Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Thegynaecologygroup.co.uk
medical education case study Management of chronic pelvic pain This case of persistent pelvic pain illustrates the multifactorial nature of the condition. By Mr Philip Kaloo
well as the probable findings (recurrent endometriosis and
case study
pelvic adhesions) and the risk of complications. Laparoscopy
Miss aP, a 28-year-old nulliparous woman, presented to the
showed significant large bowel adhesions in the right iliac fossa/
pelvic pain/endometriosis clinic in 2008 with a four-year
flank (figure 1) and an adherent right ovary to the pelvic side
history of right-sided pelvic pain. the pain was intermittent in
wall and posterior aspect of the uterus (figure 2). The pelvis was
nature, rated as nine out of 10 at worst, and associated with
otherwise normal, with no obvious endometriosis or evidence of
the patient described the pain as burning and stabbing,
The bowel adhesions were divided laparoscopically and the
requiring bed rest and tramadol analgesia when at its worst.
right ovary was mobilised from the pelvic side wall. Meticulous
She had no significant urinary or bowel symptoms. triple swabs
haemostasis was ensured. In addition, 500ml icodextrin
had previously been taken and were negative for chlamydia. In
instillate was left within the abdominal cavity with the object of
addition, she experienced significant deep dyspareunia and
worsening dysmenorrhoea within an otherwise regular cycle.
Preoperatively, the abdominal trigger point was marked on
She used the combined oral contraceptive pill and was up to
the abdominal wall and local anaesthetic and steroid were
instilled intraoperatively in an attempt to deal with the
Miss aP had a history of endometriosis diagnosed by
neuropathic pain element of her symptoms.
laparoscopy in 2000, with a subsequent right ovarian
At three-month follow-up, Miss AP rated her abdominal pain
cystectomy via a transverse laparotomy in 2004.
as three out of 10 at worst and her deep dyspareunia was now a
‘minor problem’. She still had a mildly positive Carnett’s test and
What is the diagnosis and management?
subsequently had a repeat local anaesthetic infiltration to her
trigger point. She was offered psychological support for her
Chronic pain is described by the International Association for
At six-month follow-up, Miss AP rated her abdominal pain as
the Study of Pain as an unpleasant sensory and emotional
two out of 10. Her deep dyspareunia persisted but remained a
experience associated with actual or potential tissue damage.
‘minor’ problem. She stated that she was very happy with the
The incidence in UK general practice is similar to that for
migraine, back pain and asthma, at 21.5 per 1,000 consultations.1
Chronic pelvic pain is usually multifactorial. It can be constant discussion
or intermittent and can last more than six months. Postoperative This case is an example of how chronic pain can often be
adhesions are common and may cause pelvic pain. Endometriosis multifactorial in nature. Although Miss AP had clinical
and irritable bowel syndrome are common copathologies.
evidence of nerve entrapment, she was considered to be highly
Carnett’s test2 can help to differentiate between abdominal
likely to have additional pelvic pathology in view of her
wall and intra-abdominal pathology. This test for nerve
entrapment involves palpating the area of maximal abdominal
Nerve entrapment is not uncommon following a Pfannenstiel
tenderness with the patient supine, then asking them to tense
incision (3.7 per cent)3 and to a lesser extent, laparoscopic
their abdominal wall by lifting their head off the couch. If nerve
surgery. Such peripheral neuropathic pain may also occur de
entrapment within the abdominal wall is present, tensing the
novo and up to 10 per cent of patients with suspected GI
muscles usually leads to increasing pain (a positive test). If pain
pathology actually have abdominal wall ‘pathology’.4
is reduced, this may suggest intra-abdominal pathology, the
The early diagnosis of this pathology could prevent
splinting effect of the muscles ‘protecting’ the affected organs.
unnecessary gynaecological or GI intervention. Carnett’s test is a
useful way to help triage patients in primary or secondary care. examination and investigation
Adhesions following surgery can lead to significant
In Miss AP’s case, abdominal examination elicited pain in the
morbidity and recently, increasing litigation.5 They are
right iliac fossa without evidence of peritonism. Carnett’s test
predominantly a result of extensive and/or open surgery but
was positive superior to the right lateral edge of her laparotomy
may occur after any operative procedure.6
incision. Vaginal examination elicited the same localised
There is uncertainty as to the true benefit of adhesiolysis, but
tenderness in the right adnexal region, but with no cervical
a Cochrane review suggests it is only beneficial when severe
excitation. Musculoskeletal examination by a women’s health
adhesions are present.7 Anecdotally, many patients find
significant relief with adhesiolysis of firm adhesions, especially
Pelvic ultrasound revealed a normal uterus and ovaries, but
when they cause reduced organ mobility.
marked tenderness in the right adnexal region. Chlamydia PCR
persistent pelvic pain Despite the identification and treatment of possible causes of management and follow-up
pelvic pain, its persistence is not uncommon. A common
A laparoscopy was offered and Miss AP accepted, having been
cause of persisting pain is chronic overstimulation of sensory
counselled about the possibility of a ‘negative’ laparoscopy, as
nerves from the viscera to the spinal cord. Such persisting
42 MIMS woMen’S health vol 4, no 4, 2009 www.healthcarerepublic.com/wh figure 1: Laparoscopy showing significant large bowel adhesions figure 2: the right ovary is shown to be adherent to the pelvic in the right iliac fossa side wall and to the posterior aspect of the uterus
stimulation causes permanent alteration in neuronal
box 1: chronic pelvic pain management
function (neuroplasticity), leading to hyperalgesia (excessive
sensitivity to pain) or allodynia (pain from stimuli that are not
the basic rationale behind the management of chronic pelvic pain is as follows:11-13
Such pain can be difficult to manage but neuromodulators
such as amitriptyline, pregabalin, gabapentin and carbamazepine
● treat pain with, for example, nSaIDs and antispasmodics
have been shown to be beneficial. Hormonal manipulation,
● hormonal manipulation with the combined oral
psychological support and TENS, among other interventions,
contraceptive pill, progesterone, gnrh analogues
● neuromodulation can be effected with, for example,
amitriptyline, pregabalin, gabapentin or carbamazepine
the negative laparoscopy
● Multidisciplinary approach involving gynaecologist,
It is imperative that all patients undergoing a laparoscopy for
anaesthetist, physiotherapist, psychologist
chronic pelvic pain have the likely findings discussed, including
a ‘negative’ finding. A negative laparoscopy, that is, one in which
no definitive aetiology is visible, may occur in up to half of
5. Ellis H. Medicolegal consequences of adhesions. Hosp Med 2004;
procedures. This can be seen as ‘positive’, in that there is no
visible pathology but it is important to reassure patients that
6. Lower AM, Hawthorn RJ, Clark D et al. Adhesion-related
although it is not visible, there is still a cause for their pain.
readmissions following gynaecological laparoscopy or laparotomy in
The aetiology of chronic pelvic pain is usually multifactorial.
Scotland. Hum Reprod 2004; 19: 1877-85.
Despite treatment, it can often persist. Patients have better
7. Stones W, Cheong YC, Howard FM. Interventions for treating
outcomes if an integrated multidisciplinary approach (see box 1)
chronic pelvic pain in women. Cochrane Database Syst Rev 2005,
is adopted, involving clinicians who are experienced in the
Issue 1. Art No: CD000387. DOI: 10.1002/14651858.CD000387.8. Wiffen PJ, McQuay HJ, Rees J et al. Gabapentin for acute and Mr Philip Kaloo is consultant obstetrician and gynaecologist and chronic pain. Cochrane Database Syst Rev 2005, Issue 3. Art No: runs the endometriosis/pelvic pain clinic at cheltenham General CD005452. DOI: 10.1002/14651858.CD005452. Hospital, Gloucestershire NHs trust 9. Nnoaham KE, Kumbang J. Transcutaneous electrical nerve stimulation (TENS) for chronic pain. Cochrane Database Syst Rev 2008, Issue 2. Art No: CD003222. DOI: 10.1002/14651858.RefeReNces 10. Dworkin RH, O’Connor AB, Backonja M et al. Pharmacologic 1. Zondervan KT, Yudkin PL, Vessey MP et al. Prevalence and management of neuropathic pain. Pain 2007; 132: 237-51.incidence of chronic pelvic pain in primary care: evidence from a 11. Royal College of Obstetricians and Gynaecologists. The initial national general practice database. Br J Obstet Gynaecol 1999; 106: management of chronic pelvic pain. RCOG Guideline 41. London, 2. Carnett JB. Intercostal neuralgia as a cause of abdominal pain and 12. Jarrell JF, Vilos GA, Allaire C et al. Consensus guidelines for the tenderness. Surg Gynecol Obstet 1926, 42: 625-32.management of chronic pelvic pain. J Obstet Gynaecol Can 2005; 3. Perry CP. Peripheral neuropathies causing chronic pelvic pain. J Am Assoc Gynecol Laparosc 2000; 7: 281–7.13. American College of Obstetricians and Gynecologists Committee 4. Srinivasan R, Greenbaum DS. Chronic abdominal wall pain: a on Practice Bulletins – Gynecology. ACOG Practice Bulletin No. 51. frequently overlooked problem. Am J Gastroenterol 2002; 97: 824-30.Chronic pelvic pain. Obstet Gynecol 2004; 103: 589-605.www.healthcarerepublic.com/wh
MIMS woMen’S health vol 4, no 4, 2009 43
Association des Disciplines Orthodontiques et Maxillo-Faciales Le chirurgien maxillo-facial peut réaliser les extractions dentaires difficiles. - cas de dent dévitalisée et ankylosée. - cas d'extractions dents multiples. - présence de kyste plus ou moins volumineux attenant aux dents. - risques de complications hémorragiques du fait de traitement anti-agrégant (Aspégic®, Kardégic®, P
Clinical Chemistry 56:10 1528–1534 (2010) Clinical Chemistry Guide to Scientific Writing Bring Your Best to the Table Sometime in the past you were likely taught about thetext (e.g., mass transitions for 20 different drugs beingimportance of “bringing your best to the table”—inother words contributing your best ideas and results. A good table, although used for a purpose
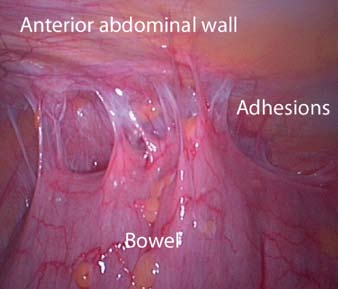
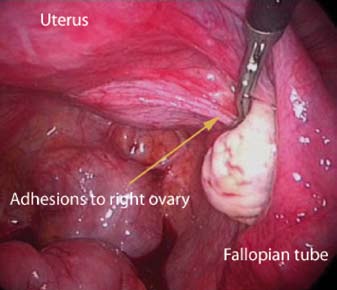 figure 1: Laparoscopy showing significant large bowel adhesions
figure 1: Laparoscopy showing significant large bowel adhesions