Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
English.pdf
“PROTEZIONE CIVILE EDUCATIONAL” - www.casaleinforma.it/pcivile
V° Contingente CRI at the Italian Red Cross Hospital in Baghdad
PROTOCOL FOR THE TREATMENT OF BURNS AT THE ITALIAN RED CROSS HOSPITAL IN BAGHDAD
Document drawn up by Dr. Sandro Gregorio doctor at the Orthopaedic and
Trauma O.U at the “G. Gaslini” Institute in Genova.
Background
what “non conventional” means: we found ourselves in a situation where we
had to face extensive burns that very often involved 100% of the body
surface, without the aid of resuscitation or intensive care units when the
sacred medical tests state that burns that involve more than 30% of the body
surface have to be treated in the intensive care unit.
Clearly this document is not intended to revolutionize the cure and treatment
of burns but it is aimed only to give indications that can be helpful in case of
medical emergencies that could be verified immediately after a natural
I also have to add another point: the following is the result of about 40 days
constant work on burns and reflexes from my personal point of view as well as
the experience of the other members of the Italian Red Cross mission in
Baghdad. It is therefore my intention to open a debate to actually verify what
has been done and to actually improve our knowledge.
“PROTEZIONE CIVILE EDUCATIONAL” - www.casaleinforma.it/pcivile
Initial Receiving Procedure 1. Freeing of clothes and evaluation of injury: it is of the utmost
importance to “waste time” at this stage to evaluate the priority of the
treatment and therefore the initial positioning of the injured on the bed.2. Venous access for sedation and analgesic therapy: it is quiet clear that
without a certain venous entry the treatment is without effect; in Baghdad
the most commonly used drug to control pain during medication is
Ketamina; other positively used drugs are cocktails of Fentanest and
Diprivan. Naturally this is done also by controlling saturation and oxygen
3. If the burns involve more than 20% of the body surface: urinary catheterisation. 4. Blood samples to evaluate haematic parameters: when possible 5. Start hydration with milk white Ringer and physiological solution (at least 1000 cc during medication, 500 cc children) 6. Wash injuries with 5% Chlorhexidine solution (0.25% as active
constituent): bowls of solution were used and the gauzes are dipped and
then picked up by the use of pincers.
7. Washing of the inside of the mouth with 4% Chlorhexidine (0.2% as
active constituent) in the case the burns include the area which is inside the
mouth. This can also be done with gauzes that have been dampened with
the Chlorhexidine solution in the case of unconscious patients or as a mouth
wash in conscious patients. Chlorhexidine is absorbed by the mucous
membrane and released in the 6-8 hour period following the treatment to
guarantee the reduction of the saliva bacteria flora for the entire period.
8. Extirpation of the delimited necrotic parts and of the uplifted skin. Removal of the flictene if present, leaving the superficial surface intact:
leaving the skin of the flictene is possible only if they are isolated; the
emptying injection must be carried out in sterile conditions.
9. Disinfection of the injuries with Betadine: sterile gauzes soaked in
Betadine are passed over the injuries trying to avoid rubbing them.
“PROTEZIONE CIVILE EDUCATIONAL” - www.casaleinforma.it/pcivile
10. Application of Sofargen cream on the injuries: this cream is
11. Covering with fatty gauzes and layers of sterile gauzes and further bandaging: we had
characterized by sufficient absorbent properties, to take into consideration
the notable secretions that are produced. Naturally the fingers of the hands
must be bandaged separately, or at least separate between themselves
inside the bandage. it is also necessary to keep the folds of the skin
separate such as armpits to avoid painful adherence.
12. If the patient is catheterised the quantity of urine must be controlled
to evaluate the further necessity of infusions.
13. Start of antibiotic treatment with wide scale antibiotics.
Start gastro protective therapy with Ranitidina 50 mg 3 times a day for
adults, twice a day for children by means of injections: the antibiotic therapy
that was used was based on Piperacillina with the addition of Flagyl and
Gentamicina in the following phases if necessary. Take into consideration that
these were the antibiotics that were available: we would have also liked to
have used Vancomicina, but it was difficult to obtain.
Patients in hospital
The day after admission it is necessary to control the laboratory parameters,
urine quantity as well as body temperature.
The calculation of the quantity of liquid to be introduced as well as the anti
“PROTEZIONE CIVILE EDUCATIONAL” - www.casaleinforma.it/pcivile
Liquids must be plentiful: 6000 cc a day at least for adults and 4000 for
children. The flow of urine can cause confusion because the patients are hemo-
It is better to not give the patients food the first day.
For the infusion therapy it is better to use not more than 500 cc of Ringer and
it is preferable to use glucose and Normosol solutions with the addition of a
physiological solution for the alternatives.
The Ringer is gradually abandoned during the following days.
Subsequent Medication
§ Blood samples for laboratory exams on the basis of which the subsequent
§ Washing of injuries with a 5% Chlorhexidine solution.
§ Removal of the delimited necrotic parts: this is an ideal environment for
germs. It is better to remove them with surgical instruments: the blade
must cut the edge between healthy and necrotic and to make the cut easier
it must be tractioned perpendicular to the surface that is to be separated
§ Disinfection with Betadine and the application of Sofargen cream: the
Sofargen cream is not to be used on the granulated parts where only the
§ Covering with fatty and sterile gauzes and following bandaging.
Sofargen: do not use this cream on the exposed under epidermis and on Granulation: if hypertrophic it is better to reduce the area with touches of
silver nitrate. Gloves : are to be changed often during medication, they must
be changed after washing of the injuries and whenever soiled.
Pincers: it is better to use pincers to pick up the gauzes from the
Chlorhexidine solution so as not to pollute it.
“PROTEZIONE CIVILE EDUCATIONAL” - www.casaleinforma.it/pcivile
Chlorhexidine: this was available in a 5% active solution, the above
mentioned solutions are prepared by diluting the product as it is. The real
concentration of the active material is to be reported.
Chlorhexidine is not compatible with normal detergents due to its cationic
nature. It is necessary to avoid mixing it with detergents.
Betadine solution: 10% active principal (Iodopovidone). The application is to
be carried out with the product as it is. Sofargen: this is a local wide scale antimicrobic, with a silver sulfadiazine base, it is a metallorganic substance obtained by
the reaction between the silver nitrate with the sulfadiazine. It was available in cream with 1% active principal. Cuticerin: Gauze (AG) consists of a gauze dressing made from fibers of cellulose acetate, impregnated with a cream composed of petrolatum, mineral oil, mineral wax and wool-wax alcohol. Conclusion
This was our treatment of patients with burns. However the silver nitrate in a
pencil form was impossible to obtain so therefore we treated the hypertrophic
granulations with dry medications that however have the disadvantage of
being painful when removed or with the surgical reduction.
I hope that this information will be a source of further discussion.
My e-mail address is : sandrogregorio@ospedale-gaslini.ge.it
“PROTEZIONE CIVILE EDUCATIONAL” - www.casaleinforma.it/pcivile
V Contingente 2003 Baghdad – Italian Red Cross Hospital Washing with Chlorhexidine solution (2-2.5%) Washing with Betadine (Not soapy solution) Extirpation of the Silver Nitrate on the necrotic parts ( Hypertrophyc granulations (Doctor) Application of Silver Sulfadiazine cream Covering with fatty gauzes, layers of sterile gauzes and further Plastering application to keep the limbs in the correct position Soft bandage
e-mail submissions to correspondence@lancet.comMortality reduction by breast-cancer screening yield accorded with the trial results: oneThis article, together with other reportsJulius Center for Health Sciences and PrimaryCare, Utrecht Medical Center, HP D 01.335,PB 85500, 3508 GA Utrecht, Netherlands(e-mail: l.bonneux@jc.azu.nl)Otto SJ, Fracheboud J, Looman CWN, et al. mammography screeni
“ Yoga como Medicina ” por Timothy MCcall Rolf Sovik começou a estudar yoga com Swami Rama cedo nos anos 70. Por sugestão do seu guru, fez um doutoramento em psicologia clínica, escrevendo uma tese, comparando a terapia cognitiva com yoga, completando um projecto de pesquisa sobre o uso da respiração no tratamento da ansiedade. Rolf exerce como psicoterapeuta, é professor de yoga, e com
 “PROTEZIONE CIVILE EDUCATIONAL” - www.casaleinforma.it/pcivile
V° Contingente CRI at the Italian Red Cross Hospital in Baghdad
PROTOCOL FOR THE TREATMENT OF BURNS AT THE ITALIAN RED
“PROTEZIONE CIVILE EDUCATIONAL” - www.casaleinforma.it/pcivile
V° Contingente CRI at the Italian Red Cross Hospital in Baghdad
PROTOCOL FOR THE TREATMENT OF BURNS AT THE ITALIAN RED  “PROTEZIONE CIVILE EDUCATIONAL” - www.casaleinforma.it/pcivile
10. Application of Sofargen cream
“PROTEZIONE CIVILE EDUCATIONAL” - www.casaleinforma.it/pcivile
10. Application of Sofargen cream 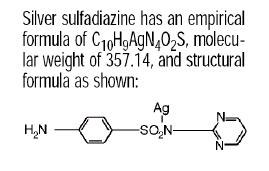 “PROTEZIONE CIVILE EDUCATIONAL” - www.casaleinforma.it/pcivile
Chlorhexidine: this was available in a 5% active solution, the above
“PROTEZIONE CIVILE EDUCATIONAL” - www.casaleinforma.it/pcivile
Chlorhexidine: this was available in a 5% active solution, the above