Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Microsoft word - faverin_112009_pi-10.doc
PRODUCT INFORMATION Name of the drug
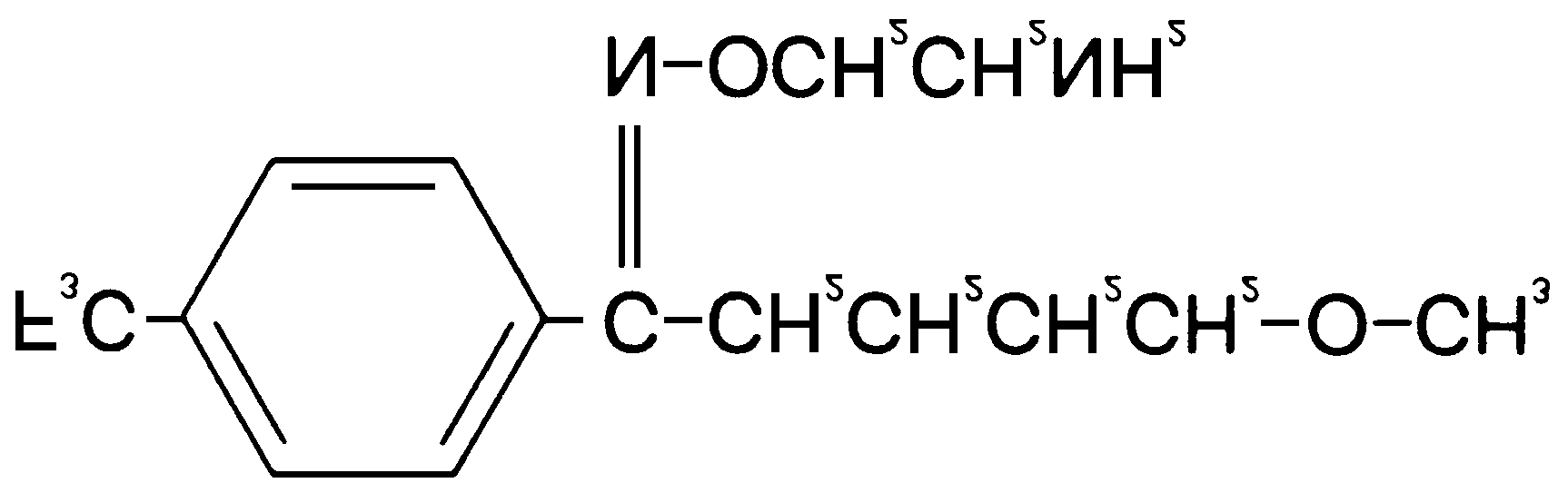
Fluvoxamine maleate is chemically identified as (E)-5-methoxy-4/-trifluoromethylvalerophenone 0-2- aminoethyloxime maleate. It has the fol owing chemical structure:
CAS No. 61718-82-9 MW= 434.4 Description
Fluvoxamine maleate is a white to slightly off-white, odourless, crystal ine powder, sparingly soluble in water, freely soluble in ethanol and chloroform, practically insoluble in diethylether. It has a partition coefficient (n-octanol/water, own pH) P=38.7. Fluvoxamine is a member of a class of antidepressant agents known as selective serotonin reuptake inhibitors (SSRI). It is chemically unrelated to the tricyclic antidepressants, and to other serotonin reuptake inhibitors as it is a monocyclic compound. FAVERIN (fluvoxamine maleate) is available in 50 mg and 100 mg white, film-coated, scored tablets. The inactive ingredients are: mannitol, maize starch, pregelatinised potato starch, sodium stearylfumarate, colloidal anhydrous silica, hypromellose, propylene glycol, talc, titanium dioxide. Pharmacology
Pharmacodynamics
Fluvoxamine has two isomeric forms: an E isomer which is pharmacological y active, and a Z isomer which is non-active. FAVERIN tablets contain only the E isomer. The mechanism of action of fluvoxamine is believed to be related to its ability to selectively inhibit presynaptic reuptake of serotonin, and thus increase the serotonin concentrations within the synaptic cleft. This is accompanied by minimal interference with the noradrenergic and dopaminergic processes. Faverin – Product information
Unlike tricyclic antidepressants, fluvoxamine has limited affinity for alpha adrenergic, beta adrenergic, histaminergic, muscarinic, dopaminergic or serotoninergic receptors. Antagonism of these post- synaptic receptors are believed to be associated with some of the cardiovascular, anticholinergic and sedative effects of classical tricyclic antidepressant drugs. Dose-dependent decreases in rapid eye movement (REM) sleep and increased REM latency were found with fluvoxamine. These effects are similar to those of other antidepressant drugs. Clinical Trials
Depression
In depression, the efficacy of fluvoxamine was established in 15 three-way trials in which fluvoxamine (≥100mg/day) was compared with both placebo and a tricyclic antidepressant (imipramine ≥ 150mg/day or desipramine, ≥100mg/day) generally over a period of 6 weeks and using HAM-D, CGI severity and MADRS as the main efficacy criteria. Of these studies, seven showed conclusive results: four were positive for both fluvoxamine and active reference therapy, whereas the other three studies showed only efficacy for active reference therapy. In a pooled analysis of the results of all these studies, both fluvoxamine (n=837) and active reference therapy (n=779) were found to be more effective than placebo (n=837). HAM-D improvements (LOCF) after 6 weeks were 39.1%, 41.9% and 33.9%, respectively. In these studies, the effective dose range for fluvoxamine was determined to lie between 100mg and 300mg per day. Using various definitions of response based on HAM-D or CGI criteria, there were no statistically significant differences in response rates between fluvoxamine and active reference therapy. Statistical analyses of the data did not reveal any patient features (such as age, sex, race etc.) which predict treatment response to fluvoxamine. Prevention of relapse of depression
A study of depressed outpatients who had responded to fluvoxamine (MADRS ≤ 10) during an initial 26 week open treatment phase (n=204) and were then double-blind randomised to continuation on fluvoxamine (100mg/day) or placebo for 1 year demonstrated a significantly lower relapse rate for fluvoxamine (13%) compared to those on placebo (35%). Obsessive Compulsive Disorder (OCD)
Adult OCD Studies: The effectiveness of fluvoxamine in the treatment of Obsessive Compulsive
Disorder (OCD) was demonstrated in two 10-week placebo-controlled studies (Studies 1 and 2). The results of two 10 week clomipramine-controlled studies (Studies 3 and 4) support the effectiveness of fluvoxamine in the treatment of OCD. -
Studies 1 and 2 were flexible dose double-blind paral el group, multicentre studies in which patients with moderate to severe OCD received fluvoxamine in doses up to 300mg/day or placebo. 157 patients received fluvoxamine versus 158 patients who received placebo. Improvements from baseline in Yale-Brown Obsessive Compulsive Disorder (Y-BOCS) and NIMH-OC scores and the CGI improvement score were significantly greater in fluvoxamine-treated patients. In these studies, the overall response rates were 36% for fluvoxamine and 12% for placebo, and the effective dosage range for fluvoxamine was between 100mg and 300mg daily. In open extension studies, efficacy in OCD was demonstrated to be maintained in a total of 72 patients treated for a total of 46 weeks or more.
Studies 3 and 4 were flexible dose double-blind paral el group multicentre studies comparing fluvoxamine (100-300mg/day) with clomipramine (100mg-250mg/day). 69 patients received fluvoxamine versus 76 patients who received clomipramine. Fluvoxamine and clomipramine were equally efficacious on the Y-BOCS, NIMH-OC and CGI improvement scores.
Paediatric OCD Study: The effectiveness of fluvoxamine for the treatment of OCD was also
demonstrated in a 10-week multicentre, parallel group, placebo-controlled study in a paediatric outpatient population (children and adolescents, ages 8-17) followed by an open-label extension of up to two years.
Faverin – Product information
In the double-blind phase of the study, patients were titrated to a total daily fluvoxamine dose of approximately 100mg/day over the first two weeks of the trial, following which the dose was adjusted within a range of 50-200mg/day (on a b.i.d. schedule) on the basis of response and tolerance. All patients had moderate to severe OCD (DSM-III-R) with mean baseline ratings on the Children’s Yale-Brown Obsessive Compulsive Scale (CY-BOCS), total score of 24. Patients receiving fluvoxamine maleate experienced mean reductions of approximately 6 units on the CY-BOCS total score, compared to a 3 unit reduction for placebo patients. The fol owing table provides the outcome classification by treatment group on the Global Improvement item of the Clinical Global Impression (CGI) scale for the paediatric study.
OUTCOME CLASSIFICATION (%) ON CGI-GLOBAL IMPROVEMENT ITEM FOR COMPLETERS IN PAEDIATRIC STUDY Outcome Classification Fluvoxamine Placebo (N=36)
Post hoc exploratory analyses for gender effects on outcomes did not suggest any differential responsiveness on the basis of gender. Further exploratory analyses revealed a prominent treatment effect in the 8-11 age group and essentially no effect in the 12-17 age group. The reason for the difference in these results is unknown. However, fol ow up data from the open extension of the study showed a further improvement as demonstrated by a decrease of an additional 3 to 6 units on the CY- BOCS in young, as well as adolescent, patients. This improvement was sustained over a one-year period in 54 of the 98 patients who completed the one-year extension and in 12 of the 22 patients who completed the two year extension. Pharmacokinetics
Fluvoxamine is almost completely absorbed following oral administration. The absolute bioavailability is 53% (90% confidence interval: 44-62%). Absorption is unaffected by the presence of food. Maximum plasma levels occur within 3-8 hours of dosing. Steady state levels are usually achieved within one week. The mean plasma half-life is approximately 12-13 hours after a single dose and approximately 22 hours following repeated dosing. The pharmacokinetics of fluvoxamine is linear between single oral doses of 25-100mg. During multiple dosing in the range of 100-300mg per day, the higher doses produced disproportionally higher plasma concentrations than predicted from data obtained with the lower dose. Fluvoxamine undergoes extensive hepatic transformation, mainly via oxidative demethylation, into at least 9 metabolites. Less than 4% of the dose is excreted in the urine as unchanged parent compound, while approximately 94% of the dose is recovered in the urine as metabolites. The two principal metabolites exhibit negligible pharmacological activity. In view of the structures of the other metabolites, it is not expected that the other metabolites would be pharmacologically active. In vitro binding of fluvoxamine to human plasma proteins is 80%, and the volume of distribution is Faverin – Product information
The pharmacokinetics of fluvoxamine in patients with renal dysfunction do not appear to differ significantly from those in healthy, young volunteers. The area under the plasma concentration-time curve (AUC) and half-life were greater, however, in patients with liver dysfunction. Patients suffering from renal or hepatic insufficiency should be careful y monitored when treated with fluvoxamine. Upward dose titration should be carried out more slowly in this patient population. Paediatric subjects The multiple-dose pharmacokinetics of fluvoxamine was determined in male and female children (ages 6-11) and adolescents (ages 12-17). The clearance of fluvoxamine in children was approximately half that observed in adolescents. AUC and Cmax in children were 1.5 to 2.7 fold higher
than that in adolescents. As in adults, both children and adolescents exhibited non-linear multi-dose pharmacokinetics. Female children showed significantly lower clearance values and higher AUC (0-12) and Cmax compared to male children and, therefore, lower doses of FAVERIN may produce therapeutic
benefit. No gender differences were observed in adolescents. Body weight adjusted mean clearance at a dose of 300mg/day was approximately 50% higher in adolescents compared to adults in previous studies. Indications
FAVERIN (fluvoxamine maleate) is indicated for the treatment of major depression in adults. FAVERIN (fluvoxamine maleate) is also indicated for the treatment of Obsessive Compulsive Disorder (OCD) in both children aged 8 years and older, adolescents and adults. Contraindications
Fluvoxamine is contraindicated in combination with tizanidine and monoamine oxidase inhibitors (MAOIs). Treatment with fluvoxamine can be initiated: -
two weeks after discontinuation of an irreversible MAOI, or
the following day after discontinuation of a reversible MAOI. At least one week should elapse between discontinuation of fluvoxamine and initiation of therapy with any MAOI.
Fluvoxamine is contraindicated in combination with cisapride. FAVERIN Tablets are contraindicated in patients with hypersensitivity to any component of the product. (see "Description"). Fluvoxamine has been shown to increase postnatal mortality in rats at doses greater than 1mg/kg/day, and should not be used by nursing mothers. Precautions
Clinical worsening and suicide risk associated with psychiatric disorders
The risk of suicide attempt is inherent in depression and may persist until significant remission occurs. This risk must be considered in all depressed patients.
Faverin – Product information
Patients with depression may experience worsening of their depressive symptoms and/or the emergence of suicidal ideation and behaviour (suicidality), whether or not they are taking antidepressant medications, and this risk may persist until significant remission occurs. As improvement may not occur during the first few weeks or more of treatment, patients should be closely monitored for clinical worsening and suicidality, especially at the beginning of a course of treatment, or at the time of dose changes, either increases or decreases. Consideration should be given to changing the therapeutic regimen, including possibly discontinuing the medication, in patients whose depression is persistently worse or whose emergent suicidality is severe, abrupt in onset, or was not part of the patient’s presenting symptoms. Patients (and caregivers of patients) should be alerted about the need to monitor for any worsening of their condition and/or the emergence of suicidal ideation/behaviour or thoughts of harming themselves and to seek medical advice immediately if these symptoms are present. Patients with co-morbid depression associated with other psychiatric disorders being treated with antidepressants should be similarly observed for clinical worsening and suicidality. Obsessive compulsive disorders may also be associated with an increased risk of suicide-related events. The same precautions should therefore be observed for these patients. Patients with a history of suicide-related events, or those exhibiting a significant degree of suicidal ideation prior to commencement of treatment, are at a greater risk of suicidal thoughts or suicide attempts, and should receive careful monitoring during treatment. Pooled analysis of 24 short-term (4 to 16 weeks) placebo-controlled trials of nine antidepressant
medicines (SSRIs and others) in 4400 children and adolescents with major depressive disorder (16 trials), obsessive compulsive disorder (4 trials) or other psychiatric disorders (4 trials) have revealed a greater risk of adverse events representing suicidal behaviour or thinking (suicidality) during the first few months of treatment in those receiving antidepressants. The average risk of such events in patients treated with an antidepressant with 4% compared with 2% of patients taking a placebo. There was considerable variation in risk among the antidepressants but there was a tendency towards an increase for almost all antidepressants studied. The risk of suicidality was most consistently observed in the major depressive disorder trials but there were signals of risk arising from the trials in other psychiatric indications (obsessive compulsive disorder and social anxiety disorder) as well. No suicides occurred in these trials. It is unknown whether the suicidality risk in children and adolescent patients extends to use beyond several months. The nine antidepressant medicines in the pooled analyses included five SSRIs (citalopram, fluoxetine, fluvoxamine, paroxetine, sertraline) and four non-SSRIs (bupropion, mirtazepine, nefazodone, venlafaxine). Pooled analysis of short term studies of antidepressant medications have also shown an increased risk of suicidality in young adults aged 18 to 24 during initial treatment (generally the first one to two months). Short term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond the age of 24 years; there was a reduction with antidepressants compared to placebo in adults aged 65 years and older. Symptoms of anxiety, agitation, panic attacks, insomnia, irritability, hostility (aggressiveness), impulsivity, akathisia (psychomotor restlessness), hypomania and mania, have been reported in adults, adolescents and children being treated with antidepressants for major depressive disorder as well as for other indications, both psychiatric and non-psychiatric. Although a causal link between the emergence of such symptoms and either worsening of depression and/or emergence of suicidal impulses has not been established there is concern that such symptoms may be precursors of emerging suicidality. Families and caregivers of children and adolescents being treated with antidepressants for major depressive disorder or for any other condition (psychiatric or non-psychiatric) should be informed about the need to monitor these patients for the emergence of agitation, irritability, unusual changes in behaviour, and other symptoms described above, as well as the emergence of
Faverin – Product information
suicidality, and to report such symptoms immediately to health care providers. It is particularly important that monitoring be undertaken during the initial few months of antidepressant treatment or at times of dose increase or decrease. Prescriptions for Faverin should be written for the smallest quantity of tablets consistent with good patient management, in order to reduce the risk of overdose. Seizures
Although in animal studies, fluvoxamine has no pro-convulsive properties, caution is recommended when the drug is administered to patients with a history of convulsive disorders. Fluvoxamine should be avoided in patients with unstable epilepsy and patients with controlled epilepsy should be careful y monitored. Treatment with fluvoxamine should be discontinued if seizures occur or if seizure frequency increases. Glucose Metabolism
Glycaemic control may be disturbed, especially in the early stages of treatment. The dosage of anti- diabetic drugs may need to be adjusted. Heart rate changes
Fluvoxamine may cause a non-significant decrease in heart beat (2-6 beats per minute). Psychomotor Effects
Fluvoxamine at doses up to 150mg per day exhibited no effect on psychomotor skills associated with driving and operating machinery in healthy volunteers. However, somnolence has been reported during treatment with fluvoxamine. Therefore, caution is recommended until the individual response to the drug has been determined. Discontinuation/Withdrawal Symptoms (see also “Dosage and Administration”) The onset of symptoms may occur one to three days after abrupt discontinuation of SSRI therapy and (rarely) after dosage lowering. It is important but may be difficult to distinguish the discontinuation symptoms from a recurrence of the underlying disease. Both may present with disturbances of the equilibrium and of the sensory system. However, they may differ in view of the severity, onset and duration of the symptoms. Discontinuation symptoms rarely occur after treatment of less than 5 weeks duration and usually last from one day to three weeks. It is advised that in accordance with clinical experience and individual need of a patient, the dosage should be gradually tapered over a couple of weeks when discontinuing treatment. Bleeding disorders
There have been reports of cutaneous bleeding abnormalities such as ecchymoses and purpura as well as haemorrhagic manifestations e.g. gastrointestinal bleeding with SSRIs. Caution is advised in patients taking SSRIs, particularly in elderly patients and in patients who concomitantly use drugs known to affect platelet function (e.g. atypical antipsychotics and phenothiazines, most tricyclic antidepressants, aspirin and NSAIDs) or drugs that increase risk of bleeding as well as in patients with a history of bleeding disorders and in those with predisposing conditions (e.g. thrombocytopenia). If any significant bleeding or bruising is observed, it is recommended that a platelet count should be performed.
Faverin – Product information
Use in the Elderly
Data in elderly subjects gives no indication of clinical y significant differences in pharmacokinetics compared with younger subjects. Nevertheless, upward dose titration should be carried out more slowly in this patient population, and dosing should always be handled with caution. Use in Children and Adolescents (age <18 years)
Fluvoxamine should not be used in children and adolescents (age <18 years) for the treatment of major depressive disorder as the efficacy and safety of the medicine in these patients for this condition has not been satisfactorily investigated. Decreased appetite and weight loss have been observed in association with the use of fluvoxamine as well as with other SSRIs. Although no detrimental effect on growth, development and maturation was apparent in the long-term, open-label clinical studies in children, regular monitoring of weight and growth is recommended if treatment of a child with an SSRI is to be continued long term. Use in Renal Insufficiency
Patients suffering from renal insufficiency should be carefully monitored when treated with fluvoxamine. Upward dose titration should be carried out more slowly in this patient population. Use in Hepatic Insufficiency
Patients suffering from hepatic insufficiency should be careful y monitored when treated with fluvoxamine. Upward dose titration should be carried out more slowly in this patient population. Clearance of fluvoxamine is slower in patients with hepatic impairment (e.g. cirrhosis). Carcinogenicity, Mutagenicity, Impairment of Fertility
In animal studies, there was no evidence of carcinogenic activity when fluvoxamine was given to rats at dietary doses up to 211mg/kg/day for 30 months (approximately 2-5 times the maximum human exposure, based on plasma AUC), or to hamsters at about the same dose level for 112 weeks (male) and 85 weeks (female) (approximately two thirds the maximum human exposure, based on plasma AUC). No evidence of mutagenicity or chromosomal damage was observed in vitro. An in vivo test
for chromosomal damage in mice (micronucleus test) gave no clear evidence of clastogenic activity. No evidence of impairment of fertility in male or female rats was observed with fluvoxamine at oral doses up to 80mg/kg/day. Use in Pregnancy (Category C)
There was no evidence of teratogenic effects following administration of fluvoxamine at oral doses up to 80 mg/kg/day to rats and rabbits during the period of organogenesis, with rat exposure (based on plasma AUC similar to human exposure at the maximum recommended human dose. Oral administration of fluvoxamine to rats at doses of 5 – 160 mg/kg/day during late gestation and lactation was associated with increased postnatal pup mortality. Reproduction studies in animals revealed impaired fertility (Note: at doses exceeding about 4 times the maximum recommended human dosage), increased embryofoetal death, decreased foetal body weight and increased incidences of foetal eye abnormalities (folded retina) in fluvoxamine doses which markedly exceed maximum recommended human dose. The potential risk for humans is unknown. Caution should however be exercised when prescribing to pregnant women. Faverin – Product information
Neonates exposed to fluvoxamine, other SNRIs (Serotonin and Norepinephrine Reuptake Inhibitors) or SSRIs (Selective Serotonin Reuptake Inhibitors) late in the third trimester have developed complications requiring prolonged hospitalisation, respiratory support, and tube feeding. Such complications can arise immediately upon delivery. Reported clinical findings have included respiratory distress, cyanosis, apnoea, seizures, temperature instability, feeding difficulty, vomiting, hypoglycaemia, hypotonia, hypertonia, hyperreflexia, tremor, jitteriness, irritability and constant crying. These features are consistent with either a direct toxic effect of SSRIs and SNRIs or, possibly, a drug discontinuation syndrome. Use in Lactation
Oral administration of fluvoxamine to rats at doses greater that 1 mg/kg/day during late gestation and lactation was associated with increased postnatal pup mortality. Since fluvoxamine is excreted in human milk, the drug should not be used by lactating women. (See “Contraindications”). Interactions with Other Drugs
Pharmacodynamic interactions:
Fluvoxamine is a serotonergic drug and it can potentiate the effects of other serotonergic and/or neuroleptic drugs. In rare cases, this could lead to the development of a serotonin syndrome or neuroleptic malignant syndrome (NMS)-like events. As these symptoms may result in potentially life-threatening conditions, treatment with fluvoxamine should be discontinued if such events (characterised by clusters of symptoms such as hyperthermia, rigidity, myoclonus, autonomic instability with rapid fluctuations of vital signs, mental status changes including confusion, hypomania, extreme agitation progressing to delirium and coma) occur and supportive symptomatic treatment should be initiated. Fluvoxamine should not be used in combination with monoamine oxidase inhibitors (MAOIs) (see “Contraindications”). It should be used with caution in combination with other SSRIs, tricyclic antidepressants, tryptophan, sumatriptan, phentermine or tramadol. Although fluvoxamine has been used in combination with lithium in the treatment of severely ill, drug-resistant patients, possible potentiation of serotonergic effect should be kept in mind. As with other SSRIs, possible potentiation of an increased serotonergic effect should be considered where preparations containing St. Johns Wort are used in combination with fluvoxamine. As with other psychotropic drugs, patients should be advised to avoid using alcohol while taking fluvoxamine. When fluvoxamine was co-administered with warfarin for 2 weeks, plasma prothrombin times were prolonged. This can be ascribed to the intrinsic ability of SSRIs to lower the serotonin concentration in blood platelets (which can lead to prolonged bleeding in sensitive patients), and to fluvoxamine increasing the warfarin plasma concentrations (see below). Patients receiving anticoagulants should have their prothrombin time monitored and their anticoagulant dose adjusted accordingly when administered fluvoxamine.
Faverin – Product information
Pharmacokinetic interactions:
Fluvoxamine is metabolised in the liver, mostly via the cytochrome P450 system. While the specific enzymes involved are not definitively known, it would appear, based on available in vitro data, that CYP1A2 is the main isoenzyme involved. To a much lesser extent CYP3A4 and CYP2C19 may also be involved in the metabolism of fluvoxamine. Fluvoxamine is known to prolong the elimination of drugs oxidised in the liver, in particular drugs metabolised via CYP1A2. Fluvoxamine is a moderate inhibitor of CYP3A4 and CYP2C19. Fluvoxamine has only a weak inhibitory effect on CYP2D6, and is therefore not likely to increase plasma concentrations of drugs metabolised by CYP2D6 to a clinically relevant extent. CYP1A2 An increase in previously stable plasma levels of those tricyclic antidepressants (such as clomipramine, amitriptyline and imipramine) and neuroleptics (or antipsychotics such as clozapine and olanzapine) which are largely metabolized through CYP1A2 has been reported when used together with fluvoxamine. The combination of fluvoxamine with these drugs is not recommended. Patients co-administered fluvoxamine and CYP1A2 metabolised drugs with a narrow therapeutic index (such as tacrine, theophylline, methadone, mexiletine) should be carefully monitored and, if necessary, dose adjustments of these drugs is recommended. When given with fluvoxamine, warfarin plasma concentrations were significantly increased and prothrombin time prolonged. Isolated cases of cardiac toxicity have been reported when fluvoxamine was combined with thioridazine. As plasma concentrations of propranolol are increased in combination with fluvoxamine, the propranolol dose may need to be lowered. Caffeine plasma levels are likely to be increased during co-administration with fluvoxamine. Thus, patients who consume high quantities of caffeine-containing beverages should lower their intake when fluvoxamine is administered and adverse caffeine effects (like tremor, palpitations, nausea, restlessness, insomnia) are observed. CYP3A4 When combined with fluvoxamine, plasma concentrations of cisapride may be increased resulting in an increased risk of QT-prolongation/Torsade de Pointes. Therefore, fluvoxamine should not be co-administered with cisapride. The plasma concentrations of benzodiazepines metabolised by oxidation (such as triazolam, midazolam, alprazolam and diazepam) are likely to increase when co-administered with fluvoxamine. For benzodiazepines metabolised by glucuronidation (lorazepam, lormetazepam, oxazepam, temazepam) or nitro-reduction (clonazepam, nitrazepam) such an effect is not likely to occur. Increased serum concentrations of haloperidol have also been reported after concomitant use of haloperidol and fluvoxamine.
Patients co-administered fluvoxamine and CYP3A4 metabolised drugs with a narrow therapeutic index (e.g. cyclosporin, methadone, or carbamazepine) should be carefully monitored and, if necessary, dose adjustments of these drugs is recommended. CYP2C Patients co-administered fluvoxamine and CYP2C metabolised drugs with a narrow therapeutic index (such as phenytoin) should be carefully monitored and, if necessary, dose adjustments of these drugs is recommended.
Faverin – Product information
Other No interactions were seen with digoxin or atenolol, which are renal y excreted. After a single oral dose, fluvoxamine plasma concentrations were lower in smokers than in non- smokers. Effects on Laboratory Tests
Rarely, treatment with fluvoxamine has been associated with an increase in hepatic enzymes, mostly accompanied by clinical symptoms. In these cases, treatment should be discontinued. Effects on other laboratory tests have not been established. Adverse Reactions Nausea, sometimes accompanied by vomiting, is the most frequently observed symptom associated with fluvoxamine treatment. This side effect usually diminishes within the first two weeks of treatment. Other adverse events, observed in clinical studies at frequencies listed below (database size approx - 35,000 patients; dose range 50-300mg/day), are often associated with the illness and are not necessarily related to treatment.
Events are listed within body systems and categorised by frequency according to the following definitions:
Uncommon (frequency ≥ 0.1% and < 1 %)
Rare (frequency ≥ 0.01% and < 0.1 %)
Common - Agitation, anxiety, dizziness, insomnia, nervousness, somnolence,
Uncommon - Ataxia, confusion, extrapyramidal symptoms, hal ucinations
Common - Abdominal pain, anorexia, constipation, diarrhoea, dry mouth,
Uncommon - Abnormal (delayed) ejaculation
Faverin – Product information
Symptoms, including paraesthesia, headache, nausea, dizziness and anxiety, have been rarely reported after abrupt discontinuation of fluvoxamine. Post-marketing data As with other SSRIs, hyponatraemia has been rarely reported with fluvoxamine and appeared to be reversible when fluvoxamine was discontinued. Some cases were probably due to the syndrome of inappropriate antidiuretic hormone secretion. The majority of reports were associated with older patients. Haemorrhage, ecchymoses, purpura and gastrointestinal bleeding have been reported (see “Precautions”). Changes in weight (weight gain or weight loss) have also been reported. Very rarely, paresthesia and taste perversion have been reported. Urogenital:
Uncommon – cutaneous hypersensitivity reaction (including angioedema).
Other Adverse Events in OCD Paediatric Population In paediatric patients (N=57) treated with fluvoxamine the overall profile of adverse events was generally similar to that seen in adult studies. However the following events not appearing above have been reported in two or more of the paediatric patients and were more frequent with fluvoxamine than placebo: abnormal thinking, cough increase, dysmenorrhoea, emotional lability, epistaxis, hyperkinesia, infection and sinusitis. Dosage and Administration
Depression
The recommended starting dose of fluvoxamine is 50mg per day for one week, given as a single dose in the evening. Doses should be gradually increased (by 50mg per week) until an effective dose is reached, with a maximum of 300mg per day. (The usually effective dose is 100mg/day.) Doses up to 150mg can be given as a single dose. It is recommended that total daily doses of greater than 150mg be given in 2 or 3 divided doses. If no improvement is observed within 6 weeks of initiation of therapy, treatment with fluvoxamine should be reconsidered. It is important to ascertain that an adequate therapeutic dose has been maintained throughout this period. In agreement with the consensus statement of the WHO, antidepressant medication should be continued for at least 6 months after recovery from a depressive episode. Obsessive Compulsive Disorder
Adults: The recommended starting dose of fluvoxamine is 50mg per day for 3 to 4 days. The dosage should be increased gradually (i.e. by 50mg every 4 to 6 days) until an effective dose is achieved, with a maximum of 300mg per day. (The usually effective dose is in the range of 100-300mg/day.) Doses up to 150mg per day can be given as a single dose, preferably in the evening. It is recommended that a total daily dose of more than 150mg is given in 2 or 3 divided doses. Faverin – Product information
Children and adolescents (8-17 years): The recommended starting dose of fluvoxamine in paediatric populations (ages 8-17 years) is 25mg administered as a single daily dose at bedtime. In a controlled clinical trial establishing the effectiveness of FAVERIN in OCD, paediatric patients (ages 8-17) were titrated within a dose range of 50 to 200mg/day. The dose should be increased in 25mg increments every 4 to 7 days, as tolerated, until maximum therapeutic benefit is achieved. Physicians should consider age and gender differences when dosing paediatric patients. The maximum dose should not exceed 200mg/day. Therapeutic effect in female children may be achieved with lower doses. It is advisable that a total daily dose of more than 50mg should be given in two divided doses. If the two divided doses are not equal, the larger dose should be given at bedtime. If a good therapeutic response is achieved, treatment can be continued at the required dosage. There are no systematic studies which address the issue of the length of treatment. However, since obsessive compulsive disorder (OCD) is a chronic condition, it is reasonable to consider continuation beyond 10 weeks in responding patients. Data from the long-term (up to two years) open-extension phase of the placebo-controlled study in children supports sustained efficacy of the medicine. Dosage adjustments should be made carefully, on an individual patient basis, throughout therapy to maintain the patient at the lowest effective dose. The need for treatment should be reassessed periodically. Some clinicians advocate concomitant behavioural psychotherapy in conjunction with pharmacotherapy. If no improvement is observed within 10 weeks of initiation of therapy, treatment with fluvoxamine should be reconsidered. It is important to ascertain that an adequate therapeutic dose has been maintained throughout this period. Administration
FAVERIN (fluvoxamine maleate) tablets should be swallowed with water, without chewing. Discontinuation
At daily doses of 200mg or higher fluvoxamine should not be abruptly discontinued or reduced. It is recommended to reduce the daily dosage by 100mg every 3 days. Overdosage
Symptoms
The most common symptoms of overdose include gastrointestinal complaints (nausea, vomiting and diarrhoea). Somnolence and dizziness, cardiac events (tachycardia, bradycardia, hypotension), liver function disturbances, convulsions and coma have also been reported. More than 300 cases of deliberate overdosage with fluvoxamine have been reported to date. The highest documented dose of fluvoxamine ingested by a patient is 12 gram. This patient recovered completely. Occasionally, more serious complications have been observed in cases of deliberate overdosage of fluvoxamine in combination with other drugs. Six deaths due to an overdose of fluvoxamine alone have been reported. Faverin – Product information
Treatment
There is no specific antidote to fluvoxamine. Treatment should consist of general measures employed in the management of overdose along with general symptomatic and supportive measures. Presentation
FAVERIN (fluvoxamine maleate) 50mg: round, biconvex, scored white film-coated tablets inscribed with ‘S’ on one side and ‘291’ on the other, on either side of the score, in packs of 60, 30, and 10 (sample pack). FAVERIN (fluvoxamine maleate) 100mg: oval, biconvex, scored, white film-coated tablet, inscribed with ‘S’ on one side and ‘313’ on the other, on either side of the score, in packs of 30, and 10 (sample pack). 50mg Tablets:
Storage Conditions
Store below 25oC. Keep out of the reach of children. Sponsor
Sigma Pharmaceuticals (Australia) Pty Ltd 96 Merrindale Drive Croydon VIC 3136 Text approved by the Therapeutic Goods Administration: 11 July 2002 Date of most recent amendment: 19 November 2009
ALBENDAZIVEN COMPOSICIÓN: Albendazol, 19 mg; Excipiente, c.s.p. 1 ml. PROPIEDADES FARMACOLÓGICAS: El Albendazol es un potente antihelmíntico que presenta un amplio espectro de actividad y un margen de seguridad terapéutica elevado. De administración única, es compatible con otros tratamientos. ESPECIES DE DESTINO: Bovino, ovino y caprino. INDICACIONES: En ovino
RESUME DES CARACTERISTIQUES DU PRODUIT La titration de la dose doit être progressive, étant donné qu’il peut s’écouler environ 2 semaines avant que l’effet antihypertenseur maximal ne soit apparent. DENOMINATION DU MEDICAMENT Certains individus n’obtenant pas un contrôle tensionnel adéquat avec un seul agent Lercanidipine Mylan 10 mg comprimés pelliculés antihypertenseu