Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Fibromyalgia syndrome (chronic widespread pain)
Fibromyalgia Syndrome (Chronic Widespread Pain)
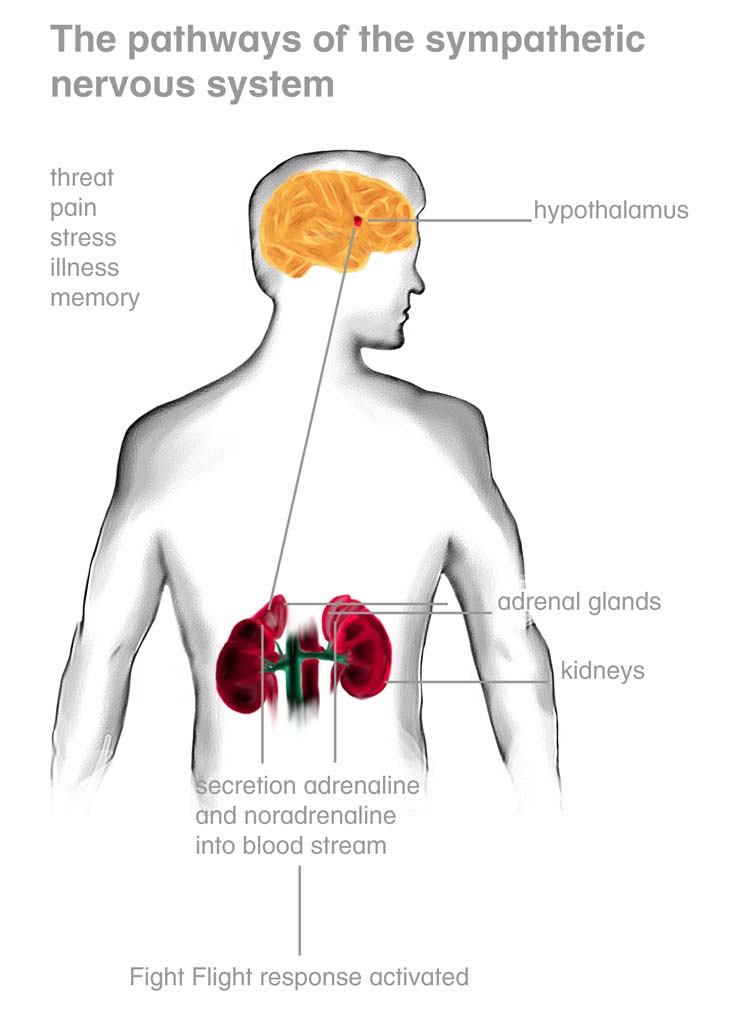
Dr Giresh Kanji Musculoskeletal Pain Specialist Southern Cross Specialist Centre 90 Hanson St, Newtown Wellington New Zealand dr.kanji@xtra.co.nz Ph 9102187 Fax 3895230 Fibromyalgia is a syndrome (collection of symptoms) including widespread pain, poor sleep and fatigue. Fibromyalgia can be accompanied by headaches, migraines, irritable bowel syndrome, anxiety and depression. It is reported that up to 4% of females suffer from fibromyalgia. Fibromyalgia is not a disease (not a specific diagnosis) i.e. unlike pneumonia which is caused by a virus or bacteria it is a term used to define people suffering from a selection of symptoms in which the cause is unknown. The unknown causation also leads to the premise there is no cure. Pain releases stress chemicals adrenaline and cortisol from the adrenal gland that sits above the kidney. The hypothalamus in the brain sends signals to the pituitary gland which then signals the adrenal gland to release adrenaline and cortisol (figure 1). When an animal is in pain endorphins are released by the brain to help control pain. Unfortunately Adrenocorticotrophic hormone (that causes adrenaline and cortisol to be released by the adrenal gland) is part of the same molecule as beta endorphin. They are both part of a larger molecule called propriomelanocortanin (POMC) therefore are released together. The release of stress chemicals (adrenaline and cortisol) is designed to fight the tiger in evolutionary terms. The fight/flight (running or fighting) burns up the stress chemicals returning humans to their
normal state. The release of stress chemicals and endorphins is useful. If wounded in battle then pain is suppressed and the fight/flight response is activated to deal with danger. Figure 1 The hypothalamus and adrenal glands
Unfortunately in modern society pain, emotional stress, insomnia, alcohol and viruses cause the release of adrenaline and cortisol. All of these physiological stresses are not followed by acute vigorous
physical activity (fight/flight) and adrenaline can build up and the brain pathways that receive pain are sensitized by the stress chemicals. The pain spreads into other areas of the body as a result of the sensitized spinal cord and brain pain pathways. Fibromyalgia often occurs after someone has suffered an injury to one part of the body that continues for long periods. The prolonged release of stress chemicals leads to sensitization of the brain that is followed by the pain spreading with time. Accompanying symptoms of insomnia, anxiety, headaches, migraines, depression, fatigue and irritable bowel syndrome develop as they are also caused by stress chemicals.
Effects of adrenaline and cortisol
When the body reacts to signals of threat the sympathetic nervous system creates several changes in the body preparing the body to
fight or take flight (run from danger). If the fight/flight response is activated but not followed by vigorous physical activity adverse effects can occur. The following changes occur in the body with the consequences of not consuming the adrenaline with vigorous physical activity.
• Heart and Lungs The body will require extra blood pumped to the muscles for fight/flight. To increase blood flow to muscles the heart rate speeds up and the force of contraction of the heart increases. Blood pressure increases. The lungs and the bronchial tubes are widened to give increase oxygen availability. Chronic release of stress chemicals can lead to high blood pressure and palpitations. • Abdominal and sexual organs Digestion and reproduction are not important to the fight/flight response and immediate survival from predators. Blood flow is diverted into the muscles and blood flow is reduced to the gut and sexual organs. The stomach and intestine action is suppressed. Erection is inhibited during the fight/flight response. Symptoms such as bloating, abdominal pain, constipation can develop. These are often termed Irritable bowel syndrome. Erectile and sexual dysfunction can also result.
• Cold hands and cold feet The blood flow to the extremities including the hands, feet and scalp are reduced in favour of increased blood supply to the muscles to supply nutrients required for fight/flight. Blood vessels are constricted in the extremities and dilated in the muscles. Cold hands and feet may result as constriction to the skin vessels occurs in the hands and feet. If blood flow to the scalp is chronically restricted by stress chemicals blood flow to follicles reduces leading to hair loss. • Metabolic changes During the fight or flight response from danger nutrients are released from body stores into the blood stream for muscle fuel. Glucose and fats are released into the blood stream ready to provide for the increased physical effort that may be required during the fight/flight response. The release of glucose in the
blood stream can aggravate diabetes. The release of fats, glucose into the blood stream as well as a raised blood pressure can all contribute to the risk of heart disease. This explains the well known risk between stress and development of heart disease.
The above effects of stress chemicals explain many of the symptoms of fibromyalgia including cold hands and cold feet, insomnia, anxiety and irritable bowel syndrome (blood being drawn away from the gut). The production of headaches, migraines and depression are also commonly present as these are also a result of sensitization of pain and other pathways by stress chemicals. Some people also experience fibromyalgia symptoms after a prolonged viral illness due to viral illnesses also releasing stress chemicals. Pain and other symptoms of fibromyalgia are also worse after a poor nights sleep and psychological stress such as bereavements, separation etc. Management of Fibromyalgia The management of chronic widespread pain requires the pain to be reduced to one region. If there is damage to one region of the body then pain will settle back to this region. If the original injury has healed then a patient can be pain free. The depletion of stress chemicals should help reduce the brains sensitivity to pain thus reducing the spread of pain. Heat in the form of a sauna or spa can activate the hypothalamus to begin the sweating process that is designed for cooling the body. The sweating process activates the sympathetic nervous system and helps release cortisol and adrenaline. This is why sweating is often accompanied by a state of relaxation (e.g, sauna and hot yoga) If sleep is affected then using sleeping tablets such as imovane are useful. Sleeping tablets need to be used intermittently (three to four times a week) rather than daily, rather than daily. If these are taken daily then the brain becomes used to the tablets and they can stop working. Addiction can also occur (the body reacts with stress from stopping the tablets) if the tablets are taken on a daily basis. Usually going for one or two nights with poor sleep may be tolerated but several poor nights sleep in a row causes significant fatigue and difficulty coping.
The adrenal gland often suffers after prolonged activation of the fight/flight response. It takes approximately six months of good sleep to restore normal energy to a person suffering from fatigue associated with chronic widespread pain. The muscle tenderness that spreads throughout the body can also be treated at the same time. A wide range of techniques can be used to reduce the muscle pain including acupuncture, massage, stretch techniques and saline injections. The saline injections are to reduce the pain to a source by reducing the muscle pain where the pain has spread to. Other parameters also need to be addressed including poor sleep and exercise can be increased as the person feels able. The final result of treating widespread pain will depend on whether the underlying injury has healed or not. If there is an injury of an underlying structure from a high impact trauma such as car accident or fall then pain may remain at this site. The remaining site of pain often requires investigations to try and find the source and available treatments. Patient examples The below are taken from my notes of real cases. The names have been changed. Case 1 Nicky 12/02/2008: History Nicky initially developed chest pain two years ago which may have been due lifting her two young infants. She has been reviewed by a rheumatologist and diagnosed with chostochondritis. She tried anti- inflammatories, tramadol and diazepam. This gave short term relief and new drugs were tried. She had physiotherapy at the hospital and attended the local hospital pain clinic. The pain spread to her arms, legs and back and she was diagnosed with fibromyalgia. The pain is described as a deep dull constant ache. She had one migraine two weeks ago. She has significant daytime fatigue. Visual analogue score Worst pain 8/10
Best 4/10 Sleep is poor and disturbed frequently. She is taking dothiepan 150mg nocte and imovane nocte to help sleep. She is also taking morphine 30mg mane 20 midday and 10 afternoon. She also has elixir as required. She is also taking gabapentin, panadol four hourly as well anti-inflammatories. She is taking approximately 40 tablets per day for pain control. Past medical history includes thyroid cyst removed, 3 caesarians and tonsillectomy. She has no medical illnesses. Examination There is a good range of motion of the lumbar spine with flexion to touching her toes. There is also a good range of motion of the cervical spine and shoulders. There is tenderness over the intercostal spaces at the posterior rib cage. Management Plan I have referred Nicky to physiotherapy to treat her symptoms as prescribed by myself. I have asked her to reduce her gabapentin by 300mg every three days. 04/03/2008: Nicky has halved her morphine to 30mg per day. She has stopped the dothiepin and also the gabapentin. She has stopped the anti-inflammatories. She is taking two imovane nocte. Sleep is improving. She is not suffering from headaches and migraines. Her chest pain has improved. Her worst pain is at the back of the neck and shoulder regions. Examination Nicky has tenderness over the intercostal muscles over the upper rib cage.
Management Plan I have injected the intercostal spaces that were tender with marcain 0.2ml (B228314 exp05/08) and saline 2ml 0.9% (BG87 exp 01/08). An appointment has been made in two weeks. ---------------------------------------------- 11/03/2008: History Nicky has localised neck pain at the back of the neck. She has noticed her headaches and other symptoms are settling. She is also sleeping better. Examination There is tenderness over the cervical spine suboccipital muscles. Management Plan I have injected the suboccipital muscles with marcain 0.2ml (B228314 exp05/08) and saline 2ml 0.9% (BG87 exp 01/08). An appointment has been made in two weeks. ---------------------------------------------- 25/03/2008: History Nicky is feeling much better. She is able to perform her daily tasks with ease. She is sleeping okay. She is now down to 30mg of morphine, panadol and voltaren. Examination There is some tenderness over the mid back in the intercostal space in two spaces. The tenderness over the suboccipital spaces is much better. Management Plan I have advised her to decrease the panadol and voltaren and only take them as required. The Morphine can also be decreased by 10mg per week. ---------------------------------------------- 03/06/2008:
Phone consult Nicky is sleeping well, has good energy and has no significant pain. She is taking no regular analgesic medications. Her pain is 0/10 on the visual analogue scale over 99% of the time. Comments on case 1 Nicky experienced severe widespread pain, sleep disturbance, fatigue, anxiety and depression. She also attended the sauna three times a week. Her pain resolved completely which shows that the original source of her pain had healed completely but the pain pathways of the brain were sensitized and caused widespread pain. CASE 2 George
19/10/2007: George has had several accidents over the years which have contributed to his ongoing chronic pain. He is currently living in Petone having recently moved from Blenheim. He is currently working for his brother in sheltered employment and has required significant amounts of time off work. The details of his injuries are as follows: Lumbar spine and left hip pain In 1984 George was working as a furniture removal person and after lifting a heavy freezer developed lumbar spine and left hip pain. In 1990 he lifted a 20 litre container into the boot of a car and developed thoracic spine pain. In 2002 he knocked his head on a frame while building a garage and developed neck and left arm pain. After the first two accidents he returned to work despite his pain but after the third accident he was off work for 3 years from 2002 to 2006. In 2006 he was taken off ACC earnings related compensation and was then placed onto an Invalids Benefit. 13 months ago he moved to Petone to work for his brother in sheltered employment.
Current symptoms George has pain in the lumbar spine and left groin pain. This is constant and deep in nature. This pain is aggravated by walking on uneven ground and lifting. Sitting and standing also aggravates the back and left hip pain. He finds walking better for his pain that standing. The pain also radiates into the left leg and into the foot. The leg pain is also constant and described as a deep ache. There are no parasthesiae into the left leg. The thoracic spine pain radiates into the chest region. This is a deep ache and can be sharp when radiating into the front of the chest. There is pain which also radiates into both arms in the past six months. Neckpain, headaches and migraines have been present for the past year. Prior to this time he did not suffer from headaches. He has accompanying nausea, photophobia and vomiting. Migraines are present fortnightly and he goes to sleep. Neck pain is constant and worse on movement. The arm pain is present all the time. When sleeping both arms also develop numbness which he shakes when woken to relieve this symptom. Visual analogue score Worst pain 9/10 Best pain 5/10 George sleeps poorly and has trouble getting to sleep and wakes frequently. He has increased anxiety over the past twelve months. Past medical history includes appendicectomy, depression treated by his General Practitioner. Current medications include Tramadol SR 100 SR tds, Omeprazole 20 mg daily and paracetamol prn. He has an allergy to hibitane and solicaine. He has no allergies to marcain used by the dentist. Examination George has pain on standing on his left leg immediately which improves significantly when he rests on the right leg.
Flexion of the lumbar spine is limited to touching his knees. Sidebending to both directions is limited. He is able to stand on his toes but not on the left heel. There is tenderness over the left sided sacroiliac joint posterior ligament. There is also tenderness over the iliolumbar ligament and the sacrotuberous ligament. There is tenderness over the intercostal muscles of the left side posterior ribs. There is pain on mobilising the left sacroiliac joint. Tinels test over both ulna nerves in the elbows recreates the numbness experienced in both hand little fingers. Impression George has somatic pain in the lumbar spine, cervical spine and thoracic spine region. He has referred pain into the arms as well as the legs. He also has significant headaches and migraines as well. George has several accidents which have caused pain in several regions of the body. The increased spread of pain has resulted due to convergent referred pain which spreads with time and severity of pain. The longer pain is present the more often the pain spreads and the more severe the pain the more it spreads. Management Plan I have advised George of ways to decrease the sympathetic overdrive which occurs with chronic pain. I have also injected the lumbosacral ligaments on the left side as well as the intercostal regions between ribs 1-2 and 10-12 on the left. 08/11/2007: George has noticed a reduction in headaches and migraines. The pain in the lumbar spine region is still present. Standing is worse than walking usually. Examination
Standing on the left leg immediately aggravates pain. Standing on the right leg does not increase pain immediately. The left sacroiliac joint posterior ligament is tender. The left side suboccipital muscle entheses are also tender. The left sided intercostal spaces between 4 and 10 are tender. Management Plan I have injected the posterior sacroiliac joint ligament with marcain 0.2ml (B228314 exp05/08) and saline 2ml 0.9% (BG87 exp 01/08). I have also injected the remaining tender intercostal spaces with marcain 0.2ml (B228314 exp05/08) and saline 2ml 0.9% (BG87 exp 01/08). He has reduced tramadol to 2 tablets SR100 from 3 tablets. I have now prescribed him Tramadol 50 mg so he can titrate himself off tramadol. An appointment has been made in two weeks. ---------------------------------------------- 26/11/2007: George notes his pain is worst on standing on one spot. Walking does progressively aggravate his pain. He is sleeping 5 hours per night. He is still taking tramadol 50mg three to four a day. His nausea has settled. Examination: There is marked pain on translation of the left hip which is worse than the right. There is also pain at the end range of motion of the left hip. Impression George has significant symptoms and signs of left hip pathology which may explain his lumbar spine symptoms. Management Plan
I have ordered an MRI scan of the left hip. It is likely there is an acetabular tear and/or osteochondral lesion. I will review him after the scan. ---------------------------------------------- 13/12/2007: George notes the whole left leg is painful most of the time. The left hip and groin region are the worst affected regions. The MRI scan shows there is a subchondral cyst or perhaps an intra-osseus ganglion present in the left hip. Examination There is marked pain on motion of the left hip in all directions which is not present on the right side. Translation also is painful on the left side. Management Plan I have referred him to a surgeon for a surgical opinion and perhaps arthroscopy of the left hip. Comment on case 2 George obviously damaged the left hip in one of his many traumatic injuries. The pain spread into several parts of his body including severe headaches and migraines. His pain reduced to his left hip region and investigations showed a likely cause of his pain.
a b s t r a c t A Review of the Diagnosis andManagement of Fungal Skin and Nail Infections Dermatophytes are fungi that require D’Arcy Little, MD, CCFP , Lecturer and Academic Fellow, Department of Family and keratin for growth and thus are restrict- Community Medicine, University of Toronto,Toronto, ON. ed to the hair, nails and superficialskin.1 Dermatophytoses are referred to
Sobre a rota de síntese do efavirenz O tema do efavirenz encontra-se na ordem do dia, pois este mês de maio o governo brasileiro adotou decisão inédita de decretar seu licenciamento compulsório atendendo ao interesse público. Afirmou que tem estoques deste fármaco, comprado da Merck Sharp Dohme, até agosto do corrente e que o importará da Índia como genérico enquanto não o
 normal state. The release of stress chemicals and endorphins is useful. If wounded in battle then pain is suppressed and the fight/flight response is activated to deal with danger. Figure 1 The hypothalamus and adrenal glands
Unfortunately in modern society pain, emotional stress, insomnia, alcohol and viruses cause the release of adrenaline and cortisol. All of these physiological stresses are not followed by acute vigorous
normal state. The release of stress chemicals and endorphins is useful. If wounded in battle then pain is suppressed and the fight/flight response is activated to deal with danger. Figure 1 The hypothalamus and adrenal glands
Unfortunately in modern society pain, emotional stress, insomnia, alcohol and viruses cause the release of adrenaline and cortisol. All of these physiological stresses are not followed by acute vigorous
 physical activity (fight/flight) and adrenaline can build up and the brain pathways that receive pain are sensitized by the stress chemicals. The pain spreads into other areas of the body as a result of the sensitized spinal cord and brain pain pathways. Fibromyalgia often occurs after someone has suffered an injury to one part of the body that continues for long periods. The prolonged release of stress chemicals leads to sensitization of the brain that is followed by the pain spreading with time. Accompanying symptoms of insomnia, anxiety, headaches, migraines, depression, fatigue and irritable bowel syndrome develop as they are also caused by stress chemicals.
physical activity (fight/flight) and adrenaline can build up and the brain pathways that receive pain are sensitized by the stress chemicals. The pain spreads into other areas of the body as a result of the sensitized spinal cord and brain pain pathways. Fibromyalgia often occurs after someone has suffered an injury to one part of the body that continues for long periods. The prolonged release of stress chemicals leads to sensitization of the brain that is followed by the pain spreading with time. Accompanying symptoms of insomnia, anxiety, headaches, migraines, depression, fatigue and irritable bowel syndrome develop as they are also caused by stress chemicals.