Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Microsoft word - exercise3 clinical reminders [block].docx
Configuring the EHR Unit 4: Exercise 3: Clinical Reminders Log on CPRS as a doctor1:
1. Double click on the VistA_ Apps folder installed on your desktop.
3. Log on to CPRS Chart using your doctor1 access and doctor1, verify codes.
View Clinical Reminders:
4. Open a patient’s record. (Seven, Patient would be a good choice). Click <OK>.
5. View Clinical Reminders on Cover Sheet. (Remember – by clicking on a specific
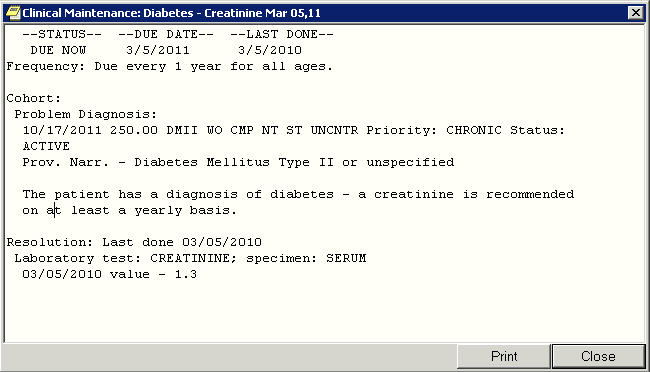
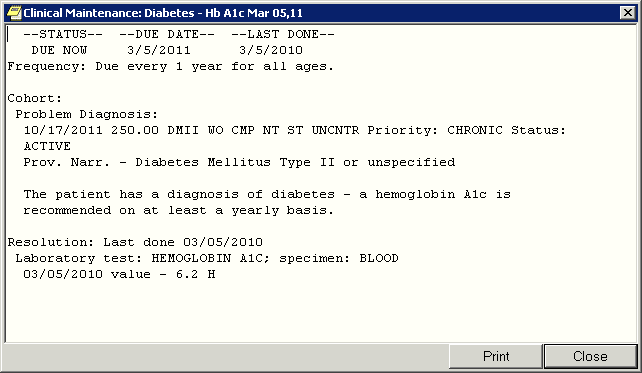
6. Use Print Screen functionality or another functionality to print the Diabetes related
Since the instruction does not say which of the three Diabetes reminders to select, here are all
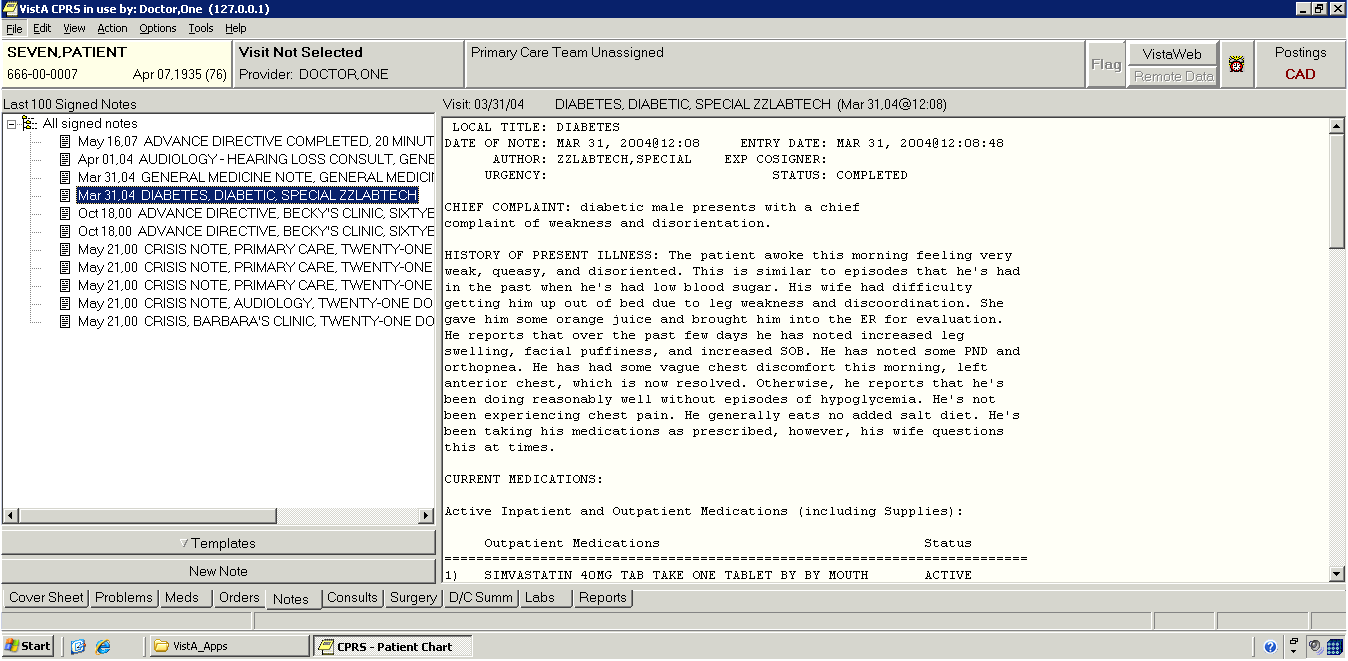
7. View Clinical Reminders on Notes Tab.
8. Select the Diabetes related note by ZZLABTECH.
9. Use Print Screen functionality or another functionality to print information displayed in
the dialog window for Diabetes Urinalysis
Following is the full text of the information provided by VistA. Contrary to what the above instructions say, there is nothing here for Seven,Patient that mentions Urinalysis.
LOCAL TITLE: DIABETES DATE OF NOTE: MAR 31, 2004@12:08 ENTRY DATE: MAR 31, 2004@12:08:48 AUTHOR: ZZLABTECH,SPECIAL EXP COSIGNER: URGENCY: STATUS: COMPLETED CHIEF COMPLAINT: diabetic male presents with a chief complaint of weakness and disorientation. HISTORY OF PRESENT ILLNESS: The patient awoke this morning feeling very
weak, queasy, and disoriented. This is similar to episodes that he's had in the past when he's had low blood sugar. His wife had difficulty getting him up out of bed due to leg weakness and discoordination. She gave him some orange juice and brought him into the ER for evaluation. He reports that over the past few days he has noted increased leg swelling, facial puffiness, and increased SOB. He has noted some PND and orthopnea. He has had some vague chest discomfort this morning, left anterior chest, which is now resolved. Otherwise, he reports that he's been doing reasonably well without episodes of hypoglycemia. He's not been experiencing chest pain. He generally eats no added salt diet. He's been taking his medications as prescribed, however, his wife questions this at times. CURRENT MEDICATIONS: Active Inpatient and Outpatient Medications (including Supplies): Outpatient Medications Status ========================================================================= 1) SIMVASTATIN 40MG TAB TAKE ONE TABLET BY BY MOUTH ACTIVE EVERY EVENING ALLERGIES: Penicillins. SOCIAL HISTORY: The patient lives in Timbuktu with his spouse of many years. He's longtime retired. He does not smoke or use tobacco products. He does not use alcohol. PAST MEDICAL HISTORY: 1) Longstanding type 2 diabetes mellitus with the following complications: nephropathy, severe neuropathy. 2) Recurrent osteomyelitis of the toes with amputations. 3) Coronary artery disease, status post CABG. 4) Chronic atrial fibrillation. 5) Chronic anticoagulation. 6) Hyperlipidemia. 7) Hypertension. 8) Chronic renal insufficiency. 9) Chronic anemia. 10) Diverticulosis. 11) History of congestive heart failure. PAST SURGICAL HISTORY: 1) CABG. 2) Toe amputations as described above. ROS: As reviewed in the HPI. PHYSICAL EXAMINATION: On admission B/P was 139/73, pulse 63, weight 182 lbs. (this was up about 7 pounds since last seen in the clinic two weeks ago). In general the patient appears an ill, weak, elderly appearing male in no acute distress. He is oriented and is able to give a good history. Skin: Somewhat clammy without notable rash. HEENT: Eyes: Sclerae anicteric. Oropharynx with moist mucous membranes. Neck: Supple without palpable mass or adenopathy. Lungs: Diminished throughout, particularly diminished in the bases bilaterally. There is dullness to percussion in both bases. I hear faint basilar rales, not prominent.
Heart: Distant, regular rate and rhythm with a 2 out of 6 systolic murmur heard loudest at the left upper sternal border. S1 is normal. S2 has a fixed split. I do not hear and S3 gallop. PMI is nondisplaced. Abdomen: Nondistended with active bowel sounds. No focal mass or tenderness. No organomegaly. GU/Rectal: Deferred. Extremities: Cool. Feet are somewhat cyanotic. Pedal pulses are diminished and sensation is diminished in a stocking distribution. Neurologic: The patient presently is alert and oriented. Speech is normal. Thought processes are logical. There is no focal motor deficit. EKG appears sinus rhythm with a right bundle branch block. There is some ST abnormality, nonspecific. Chest x-ray: There is cardiomegaly with hilar fullness and cephalization. There appears to be bilateral pleural effusions consistent with heart failure. ASSESSMENT: X: 1. Probable hypoglycemic reaction. 2. Worsening congestive failure. Recent echocardiogram revealed good LV function. There was also pulmonary hypertension. It does appear that there is a component of right heart failure and possibly diastolic dysfunction. 3. Chronic renal insufficiency. The patient has not tolerated ace inhibitors in the past. 4. Coronary artery disease, status post CABG. Cannot exclude component of ischemia. 5. Type 2 diabetes mellitus, longstanding with multiple complications. PLAN: Admit patient to Acute Medical Unit for close observation and further evaluation. Initially decrease Insulin by half and monitor his capillary blood sugars closely. Initiate diuresis with IV Furosemide. Monitor cardiac enzymes and serial EKG's. /es/ )w;X[r[M!Mn8 4)#x:wwU~ Signed: 03/31/2004 12:08 for SPECIAL ZZLABTECH PHYSICIAN
10. (Save print screen in a document to upload to blackboard assignment )
Integrating Theoretical Approaches to Promote Physical Activity Leonard H. Epstein Research on the promotion of physical activity has been based on a variety of conceptualmodels. These models generally target one level of analysis, such as the individual,community, or the environment, and differ in their relative contact with basic or appliedscience. There have been limited attempts to develop
Edwards Angell Palmer & Dodge LLP, Boston, MA Takeda v. Mylan Takeda Counsel EAPD Enlists CaseSight to Fight Off ANDA Claims THE MAT TER Actos Market Under Threat by Generic Drug Makers In 2005 Mylan Inc. sought to launch a generic version of Takeda Chemical Industries’ successful Type 2 diabetes that effectively gave Judge Cote the background and facts drug ACTOS® (pioglitazon
 Configuring the EHR
Configuring the EHR 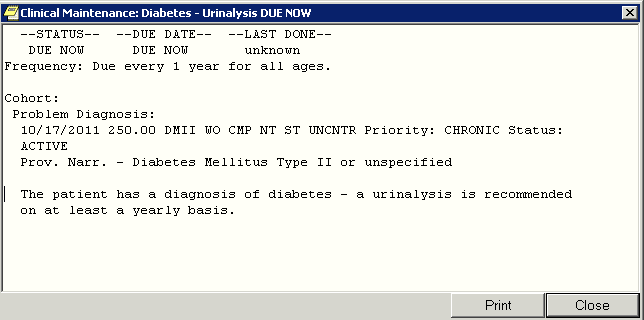
 7. View Clinical Reminders on Notes Tab.
8. Select the Diabetes related note by ZZLABTECH.
9. Use Print Screen functionality or another functionality to print information displayed in
the dialog window for Diabetes Urinalysis
Following is the full text of the information provided by VistA. Contrary to what the above
7. View Clinical Reminders on Notes Tab.
8. Select the Diabetes related note by ZZLABTECH.
9. Use Print Screen functionality or another functionality to print information displayed in
the dialog window for Diabetes Urinalysis
Following is the full text of the information provided by VistA. Contrary to what the above