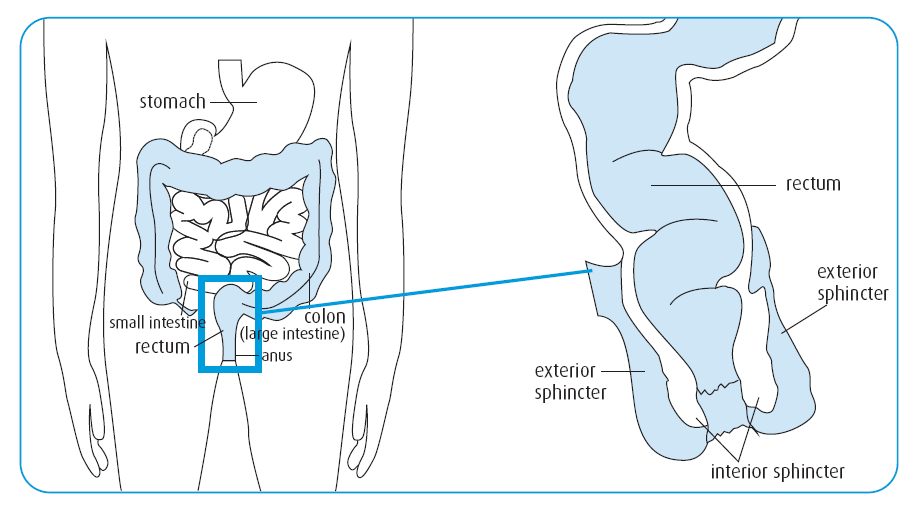 Diagram of the bowel
Diagram of the bowel  again after the next meal (eating and drinking will stimulate bowel movement),
Posture during bowel opening
again after the next meal (eating and drinking will stimulate bowel movement),
Posture during bowel opening