Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
295_298 emin alioglu
Türk Kardiyol Dern Arfl - Arch Turk Soc Cardiol 2007;35(5):295-298
Sol ventrikül yerleflimli kist hidatik: Olgu sunumu
Emin Alio¤lu, M.D., U¤ur Önsel Türk, M.D., ‹stemihan Tengiz, M.D., Ertu¤rul Ercan, M.D.
Department of Cardiology, Central Hospital, ‹zmir
Cardiac hydatid disease is uncommon, occurring in
Kardiyak hidatik hastal›¤› nadirdir ve ekinokokkosizli
0.2% to 2% of patients with echinococcal disease. A 67-
tüm hastalar›n %0.2-%2’sinde görülür. Altm›fl yedi ya-
year-old farmer presented with fatigue, dyspnea, and
fl›nda bir çiftçi bitkinlik, nefes darl›¤› ve çarp›nt› yak›n-
palpitations. He had no previous history of heart dis-
malar›yla baflvurdu. Öyküsünde kalp hastal›¤› yoktu.
ease. Cardiovascular examination, electrocardiography,
Kardiyovasküler muayenesi, elektrokardiyografi, gö-
chest X-ray, hematologic and biochemical tests were
¤üs filmi, hematolojik ve biyokimyasal testleri normal
normal. Parasitic serology was negative. Transthoracic
bulundu. Parazitik serolojisi negatif idi. Transtorasik
echocardiograpy showed a cyst, measuring 3.7x3.5 cm,
ekokardiyografide sol ventrikülün posteroapikal bölge-
in the posteroapical region of the left ventricle. Magnetic
sinde 3.7x3.5 cm boyutlar›nda bir kist görüldü. Kist
resonance imaging confirmed the cardiac cyst and
varl›¤› magnetik rezonans görüntüleme ile do¤ruland›
showed another cyst in the liver. The patient underwent
ve karaci¤erde ikinci bir kiste rastland›. Hastaya me-
surgery through median sternotomy and the cyst was
dian sternotomiyle cerrahi uygulanarak kist ç›kar›ld›.
removed. Pathologic examination confirmed the diagno-
Patolojik incelemede ekinokokkosiz tan›s› do¤ruland›.
sis of echinococcosis. Postoperatively, the patient was
Ameliyat sonras›nda hastaya dört haftal›k albendazol
treated with albendazole (800 mg/day) for four weeks.
tedavisi (800 mg/gün) uyguland›. Üç ayl›k takip süre-
At three-month follow-up, the patient was asympto-
sini hasta asemptomatik geçirdi, fonksiyonel kapasite-
matic, with improved functional capacity. Two-dimen-
sinde düzelme görüldü. ‹kiboyutlu transtorasik eko-
sional transthoracic echocardiography showed no signs
kardiyografide kist oluflumunu düflündürür bir bulgu
Key words: Cardiomyopathies; echinococcosis/surgery; hydatid
Anahtar sözcükler: Kardiyomiyopati; ekinokokkosiz/cerrahi, hi-
Echinococcosis is a tissue infection in humans
myocardium via the coronary arteries and may be
caused by the larval stage of Echinococcosis gran-
either confined solely to the heart or associated
ulosus and E. multilocularis. Canines are the hosts
with involvement of other organs.[2] The left ven-
for E. granulosus. Hydatid disease is endemic in
tricular wall is the most frequent site, but the inter-
cattle-raising areas of the world including
ventricular septum, right ventricle, and left or right
Mediterranean countries and the Middle East. The
atrium may also be involved.[3] Major complica-
incidence of hydatidosis in the Turkish population
tions of cardiac hydatid disease result from rupture
has been reported as 1:20,000.[1] Theoretically,
of the cyst either into the heart or pericardium and
echinococcosis can involve any organ, the liver
death may occur subsequent to anaphylactic shock,
being the most common, followed by the lungs.
cardiac tamponade, and systemic or pulmonary
These two organs account for 90% of all cases.
embolization. When echinococcosis is diagnosed,
Cardiac involvement is infrequent, accounting for
surgery is the treatment of choice for even asymp-
0.2% to 2%. It is caused by the invasion to the
tomatic cases due to the risk for cystic rupture.[1]
Received: December 8, 2006 Accepted: January 24, 2007Correspondence: Dr. Emin Alio¤lu. ‹zmir Central Hospital, 1644 Sok., No: 2/2, 35050 Bayrakl›, ‹zmir. Tel: 0232 - 341 67 67 Fax: 0232 - 341 68 68 e-mail: dreminalioglu@yahoo.com
ventricle, right ventricular hydatid cysts have a high-
A 67-year-old farmer complained of fatigue, dysp-
nea, and palpitations. He had no previous history of
Other manifestations of cardiac echinococcosis
heart disease. Cardiovascular examination revealed
may result from mechanical compression exerted by
no abnormal findings. His electrocardiogram and
the cyst on neighboring tissues, including myocardial
chest radiograph, and hematologic and biochemicaltests were normal. Parasitic serology was negative.
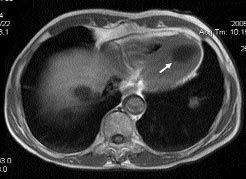
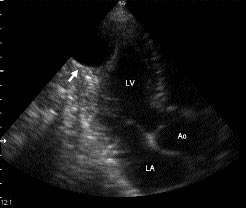
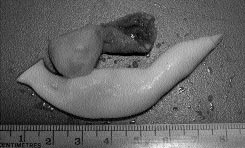
Transthoracic two–dimensional echocardiograpyshowed a cyst, measuring 3.7x3.5 cm, localized inthe posteroapical region of the left ventricle (Fig. 1a). Magnetic resonance imaging confirmed the cardiaccyst and showed another cyst in the liver (Fig. 1b). Transesophageal echocardiography showed an ovoidcavitated mass with internal areas of calcification andconfirmed the absence of additional cysts in the car-diac chambers. Selective coronary angiographyrevealed no significant lesions. The patient under-went surgery through median sternotomy. Standardcardiopulmonary bypass techniques were used withmoderate hypothermia and cardioplegic arrest. Thecyst was reached via a left ventriculotomy andremoved (Fig. 2). Hypertonic saline (10% NaCl) wasused as a scolicidal agent. Pathologic examination
confirmed the diagnosis of echinococcosis. Thepatient was discharged on the sixth postoperative dayand treated with albendazole (800 mg/day for 4weeks). At three-month follow-up, the patient wasasymptomatic, with improved functional capacity. Two-dimensional transthoracic echocardiographyshowed no signs of cystic formation.
Cardiac hydatid disease is very rare, occuring inapproximately 0.2% to 2% of patients with hydatiddisease.[4] Cardiac hydatid cysts develop in manyparts of the heart such as the left ventricle (55-71%),right ventricle (13-18%), interventricular septum (5-
Figure 1. (A) Transthoracic echocardiographic apical view.
13%), right atrium (2-4%), and left atrium (8%).[5,6]
(B) Magnetic resonance image showing hydatid cysts locatedin the left ventricular apex and in the liver.
Several hypotheses have been proposed for thepredilection for left ventricular location, includingdominance of the left coronary artery, better condi-tions of the left ventricular myocardial mass for par-asitic development, and different pressure regi-mens.[7]
Clinical manifestations of cardiac cysts are broad,
ranging from asymptomatic patients to sudden death. Symptoms depend on the location, size, and integrityof the cyst. Embolization, anaphylactic shock, andcardiac tamponade are the most serious and oftenlethal complications.[8] Cysts have the potential forintracardiac or intrapericardial ruptures. Although
Figure 2. Macroscopic view of the excised hydatoid material
hydatid cysts are more frequently located in the left
ischemia; disturbances of the cardiac rhythm; and
asymptomatic patients in order to prevent rupture.
valve malfunction. Three main symptoms that suggest
However, surgical intervention may result in seri-
the presence of an uncomplicated cyst are chest pain,
ous complications.[13] Whether the treatment should
dyspnea, and palpitations. With chest pain, the severity
be medical or surgical remains controversial.[14] It is
and the site are variable, although it is often a perma-
important to consider the localization, number, and
nent or recurrent precordial pain. Sometimes the pain
size of the cysts in choosing the treatment method.
resembles angina pectoris suggesting coronary disease,
Medical therapy with albendazole results in disap-
or myocardial infarction when it is severe. These palpi-
pearance of extracardiac hydatid cysts in up to
tations may arise from ventricular extrasystoles, parox-
48%, and reduction in size in 24%. However, the
ysmal ventricular tachycardia, and conduction disor-
specific efficacy of albendazole against cardiac
ders that may lead to a complete atrioventricular block
hydatid cysts has not been established.
with bradycardia and Adams-Stokes attack, which are
Antihelmintics have been recommended in inoper-
typical of the septal location of a cyst.
able cases or as adjuvant therapy[15] when there is
The diagnosis of a cardiac cyst is probable in
patients with a history of echinococcosis in another
Surgical approach is not recommended for peri-
organ. In the absence of any diagnostic sign, routine
cardial hydatid cysts. Percutaneous aspiration and
investigations by specific cardiac imaging proce-
instillation of ethanol or silver nitrate after pretreat-
ment with albendazole (800 mg/day for 4 weeks) is
Chest radiographic findings are usually reliable.
The chest X-ray may reveal localized or global
deformations and calcifications of the cardiac out-
1. Salih OK, Celik SK, Topcuoglu MS, Kisacikoglu B,
line. The typical image is a calsified, well-limited,
Tokcan A. Surgical treatment of hydatid cysts of the
and sessile lobular mass with clear edges.[10]
heart: a report of 3 cases and a review of the literature.
Nonspecific electrocardiographic abnormalities
such as T-wave inversion, ST-depression, prema-
2. McManus DP, Zhang W, Li J, Bartley PB.
ture ventricular beats, incomplete or complete bun-
Echinococcosis. Lancet 2003;362:1295-304.
dle branch block, and supraventricular tachycardia
3. Kardaras F, Kardara D, Tselikos D, Tsoukas A,
are present in more than 80% of patients.[8] In older
Exadactylos N, Anagnostopoulou M, et al. Fifteen year
patients, it is often more difficult to establish the
surveillance of echinococcal heart disease from a refer-
differential diagnosis between acute coronary dis-
ral hospital in Greece. Eur Heart J 1996;17:1265-70.
ease and cardiac hydatid cyst disease. In young
4. Eckert J, Deplazes P. Biological, epidemiological, and
patients, especially in the presence of a Q wave of
clinical aspects of echinococcosis, a zoonosis of increas-
necrosis the diagnosis of a cardiac hydatid cyst
ing concern. Clin Microbiol Rev 2004;17:107-35.
should be considered. This Q wave is due to the
5. Sensoz Y, Ozkokeli M, Ates M, Akcar M. Right ven-
electrical window formed by a transmural cyst.
tricle hydatid cyst requiring tricuspid valve excision. Int J Cardiol 2005;101:339-41.
Conduction disorders may also be associated with a
6. Kunt AS, Aydin S, Demir D, Selli C, Andac MH. Left
ventricle wall hydatid cyst. Kalp Damar Cer Derg
Hematology may reveal eosinophilia of a varying
degree. Serological tests including indirect hemag-
7. Thameur H, Abdelmoula S, Chenik S, Bey M, Ziadi
glutination and latex agglutination tests are useful if
M, Mestiri T, et al. Cardiopericardial hydatid cysts.
positive, but many cyst carriers will not develop an
immune response.[11] Diagnosis of cardiac hydatid
8. Bashour TT, Alali AR, Mason DT, Saalouke M.
cysts is often made using transthoracic echocardiog-
Echinococcosis of the heart: clinical and echocardio-
raphy. Transesophageal echocardiography provides
graphic features in 19 patients. Am Heart J 1996;132:
details of the cyst.[12] Computed tomography and
magnetic resonance imaging may provide valuable
9. De Paulis R, Seddio F, Colagrande L, Polisca P,
Chiariello L. Cardiac echinococcosis causing coronary
information, but two-dimensional echocardiography
artery disease. Ann Thorac Surg 1999;67:1791-3.
10. Tengiz I. Cardiac hydatid cysts. J Card Resc 2006;1:1-5.
Surgical excision is the definitive method of
11. Charet E, Roudaut R, Lafitte S, Laffort P, Madonna F, de
treatment for cardiac hydatid cysts, even for
Mascarel A. Echocardiographic demonstration of rupture
of intraseptal hydatid cyst. J Am Soc Echocardiogr 2000;
14. Akar R, Eryilmaz S, Yazicioglu L, Eren NT, Durdu S,
Uysalel A, et al. Surgery for cardiac hydatid disease: an
12. Tufan Tükek, fieref Demirel, Dursun At›lgan, Ertan
Anatolian experience. Anadolu Kardiyol Derg 2003;3:
Onursal, Ferruh Korkut. Kardiak kist hidatik tan› ve
tedavisinde transözofageal ekokardiyografinin önemi:
15. Simeunovic D, Seferovic PM, Ristic AD, Petrovic P,
iki vaka nedeni ile literatürün gözden geçirilmesi. Türk
Maisch B. Pericardial cysts: incidence, clinical presen-
tations and treatment. In: Seferovic PM, Spodick DH,
13. Kaplan M, Demirtas M, Cimen S, Ozler A. Cardiac
Maisch B, editors. Pericardiology: comtemporary
hydatid cysts with intracavitary expansion. Ann
answers to continuing challenges. Belgrade: Science
No. 06-1249 In the Supreme Court of the United States On Petition for a Writ of Certiorari to the Vermont Supreme Court BRIEF OF AMICI CURIAE PRODUCT LIABILITY ADVISORY COUNCIL, INC. AND U.S. CHAMBER OF COMMERCE IN SUPPORT OF PETITIONER Washington, DC 20006(202) 263-3000 1615 H Street, N.W. Washington, D.C. 20062 TABLE OF CONTENTS The Decision Below Thwarts Important
LUKE NIELSON Education University of Wyoming College of Business: Marketing Major Anticipated Graduation Date: May 2013 Courses Studied: Accounting, Economics, Information Management Systems, Business Calculus Western Wyoming Community College Associate of Arts in General Studies & Certificate in Digital Design Technologies Cumulativ
 ventricle, right ventricular hydatid cysts have a high-
A 67-year-old farmer complained of fatigue, dysp-
nea, and palpitations. He had no previous history of
Other manifestations of cardiac echinococcosis
heart disease. Cardiovascular examination revealed
may result from mechanical compression exerted by
no abnormal findings. His electrocardiogram and
the cyst on neighboring tissues, including myocardial
chest radiograph, and hematologic and biochemicaltests were normal. Parasitic serology was negative.
ventricle, right ventricular hydatid cysts have a high-
A 67-year-old farmer complained of fatigue, dysp-
nea, and palpitations. He had no previous history of
Other manifestations of cardiac echinococcosis
heart disease. Cardiovascular examination revealed
may result from mechanical compression exerted by
no abnormal findings. His electrocardiogram and
the cyst on neighboring tissues, including myocardial
chest radiograph, and hematologic and biochemicaltests were normal. Parasitic serology was negative.