Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Doi:10.1016/j.humimm.2004.09.014
Severe, Late-onset Graft-Versus-Host Disease in a Liver Transplant Recipient Documented by Chimerism Analysis Marilyn S. Pollack, Kermit V. Speeg, Natalie S. Callander, Cesar O. Freytes, Alfredo A. Espinoza, Robert M. Esterl, Gregory A. Abrahamian, W. Kenneth Washburn, and Glenn A. Halff ABSTRACT: A 52-year-old liver transplant recipient
identical brother, but he died 5 days after transplantation
presented 8 months after transplantation with oral thrush,
of overwhelming Candida kruseii infection. To our knowl-
then 3 days later with oral ulcers and a diffuse rash, and
edge, this is the first chimerism-analysis– documented
5 days later with an acutely reduced white blood cell
case of severe acute GVHD presenting so late after liver
count, rash, fever, and diarrhea. Bone marrow biopsy
transplantation. It is of note that the patient had no
revealed severe aplasia. Although graft-versus-host disease
known risks for GVHD in that he was relatively young
(GVHD) was considered, the late onset of these symptoms
and shared only one major human leukocyte antigen with
was felt to render this etiology unlikely because GVHD
his donor. Consideration should be given to GVHD as a
usually occurs 2 to 6 weeks after transplantation. All
cause of bone marrow aplasia at any time after organ
potentially myelosuppressive medications were discontin-
transplantation. Storage of cell pellets from all transplant
ued, and the patient was treated with high doses of
recipients and donors is highly recommended to facilitate
hematopoietic growth factors. Because his symptoms con-
tinued, chimerism analysis was performed, which indi-
28 –31 (2005). American Society for Histocompatibil-
cated that 96% of the peripheral blood mononuclear cells
ity and Immunogenetics, 2005. Published by Elsevier Inc.
were of liver-donor origin. Ultimately, the patient under-went an allogeneic peripheral blood hematopoietic pro-
KEYWORDS: liver transplantation; graft versus host
genitor cell transplant from a human leukocyte antigen–
ABBREVIATIONS BM INTRODUCTION
Graft-versus-host disease (GVHD) occurs when a trans-
cells that mount an immune response against recipient
plant donor’s T lymphocytes differentiate into effector
tissues. This is a frequent complication of allogeneichematopoietic progenitor cell (HPC) transplantation be-cause of the planned infusion of large numbers of immu-
From the Departments of Pathology (M.S.P), Medicine (K.V.S., N.S.C.,
nocompetent cells into an immunocompromised host. In
C.O.F., A.A.S), and Surgery (R.M.E., G.A.A., W.K.W., G.A.H.), Uni-
solid organ transplantation, GVHD is an infrequent but
versity of Texas Health Science Center, San Antonio, TX, USA.
serious complication and generally only occurs for trans-
Address reprint requests to: Dr. Marilyn S. Pollack, Department ofPathology, University of Texas Health Science Center, 7703 Floyd Curl
plants involving organs with relatively large numbers of
Drive, San Antonio, TX 78229; Tel: (210) 567-5698; Fax: (210)
passenger lymphocytes, notably for liver and intestine
358-0777; E-mail: Pollack@uthscsa.edu.
transplantation. Skin and gut manifestations of GVHD
Received June 29, 2004; revised September 24, 2004; accepted September
in liver transplant recipients resemble those observed in
Human Immunology 66, 28 –31 (2005) American Society for Histocompatibility and Immunogenetics, 2005
HPC transplant recipients, including skin rash and di-
weeks), and prednisone (5 mg daily). He had no episodes
arrhea. However, liver transplant recipients with GVHD
of rejection and had normal liver enzymes, with gradual
typically lack evidence of liver dysfunction and instead
resolution of the renal insufficiency that had predated his
have severe pancytopenia and bone marrow (BM) aplasia
not usually seen in HPC transplant recipients. The di-
At 8 months after transplant, the patient presented
agnosis of GVHD in organ transplant recipients is
with oral thrush, which was treated with fluconazole.
largely a clinical one, but recently, more sophisticated
Three days later, he presented with a sore throat, oral
testing that allows the detection of donor organ– derived
ulcers, and a diffuse rash; fluconazole therapy was
cells in affected tissue sites can confirm the clinical
stopped. His white blood cell (WBC) count, which had
suspicion and prevent institution of inappropriate ther-
been normal, was 2500/l and then acutely dropped over
apy. For example, a skin rash with infiltrating donor
the next 5 days to 0.1 l/ml, accompanied by severe
lymphocytes should probably not be treated as a drug-
anemia and thrombocytopenia. The patient was admitted
induced toxicity with concomitant reduction of a partic-
with a 1-day history of temperature to 40°C, diffuse
maculopapular rash, diarrhea, and abdominal pain. Blood
The primary risk factor for the development of
cultures were negative, as were tests for cytomegalovirus.
GVHD in organ transplant recipients is considered to be
A BM biopsy on the second hospital day revealed no
a relatively low degree of human leukocyte antigen
aspirable elements and an overall cellularity of 10%.
(HLA) mismatching between the donor and recipient,
Special stains for mycobacteria and fungi were negative.
such as in cases of related-donor (usually parent to child)
Although GVHD was considered, the majority of the
liver transplants or donors homozygous for antigens at
staff believed that the long interval between transplan-
most or all HLA loci. A recent meta-analysis of
tation and the patient’s presentation made GVHD un-
factors increasing the risk for GVHD concluded that in
likely. Instead, it was believed that the rash and marrow
addition to low HLA mismatching, a relatively large age
aplasia were a result of drug therapy including valgan-
discrepancy (Ͼ40 years) between donor (younger) and
ciclovir and Septra. Both of those drugs were discontin-
recipient (older) and recipient age over 65 years were
ued, and he was treated with broad-spectrum antibiotics
contributing risk factors, presumably as a result of loss of
and large doses of erythropoietin and Filgrastim. Because
immune responsiveness (against donor lymphocytes) as a
he clinically stabilized, he was discharged to home with
function of age. Organ transplant–related GVHD has
oral antibiotics and growth factors.
only been documented to occur for the first time within
The patient was subsequently readmitted 5 days later
the first few months after organ transplantation
with recrudescence of the rash and fever. Meanwhile, a
when immunosuppression of the recipient is at its high-
skin biopsy that had been performed during his first
est level and presumably because donor lymphocytes
admission was read by a hematopathologist as consistent
surviving beyond that time have become tolerant to
with grade II GVHD. Chimerism analysis of separated
recipient mismatches. We describe here a liver transplant
peripheral blood (PB) mononuclear cells (MNCs) and
patient presenting for the first time 8 months after
granulocytes and total BM nucleated cells (the sample
transplantation with clinical and subsequent confirma-
was too acellular to analyze separated BM MCs) was then
performed. Stored, pretransplant WBC pellets from boththe recipient and donor were available for comparison. DNA from all samples was extracted by means of a
CASE REPORT
standard Qiagen protocol. The chimerism analysis was
This case involves a 52-year-old Hispanic man, blood
done with an ABI sequencer with a Promega PowerPlex
type O positive, who received an orthotopic liver trans-
System in which ten polymorphic, single tandem repeat
plant for end-stage liver disease from alcoholic cirrhosis.
system alleles and the X versus Y chromosome marker
The donor was a 53-year-old woman, blood type O
Amelogenin were simultaneously amplified and labeled
positive, who died from a subarachnoid hemorrhage. She
with different fluorescent dyes. Polymerase chain reac-
had normal liver enzymes. All pretransplant crossmatch
tion products with different size (repeat number) poly-
tests were negative. The patient underwent an unevent-
morphisms were then separated from each other by their
ful liver transplantation with typical preparation of the
rate of migration in a capillary gel. The results indicated
organ, including perfusion with recipient blood, and was
that all systems tested were informative in one or both
discharged 7 days after surgery. According to the routine
directions and that virtually all (96%) of the
protocols at our institution, he did not receive any
PB MCs (largely lymphocytes) were of liver donor origin
antilymphocyte induction therapy, and his immunosup-
third panel). The PB granulocyte fraction was
pression over the next 8 months consisted of low-dose
75% donor, 30% recipient (data not shown). The BM
tacrolimus, mycophenolate mofetil (tapered off after 14
total nucleated cells appeared to be only 30% of donor
tation This case report illustrates that acute GVHD
can manifest for the first time many months after livertransplantation. No precipitating cause for its occurrence
could be clearly identified. There was no change in the
patient’s immunosuppressive regimen, he did not receive
any blood transfusions, and he had no evidence for any
systemic inflammatory response. The lack of any rejection
episodes was not indicative of unusual hypoimmunity be-
cause approximately 90% of the more than 120 liver
transplant recipients we treat per year at our institution
also do not experience any rejection episodes, but this is
our first case of documented GVHD. There is, however, a
theoretic possibility that, as occurs in many autoimmune
diseases, the immune response to his local fungal infectionactivated donor lymphocytes, which then became sensi-tized to shared epitopes present in noninfected recipient
origin last panel), but because the BM was soaplastic, it was presumed that the sample contained morerecipient-derived stromal cells than cells of hematopoi-etic lineage. Graft-versus-host disease was then diag-nosed as the certain cause of the BM aplasia. Surpris-ingly, an analysis of the patient and donor HLAphenotypes indicated only a single major an-tigen match (HLA-B35), with two mismatches forHLA-A, one for HLA-B, two for HLA-C, two for HLA-DR, and two for HLA-DQ.
A review of the literature indicated that both increasing
and decreasing immunosuppression have been usedsuccessfully in treating organ-transplant-related acuteGVHD, although outcomes have generally been poor,regardless of treatment, with a mortality that exceeded75% In this case, a course of OKT3 was provided astherapy for the GVHD. Although OKT3 reduced the totallymphocyte count even further, there was no recovery ofthe total WBC count, and repeat chimerism analysis in-dicated that the proportion of donor MCs remained thesame. Because the therapy with OKT3 failed to control theGVHD, the patient underwent an allogeneic PB HPCtransplant from an HLA-identical sibling after condition-ing with cyclophosphamide and antithymocyte globulin, acombination routinely used for patients undergoing HPCtransplantation for aplastic anemia. However, despite ag-gressive blood product support, total parenteral nutrition,and broad-spectrum antibiotic and antifungal therapy, thepatient by this time was severely debilitated and had beenpancytopenic for almost 2 months. He developed a dis-
Chimerism analysis 8.5 months after transplant
seminated Candida kruseii infection and died on the fifth
(during severe bone marrow (BM) aplasia). Results for four of
day after stem cell transplantation of multiorgan failure
the 11 systems tested are shown in the first panel using the
with no evidence of marrow recovery.
patient’s pretransplant peripheral blood (PB) DNA; secondpanel, donor PB DNA; third panel, the patient’s 8.5-monthposttransplant PB mononuclear cell DNA (96% donor); and
DISCUSSION
last panel, the patient’s 8.5-month posttransplant BM aspiratetotal nucleated cell DNA (30% donor). D ϭ donor-specific
Liver transplant recipients who develop acute, rapidly pro-
alleles; R ϭ recipient-specific alleles; D, R ϭ shared alleles.
gressing GVHD with large numbers of circulating donor
For allele numbers for each system, see Results for the
lymphocytes generally do so 2 to 6 weeks after transplan-
tory of hyperimmune responses. In addition, as a woman,the liver donor for our patient would also be predicted to
have relatively high immune reactivity well known, for
example, to cause a greater risk of GVHD for recipients of
female HPC transplants possibly derived from expo-
sure to alloantigens during pregnancy. Studies of other
liver transplant patients with GVHD that look for mul-tiparous female versus male donor status should be con-
Abbreviation: HLA ϭ human leukocyte antigen.
sidered to see whether that may be generally considered anadditional risk factor for the development of GVHD after
tissues. Whatever the precipitating cause, the resulting
liver transplantation. In any case, histocompatibility lab-
marrow aplasia evidently stimulated new blood cell for-
oratories are strongly encouraged to save test material from
mation from donor hematopoietic stem cells that had been
all organ transplant recipients and donors, even if their
transplanted along with the graft, because in addition to
transplant programs do not routinely request HLA typing
the donor lymphocytes, 75% of the circulating granulo-
for liver transplant recipients. The cost for long-term stor-
cytes at the time of GVHD diagnosis were of donor origin.
age of cell pellets is relatively low, and a reference labora-
Other reports of GVHD occurring late after transplan-
tory can be used if chimerism testing is not available on
tation appear to involve more easily treatable chronic
site. A rapid diagnosis of GVHD will allow early therapy,
GVHD rather than acute GVHD. One previous report
giving patients a better chance for recovery.
described recurrent GVHD in two pediatric liver trans-plant recipients at approximately 11 and 7 months after
transplantation that had first manifested at approximately
We thank Julie B. Forman and Laura M. McNeish for expert
3 and 4 months after transplantation, respectively. For
these patients, only about 3% donor cells were detected inthe PB, and both patients responded to temporary discon-
REFERENCES
tinuation of immunosuppressive therapy. Dunn et al.
1. Smith DM, Agura E, Netto G, Collins R, Levy M, Goldstein
described another child who presented 5 years after liver
R, Christensen L, Baker J, Altrabulsi B, Osowski L, McCor-
transplantation with intestinal and skin symptoms consis-
mack J, Fichtel L, Dawson DB, Domiati-Saad R, Stone M,
tent with GVHD. Her PB revealed (only) 1% male cells,
Klintmalm G: Liver transplant–associated graft versus host
but because she had received six of 16 units of unirradiated
disease. Transplantation 75:118, 2003.
blood from male donors, the diagnosis of GVHD could not
2. Pinna AD, Weppler D, Berho M, Masetti M, DeFaria W,
be attributed to liver donor lymphocytes; the patient
Kato T, Thompson J, Ricordi C, Tzakis AG: Unusual
quickly recovered after treatment with a small pulse of
presentation of graft-versus-host disease in pediatric liver
steroids. It should also be noted that a small degree of
transplant recipients: evidence of late and recurrent disease.
chimerism is often found after organ transplant for recip-
ients who do not experience any symptoms of GVHD
3. Dunn SP, Krueger LJ, Butani L, Punnett H: Late onset of
The patient described in our case report had none of the
severe graft-versus-host disease in a pediatric liver trans-plant recipient. Transplantation 71:1483, 2001.
risk factors previously associated with GVHD presentingin the first few weeks after liver transplant in that there
4. Starzl TE: Cell migration and chimerism—a unifying concept
was a high degree of HLA mismatching and the recipient
in transplantation with particular reference to HLA matchingand tolerance induction. Transplant Proc 25:8, 1993.
was relatively young. However, two other risk factorsmight be implicated in the development of his GVHD.
5. Manabe K, Donaldson PT, Underhill JA, Doherty DG,
Mieli-Vergani G, McFarlane JG, Eddleston AL, Williams R:
First, the donor was found to have an HLA phenotype
Human leukocyte antigen A-1-B8-DR3-DQ2-DPB1*0401
consistent, because of significant linkage disequi-
extended haplotype in autoimmune hepatitis. Hepatology
librium, with having the HLA haplotype that is most
frequently documented to confer a higher than normal risk
6. Chen D, Ueda R, Harding F, Patil N, Mao Y, Kkurahara C,
for hyperimmune responses that result in autoimmune
Platenburg G, Huang M: Characterization of HLA DR3/
diseases: HLA-A1, B8, DR17 (DR3), DQ2 In this
DQ2 transgenic mice: a potential humanized animal model
regard, it is intriguing that one of the two patients de-
for autoimmune disease studies. Eur Immunol 33:172, 2003.
scribed by Pinna et al. as having recurrent GVHD many
7. Remberger M, Kumlien G, Aschan J, Barkhold L, Hentschke
months after transplant also had a donor with this haplo-
P, Ljungman P, Mattsson J, Svennilson J, Ringdon O: Risk
type (population frequency less than 9%).
factors for moderate-to-severe chronic graft-versus-host dis-
Perhaps the persistence after transplantation of immuno-
ease after allogeneic hematopoietic stem cell transplantation.
responsive donor lymphocytes is associated with their his-
Biol Blood Marrow Transplant 8:674, 2002.
Chemical Descriptions for Marcellus Shale Wells The purpose of this document is to allow a better understanding of the chemistry that is commonly used in stimulating a Marcellus shale well. An explanation of the entire completion process is needed to understand the closed system in which the chemicals are injected into the fluid system and enter an isolated and specific formation. Additional doc
Clinical Bulletin Information for Health Professionals Pain in Multiple Sclerosis by Heidi Maloni, DNScc, RN, APRN, BC-ANP, CNRN, MSCN INTRODUCTION Pain is a recognized symptom of multiple sclerosis (MS), affecting as many as seventy-fivepercent of people at some time during the course of their disease.1–4 However, only twenty-five percent of those who suffer with MS pain are
 Severe, Late-onset Graft-Versus-Host
Severe, Late-onset Graft-Versus-Host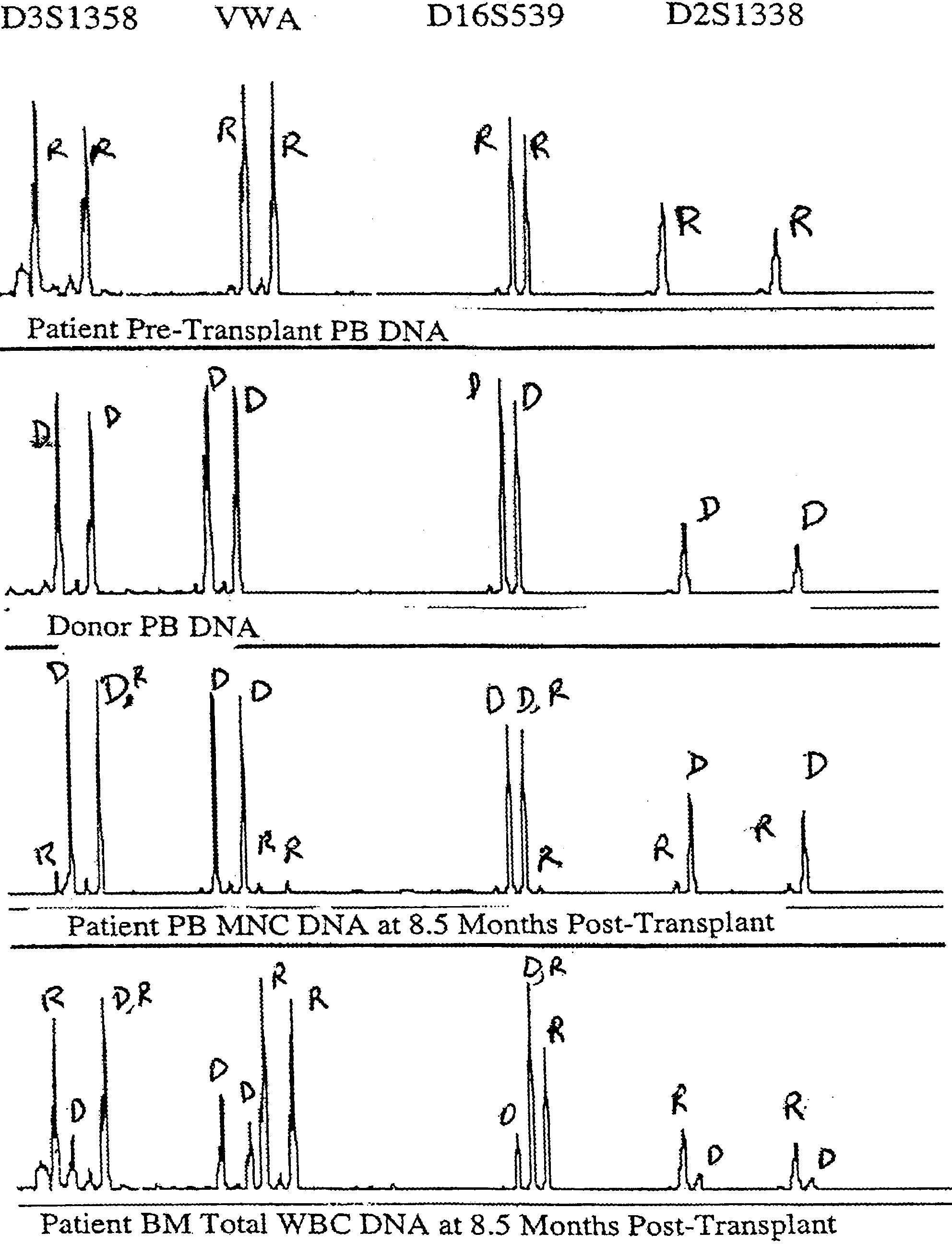 tation This case report illustrates that acute GVHD
can manifest for the first time many months after livertransplantation. No precipitating cause for its occurrence
could be clearly identified. There was no change in the
patient’s immunosuppressive regimen, he did not receive
any blood transfusions, and he had no evidence for any
systemic inflammatory response. The lack of any rejection
episodes was not indicative of unusual hypoimmunity be-
cause approximately 90% of the more than 120 liver
transplant recipients we treat per year at our institution
also do not experience any rejection episodes, but this is
our first case of documented GVHD. There is, however, a
theoretic possibility that, as occurs in many autoimmune
diseases, the immune response to his local fungal infectionactivated donor lymphocytes, which then became sensi-tized to shared epitopes present in noninfected recipient
origin last panel), but because the BM was soaplastic, it was presumed that the sample contained morerecipient-derived stromal cells than cells of hematopoi-etic lineage. Graft-versus-host disease was then diag-nosed as the certain cause of the BM aplasia. Surpris-ingly, an analysis of the patient and donor HLAphenotypes indicated only a single major an-tigen match (HLA-B35), with two mismatches forHLA-A, one for HLA-B, two for HLA-C, two for HLA-DR, and two for HLA-DQ.
tation This case report illustrates that acute GVHD
can manifest for the first time many months after livertransplantation. No precipitating cause for its occurrence
could be clearly identified. There was no change in the
patient’s immunosuppressive regimen, he did not receive
any blood transfusions, and he had no evidence for any
systemic inflammatory response. The lack of any rejection
episodes was not indicative of unusual hypoimmunity be-
cause approximately 90% of the more than 120 liver
transplant recipients we treat per year at our institution
also do not experience any rejection episodes, but this is
our first case of documented GVHD. There is, however, a
theoretic possibility that, as occurs in many autoimmune
diseases, the immune response to his local fungal infectionactivated donor lymphocytes, which then became sensi-tized to shared epitopes present in noninfected recipient
origin last panel), but because the BM was soaplastic, it was presumed that the sample contained morerecipient-derived stromal cells than cells of hematopoi-etic lineage. Graft-versus-host disease was then diag-nosed as the certain cause of the BM aplasia. Surpris-ingly, an analysis of the patient and donor HLAphenotypes indicated only a single major an-tigen match (HLA-B35), with two mismatches forHLA-A, one for HLA-B, two for HLA-C, two for HLA-DR, and two for HLA-DQ.