Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Neurooncology.ucla.edu
P h a s e I I E v a l u a t i o n o f T e m o z o l o m i d e a n d 1 3 - c i s - R e t i n o i c A c i d f o r t h e T r e a t m e n t o f R e c u r r e n t a n d P r o g r e s s i v e M a l i g n a n t G l i o m a : A N o r t h A m e r i c a n B r a i n T u m o r C o n s o r t i u m S t u d y
By Kurt A. Jaeckle, Kenneth R. Hess, W.K. Alfred Yung, Harry Greenberg, Howard Fine, David Schiff, Ian F. Pollack, John Kuhn,
Karen Fink, Minesh Mehta, Timothy Cloughesy, M. Kelly Nicholas, Susan Chang, and Michael Prados
Purpose: Temozolomide (TMZ) and 13-cis-retinoic acid Median overall PFS was 19 weeks (95% CI, 16 to 27 weeks), (cRA) have shown activity in prior single-agent trials of and median overall survival (OS) was 47 weeks (95% CI, 36 recurrent malignant gliomas (MG). This phase II trial evalu- to 58 weeks). OS was 46% (95% CI, 36% to 57%) at 52 ated efficacy and toxicity of combination temozolomide and weeks and 21% (95% CI, 13% to 31%) at 104 weeks. Of 84 cRA treatment in recurrent MG. assessable patients, there were two (3%) complete re- Patients and Methods: Adults with recurrent supratento- sponses and eight (12%) partial responses (complete plus rial MG for whom surgery, radiation, and/or chemotherapy partial response, 15%). Among 499 treatment cycles, the failed were eligible. Treatment included oral TMZ 150 or most common grade 3/4 events included granulocytopenia 200 mg/m2/d, days 1 through 5, and cRA 100 mg/m2/d, (1.8%), thrombocytopenia (1.4%), and hypertriglyceride- days 1 to 21, every 28 days. Primary end point was pro- mia (1.2%). gression-free survival at 6 months (PFS 6); secondary end Conclusion: TMZ and cRA were active, exceeding our points included response, survival, and PFS12. 20% thresholds for PFS 6 success, assuming 20% improve- Results: Eighty-eight eligible patients (glioblastoma mul- ment over our previously reported database (glioblastoma tiforme [n ؍ 40]; anaplastic gliomas [n ؍ 48; astrocytoma, multiforme: expected, 30%; observed, 32%; anaplastic gli- 28; oligodendroglioma, 14; mixed glioma, six]) received oma: expected, 40%; observed, 50%). treatment. PFS 6 was 43% (95% confidence interval [CI], J Clin Oncol 21:2305-2311. 2003 by American 33% to 54%) and PFS12 was 16% (95% CI, 10% to 26%). Society of Clinical Oncology.
DESPITE OPTIMAL treatment for malignant gliomas, re-
currence is common within the first 2 years. This poor
The study was performed by the NABTC, a National Cancer Institute
outcome was underscored by a recent analysis of eight consec-
(NCI) consortium of 11 participating institutions (Dana-Farber Cancer
utive phase II trials of 375 patients with recurrent glioma treated
Institute, University of California at San Francisco, University of Michigan
with various chemotherapeutic regimens.1 This analysis revealed
Hospital, University of Pittsburgh, Children’s Hospital of Pittsburgh, Uni-versity of Texas Health Sciences Center at San Antonio, University of Texas
a 6-month progression-free survival rate (PFS 6) of only 15% for
M.D. Anderson Cancer Center, University of Texas Southwestern, Univer-
patients with glioblastoma multiforme (GM) and 31% for pa-
sity of Wisconsin, University of California at Los Angeles, and University of
tients with anaplastic glioma (AG). After recurrence, response to
Chicago). The study was activated December 17, 1998 at the University of
treatment was observed in only 9% of patients, and overall
Texas M.D. Anderson Cancer Center, was expanded to the NABTC on April
median survival was only 30 weeks. In meta-analysis studies,
9, 1999, and was closed to accrual on January 30, 2000. All data werecollected and analyzed at the NABTC Data Management Center at the
there seems to be modest evidence of a survival benefit whenchemotherapy is added to standard surgical and radiation ther-apy, particularly in selected subsets of newly diagnosed gliomapatients.2,3 However, there is little evidence of benefit of
From the University of Texas M.D. Anderson Cancer Center, Houston;
chemotherapy after tumor recurrence or progression, and newer
University of Texas Health Science Center, San Antonio; and University of
agents and regimens need evaluation. Texas Southwestern Medical Center, Dallas, TX; University of Michigan,Ann Arbor, MI; Dana-Farber Cancer Institute, Boston, MA; University of
There is preclinical and clinical evidence of activity of
Pittsburgh and Children’s Hospital of Pittsburgh, Pittsburgh, PA; University
retinoids and/or alkylators in gliomas, either as single agents or
of Wisconsin, Madison, WI; University of California at Los Angeles, Los
in combination. Two such orally administered agents with
Angeles; University of California at San Francisco, San Francisco, CA;
different modes of action, temozolomide (TMZ) and 13-cis-
University of Chicago, Chicago, IL.
retinoic acid (cRA), have shown activity in recurrent malignant
Submitted December 17, 2002; accepted March 26, 2003. This research protocol was supported grants CA62399, CA62422,
gliomas without overlapping toxicity in phase II clinical trials.4-6
CA62412, CA16672, CA62455, CA62426, UO1CA62407-08, UO1CA62405,
Multiagent combination regimens containing both retinoids and
alkylating agents have been active in malignancies of several
RR00056, MO1-RR0865, MO1-RR00042, and MO1-RR03186 from the
histologic subtypes.7-10 On the basis of these observations, the
National Institutes of Health, Bethesda, MD.
North American Brain Tumor Consortium (NABTC) chose to
Address reprint requests to Kurt A. Jaeckle, MD, Department of Oncologyand Neurology, Mayo Clinic Jacksonville, 4500 San Pablo Blvd, Jackson-
perform a prospective, phase II, single-arm trial (NABTC
ville, FL 32224; email: jaeckle.kurt@mayo.edu.
98 – 03) of TMZ and cRA in patients with recurrent and
2003 by American Society of Clinical Oncology.Journal of Clinical Oncology, Vol 21, No 12 (June 15), 2003: pp 2305-2311
Information downloaded from www.jco.org and provided by UCLA on April 25, 2006 from 149.142.103.13.
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
University of Texas M.D. Anderson Cancer Center. Approval of the protocol
received prior chemotherapy (150 mg/m2/d for those who had received prior
and informed consent by local human investigation committees was obtained
chemotherapy) days 1 through 5 every 28 days. cRA (Isotretinoin; Roche
from each institution, in accord with assurance filed with and approved by the
Laboratories, Nutley, NJ) was administered at 100 mg/m2/d to all patients
United States Department of Health and Human Services where appropriate.
regardless of prior treatment, in two divided doses, 12 hours apart on days 1
Informed consent was obtained from each subject or subject’s guardian.
through 21 every 28 days. A course was defined as a 28-day period oftreatment. Treatment courses were repeated every 28 days from day 1,
provided that all hematologic toxicity from the previous course had resolved
The two primary objectives of this study included determination of
to grade 2 or less, and all nonhematologic toxicity had recovered to either
efficacy and toxicity of the combination of TMZ and cRA in the treatment of
grade 0 or 1. If recovery had not occurred by day 28, the subsequent course
patients with recurrent and progressive GM or AG. The primary end point
of TMZ and cRA was delayed until these criteria were met.
was progression-free survival at 6 months (PFS 6). Secondary end points
No dose escalations were allowed. Dose reduction for toxicity was
included overall survival, time to progression, and, for assessable patients,
allowed in 25-mg reduction increments, for both TMZ and cRA. Only two
response. Toxicity was evaluated in all eligible patients receiving at least one
dose reductions were permitted, and patients having grade 3 toxicity of any
type after two dose reductions were removed from study. Patients werepretreated with oral antiemetics before each TMZ dose and as needed
symptomatically. Patients were required to maintain the lowest corticosteroid
Eligibility required a prior histologic diagnosis of supratentorial GM or
dose necessary for neurologic stability.
AG, which was defined as anaplastic astrocytoma (AA), anaplastic oligo-dendroglioma, or anaplastic malignant glioma (AMG). The pathologic tissue
diagnosis made at the treating institution was accepted; however, thepathology reports on all patients were centrally reviewed to verify the tumor
Patients were evaluated for response using a combination of both clinical
histology. Unequivocal evidence of recurrence or progression by neuroim-
(neurologic examination) and neuroimaging (enhanced MRI or CT) proce-
aging procedure (computed tomography [CT] or magnetic resonance imag-
dures before every other course (eg, 3, 5, 7, and so on) as compared with
ing [MRI]) was required, with the progression observed after surgery and
baseline. Neurologic performance was assessed by the grading of symptoms
radiation and Յ two prior chemotherapy regimens, either as adjuvant
and signs that were considered to be not related to a postictal state or other
treatment or at recurrence. Patients more than 4 weeks from complete
non–tumor-related process, as compared with the last examination. Patients
resection were required to have evidence of measurably enhancing disease on
were graded as either definitely better (ϩ2), possibly better (ϩ1), unchanged
MRI or CT within 14 days of registration. Those with recent (Յ 4 weeks)
(0), possibly worse (Ϫ1), or definitely worse (Ϫ2).
complete resection were eligible without enhancing disease but were not
Response was assessed using a modification of the MacDonald criteria.11
assessable for response. Patients were required to be older than 18 years;
All final response determinations required that patients had a stable or
have a life expectancy greater than 8 weeks; have a Karnofsky performance
improved clinical examination as compared with baseline and were on stable
status greater than 60; be recovered from toxic effects of prior radiotherapy
or decreased doses of corticosteroids as compared with the prior evaluation.
or other therapies; and be at least 2 weeks from vincristine, 6 weeks from
Responses (complete response [CR] or partial response [PR]) were required
nitrosoureas, and 3 weeks from other chemotherapy. Other eligibility factors
to be sustained on two successive scans taken 8 weeks apart to be considered
included absolute neutrophil counts of greater than 1,500/mL, platelets Ն
valid. Independent central review was performed on all patients considered
100,000/mL, transaminases and alkaline phosphatase less than two times the
to be responding by the local investigators, and if the central reviewer was in
institutional upper limits of normal, bilirubin less than 1.5 mg %, blood ureanitrogen and creatinine less than 1.5 times the upper limit of institutional
agreement, response was designated as confirmed. If all relevant scans
normal, negative beta-human chorionic gonadotropin at registration, use of
were not all available at the time of central review, the response was
effective birth control, and provision of informed, written consent.
Patients were ineligible if they had active infection, were pregnant or
Progression-free survival (PFS) and overall survival (OS) were defined as
breast feeding, or had history of a prior cancer (unless off therapy and in
the time from the first day of treatment until progression or death. Patients
complete remission for Ͼ 3 years), excepting nonmelanotic skin cancer and
were removed from study if there was progressive disease, development of
unacceptable toxicity, an unacceptable status quo or patient refusal, ornoncompliance with protocol requirements.
Toxicity monitoring was performed on patients, on all cycles. Safety
parameters included all laboratory and hematologic abnormalities, neuro-logic historical and examination findings, and adverse events reported by
The primary objective was to determine whether TMZ and cRA could
patients. The NCI common toxicity criteria version 2.0 was used for adverse
significantly delay progression in patients with recurrent GM and AG.
event and toxicity reporting. Data forms were submitted to the central
Historical values were obtained from analysis of a database of 375 patients
NABTC office according to protocol guidelines and entered in the Protocol
with recurrent high-grade glioma (225 GM and 150 AA) treated on eight
Data Management System. The study was monitored by the Clinical Data
consecutive prospective phase II trials,1 in which PFS 6 was 21% (GM, 15%;
Update System Version 1.1, with cumulative Clinical Data Update System
AA, 31%). The hypotheses tested are H0: p ϭ p0 versus H1: p more than p1,
data submitted quarterly to the Cancer Treatment and Evaluation Program.
where p was the probability of remaining alive and progression-free at 6
Serious adverse events (AEs) or adverse drug reactions (ADRs) were
months, with an alpha of 10% and beta of 5%. For GM, p0 was set at 10%
reported using the NCI/Division of Cancer Treatment ADR reporting form.
and p1 at 30%, looking for improvement of 0.2. For AG, p0 was set at 20%
The process followed the NABTC and United States Food and Drug
and p1 at 40%, looking for an improvement of 0.2. A prior phase II study of
Administration guidelines for reporting of ADRs.
TMZ in 116 recurrent AGs showed a PFS 6 of 22%.5 The current study was
Quality assurance measures included ongoing (per protocol timetable)
designed to accrue 45 GM and 40 AG patients. For GM, success was defined
monitoring of protocol compliance and submitted case report forms, on-site
as observing more than seven of 40 patients alive and progression-free at 6
months (yielding alpha ϭ 4% and beta ϭ 6%). For AG, declaring success if13 of 45 reached 6 months progression-free would yield an alpha of 5% and
beta of 8%. Kaplan-Meier estimates for PFS and OS and exact binomial
TMZ (Schering Plough Pharmaceuticals, Kenilworth, NJ) was adminis-
confidence intervals (CIs) were computed using S-plus 2000 (MathSoft, Inc,
tered orally at a starting dose of 200 mg/m2/d for patients who had not
Information downloaded from www.jco.org and provided by UCLA on April 25, 2006 from 149.142.103.13.
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
TMZ AND CRA FOR RECURRENT MALIGNANT GLIOMA
Table 1. Temozolomide and cis-Retinoic Acid in Recurrent Malignant Table 2. Temozolomide and cis-Retinoic Acid in Recurrent Malignant Gliomas: Clinical Characteristics Gliomas: Response
Abbreviations: CR, complete response; PR, partial response.
or more surgeries. Almost 90% of patients had a prior partial
resection or gross total resection; 13% had received biopsy only.
The surgical procedures performed most proximate to registra-
tion were generally biopsy or partial resection. All 88 patients
had experienced treatment failure with prior radiotherapy. Most
patients (69 [78%] of 88 patients) had experienced treatment
failure with one to two prior chemotherapy regimens, but 19
patients (22%) were chemotherapy-naive. All 88 patients were
assessable for toxicity, and 84 were assessable for response (four
patients were not assessable for response because of gross total
resections without measurably enhancing disease at registration).
Of the 84 patients assessable for response (Table 2), there
were two CRs (3%) and nine PRs (12%), for an overall response
rate (ORR; CR ϩ PR) of 15%. By histologic diagnosis, re-
sponses occurred as follows: CR, AA (n ϭ 1), AO (n ϭ 1); PR,
GM (n ϭ 2), AA, (n ϭ 2), AMG (n ϭ 3), AO (n ϭ 2).
Radiographic responses were confirmed by independent central
review in all patients except one, an unconfirmed PR patient in
whom the appropriate scans were unavailable at the time of
central review. On review, all responding patients were on stable
(four of 11) or no corticosteroids (seven of 11) at the time of the
Abbreviations: GM, glioblastoma multiforme; AA, anaplastic astrocy-
toma; AO, anaplastic oligodendroglioma; AMG, anaplastic malignantglioma.
There were 88 eligible patients with recurrent supratentorial
malignant gliomas (GM, n ϭ 40; AG, n ϭ 48) analyzed by intent
to treat (Table 3; Figs 1 and 2). Thirty-eight patients (43%; 95%
Eighty-nine patients with recurrent, progressive malignant
CI, 33% to 54%) were alive and progression-free at 6 months
gliomas were registered. Eighty-eight were eligible; one patient
(PFS 6). The overall PFS 12 was 16% (95% CI, 10% to 26%).
without demonstrable radiographic progression at registration
Median overall PFS was 19 weeks (95% CI, 16 to 27), and
was found to be ineligible. Of the 88 eligible, assessable patients,
median OS was 47 weeks (95% CI, 36 to 58). OS was 46% (95%
there were 40 patients with GM (one had gliosarcoma) and 48
CI, 36% to 57%) at 52 weeks and 20% (95% CI, 13% to 31%)
patients with AG (28 patients with AA, 13 patients with
anaplastic oligodendroglioma [AO], one with oligodendrogli-
Analysis by histologic strata was also performed. In the 40
patients with GM, PFS 6 was 32% (95% CI, 21% to 51%) PFS 12
The clinical and demographic features of the 88 patients are
was 15% (95% CI, 7% to 31%), and median PFS was 16 weeks
listed in Table 1. The median age of the patients was 45 years
(95% CI, 9 to 26 weeks). The OS 6 for GM was 65% (95% CI, 52%
(range, 23 to 70 years). There was a three to two male-to-female
to 82%), and median OS was 35 weeks (95% CI, 28 to 79 weeks).
ratio. Median Karnofsky performance status (KPS) was 80, with
In the 48 patients with AG (non-GM), the PFS 6 was 50% (95% CI,
a minimum of 60. All patients had been unsuccessfully treated
38% to 66%), PFS 12 was 17% (95% CI, 9% to 31%), and median
with prior surgery; 41% had one prior surgery and 59% had two
PFS was 25 weeks (95% CI, 16 to 32 weeks). The OS 6 for all
Information downloaded from www.jco.org and provided by UCLA on April 25, 2006 from 149.142.103.13.
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
Table 3. Temozolomide and cis-Retinoic Acid in Recurrent Malignant Gliomas: Survival
Abbreviations: PFS 6, progression-free survival at 6 months; OS 6, overall survival at 6 months; PFS 12, progression-free survival at 12 months; TMZ, temozolomide; cRA,
cis-Retinoic Acid; GM, glioblastoma multiforme; AA, anaplastic astrocytoma; AG, anaplastic glioma; AMG, anaplastic mixed glioma; AO, anaplastic oligodendroglioma;NS, not stated; NR, not yet reached.
*Included 28 AA and seven AMG patients. †Intent-to-treat population.
patients with AG was 83% (95% CI, 73% to 95%), and median OS
(10%) completed at least 12 cycles (approximately 1 year of
was 52 weeks (95% CI, 38 to 60 weeks). For the subsets of AG, end
therapy), but only three (3.4%) of patients received Ն 24 cycles
point parameters for the AO and non-AO AG subsets are provided
(approximately 2 years of therapy). Five patients (6%) who did
in more detail in Table 3. Regarding the primary end point of the
not experience disease progression refused further therapy after
study (PFS 6), the results exceeded our 20% thresholds for success,
at least one dose, and two additional patients were noncompliant
assuming a 20% improvement as compared with our previously
during therapy; these were included in the analysis. Sixty-six
reported database1 (GM: expected, 30%; observed, 32%; AG:
patients went off study as a result of progressive disease after
one or more courses, and five additional patients died beforedocumented radiographic progression. Treatment Intensity and Reasons for Removal From Study
The average number of 28 day cycles received was 5.7.
Seventy-four patients (84%) received at least one cycle, and 70
Toxicity was recorded for all grades for all eligible patients
patients (79%) completed at least two cycles. Nine patients
by type, using the NCI common toxicity criteria (version 2.0). Fig 1. Overall survival by histologic subtype (Kaplan-Meier curve). GBM, glio- blastoma multiforme; AO, anaplastic oligo- dendroglioma; Oth, other.
Information downloaded from www.jco.org and provided by UCLA on April 25, 2006 from 149.142.103.13.
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
TMZ AND CRA FOR RECURRENT MALIGNANT GLIOMA
Fig 2. Progression-free survival by his- tologic subtype (Kaplan-Meier curve). GBM, glioblastoma multiforme; AO, anaplastic ol- igodendroglioma; Oth, other.
Table 4 lists all grade 1 to 5 toxicity observed, with each figure
alone, with the exception of elevated triglycerides, which was
representing the sum of the highest grade of toxicity attained, per
considered to be secondary to the cRA.
toxicity, per course for all patients. In the total of 499 treatment
courses, we observed 505 grade 1 to 4 AEs; there were no grade5 AEs. There were 35 (7%) grade 3 AEs, and 17 (3%) grade 4
The prognosis of patients with recurrent malignant astrocytoma
AEs. The most common grade 3 to 4 AEs were granulocytopenia
remains poor. Wong et al1 published an analysis of clinical
(1.8%), thrombocytopenia (1.4%), and hypertriglyceridemia
outcomes in 375 patients with recurrent malignant glioma (GM,
(1.2%). Grade 3 elevation in ALT was observed in 5.7%. No
225; AG, 150) who received chemotherapy in eight consecutive
patient went off study because of toxicity, and no deaths were
prospective phase II trials. The overall 6-month PFS rate was only
attributed to the drug regimen. No observable additive toxicity
31% and 15% for patients with recurrent AA and GBM, respec-
was observed with the combination as compared with TMZ
tively. Because of these dismal results, there has been heightenedinterest in the investigation of new agents and combinations.
TMZ is an orally bioavailable imidazotetrazine derivative of
Table 4. Temozolomide and cis-Retinoic Acid in Recurrent Malignant
dacarbazine. TMZ undergoes chemical degradation to its active
Gliomas: Toxicity
metabolite, monomethyl triazenoimidazole carboxamide, at
physiologic pH.12-14 Evidence to date suggests that cytotoxicity
of monomethyl triazenoimidazole carboxamide is primarily due
to methylation at the O6 position of guanine.12-14 TMZ addition-
ally acts as an inhibitor of DNA mismatch repair and can induce
apoptosis.15 Additive or synergistic effects on growth inhibition
have been reported in preclinical models, including cell lines and
human glioma xenograft models.16-20 Concentrations of TMZ in
the CNS reach approximately 30% of plasma concentrations
after systemic administration.21 TMZ has also shown evidence
of activity in clinical trials of human malignant gliomas. Yung et
al5 reported a CR ϩ PR rate of 35%, a PFS 6 of 46%, and overall
survival of 13.6 months in a phase II trial of TMZ in patients
with recurrent AA. Another randomized study of 116 recurrent
malignant glioma patients compared single-agent TMZ with
procarbazine.4 In that study, PFS 6 of 21% was observed with
TMZ, versus 8% with procarbazine (P ϭ .008). Noncumulative
myelosuppression, in the form of thrombocytopenia and neutro-
penia, was the dose-limiting toxicity in clinical studies.4,9
Information downloaded from www.jco.org and provided by UCLA on April 25, 2006 from 149.142.103.13.
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
Subsequently, TMZ was conditionally approved by the United
mg/m2/d for 3 weeks, followed by 1 week of rest every 28 days.
States Food and Drug Administration for the indication of
A response rate of 23% (PR, 7%; minor response, 16%) was
observed, with median time to progression of 16 weeks and
Synthetic retinoids induce apoptosis and differentiation while
median survival of 58 weeks for GM and 34 weeks for AA.
inhibiting cell proliferation.22 Inhibition of migration and prolif-
Clinical trials of combination chemotherapy with retinoids
eration has been observed after retinoic acid treatment in primary
and alkylating agents have shown activity in recurrent squamous
glioma cultures but to a lesser degree in established glioma
cell carcinoma of the head and neck, non–small-cell lung
lines.23 Inhibition of proliferation and induction of apoptosis in
carcinoma, pancreatic cancer, and childhood and acute promy-
human glioma cell lines may be concentration dependent and
elocytic leukemia.7-10 It was our hypothesis that the combination
involve signal transduction transcription factors.24 Trans-
of TMZ and cRA would have therapeutic potential in glioma,
retinoic acid has been shown to downregulate leukemia inhibi-
based on observations of preclinical and clinical activity with
tory factor and telomerase activity, resulting in inhibition of
each agent, different mechanisms of action, and predominantly
tumor growth and producing differentiation effects in medullo-
blastoma cells.25 Retinoic acid also inhibits tenascin-C expres-
The current study was a modestly sized (N ϭ 88) single-arm
sion in C6 glioma cell lines.26 cRA modulates nuclear retinoic
prospective trial, with separate stratification for GM and AG.
acid receptor and the alpha and beta retinoid x-receptors in
The patient accrual numbers were derived from a hypothesis that
glioma cell lines.27 Binding of retinoids to the nuclear retinoic
a 20% improvement in PFS 6 would be observed with the
acid receptor and retinoid x-receptor produces a downstream
combination of TMZ and cRA for both strata, based on data from
decrease in hepatocyte growth factor expression, interrupting a
the historical database.1 In our study, for all patients, the PFS 6
potential autocrine proliferative loop; hepatocyte growth factor
was 43%. PFS 6 was 32% for GM and 50% for all AG combined
and the related c-Met receptor is present in high levels in human
(46% for the non-AO AG subset and 61% for pure AO subset).
gliomas.28 Antitumor activity of retinoic acid has been observed
These results, as compared with the PFS 6 observed in the database
in the GL-15 glioblastoma29 and the U343 malignant glioma cell
(GM, 15%; AG, 31%), met the criteria for PFS 6 success, exceeding
lines.30 Pharmacokinetic studies have shown that adequate concen-
the 20% improvement for both the GM and AG strata. At the time
trations of cRA can be reached in rodent CNS after systemic
of design of the current protocol, the PFS 6 for TMZ alone was not
administration, but with a relatively short terminal half-life in rat
yet reported; subsequent clinical trials of single-agent TMZ reported
brain tissue (0.57 to 1.02 hours).31 These data support a schedule of
frequent or continuous oral dosing of cRA in human clinical trials.
An interesting aspect of this study involved the group of
A prior phase II trial (Radiation Therapy Oncology Group
patients with pure AO. In this group, the PFS 6 was 62%, and OS
91–13) of all-trans-retinoic acid in 30 patients with recurrent
was 55 weeks. A prior study of TMZ in treatment of 30 patients
malignant glioma disclosed minor activity, with tolerable side
with recurrent AO showed a response rate of 30%.35 Although
effects; a response rate of 12% was observed, with a median time
specific survival end points were not reported, 13 (44%) of the
to progression of 3.8 months and a median OS of 5.7 months.32
AO patients were progression-free at 6 months. Although direct
A similar single-institution phase II trial of all-trans-retinoic acid
comparisons are not possible, the greater survival noted with the
in 36 patients with recurrent glioma did not show much evidence
TMZ/cRA combination in this trial deserves further study. In
of activity, with a 3% minor response rate, and median time to
addition, survival of the recurrent AO cohort was much longer
progression of only 8 weeks.33 A recent phase II trial of the
than the GM and non-AO AG cohorts, raising the question of
combination of radiotherapy and cRA plus interferon alfa-2a in
whether the AO patients should be stratified separately.
patients with newly diagnosed high-grade glioma did not show
Caution is advised with regard to statistical comparisons of
an improvement in survival as compared with historical con-
these uncontrolled results with the historical database1 or prior
trols.34 Yung et al6 conducted a phase II prospective study of 43
TMZ trials.4,5 Nevertheless, the results from the current phase II
patients with recurrent malignant glioma treated with cRA as a
trial suggest that the combination of TMZ and cRA may be a
single agent, administered at a daily oral dose of 60 to 100
more active regimen in recurrent malignant gliomas.
1. Wong ET, Hess KR, Gleason MJ, et al: Outcomes and prognostic
5. Yung WK, Prados MD, Yaya-Tur R, et al: Multicenter phase II trial of
factors in recurrent glioma patients enrolled onto phase II clinical trials.
temozolomide in patients with anaplastic astrocytoma or anaplastic oligoas-
trocytoma at first relapse: Temodal Brain Tumor Group. J Clin Oncol
2. Fine HA, Dear KB, Loeffler JS, et al: Meta-analysis of radiation
therapy with and without adjuvant chemotherapy for malignant gliomas in
6. Yung WK, Kyritsis AP, Gleason MJ, et al: Treatment of recurrent
malignant gliomas with high-dose 13-cis-retinoic acid. Clin Cancer Res
3. Stewart LA: Chemotherapy in adult high-grade glioma: A systematic
review and meta-analysis of individual patient data from 12 randomized
7. Recchia F, Lalli A, Lombardo M, et al: Ifosfamide, cisplatin, and 13 -cis
retinoic acid for patients with advanced or recurrent squamous cell carcinoma of
4. Yung WK, Albright RE, Olson J, et al: A phase II study of temozolo-
the head and neck: A phase I-II study. Cancer 92:814-821, 2001
mide vs. procarbazine in patients with glioblastoma multiforme at first
8. Recchia F, Sica G, De Fillippis S, et al: Cisplatin, vindesine,
mitomycin-C, and 13-cis retinoic acid in the treatment of advanced
Information downloaded from www.jco.org and provided by UCLA on April 25, 2006 from 149.142.103.13.
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
TMZ AND CRA FOR RECURRENT MALIGNANT GLIOMA
non-small cell lung cancer: A phase II pilot study. Anticancer Res
22. Costa SL, Paillaud E, Fages C, et al: Effects of a novel synthetic
retinoid on malignant glioma in vitro: Inhibition of cell proliferation,
9. Recchia F, Sica G, Casucci D, et al: Advanced carcinoma of the
induction of apoptosis and differentiation. Eur J Cancer 37:520-550, 2001
pancreas: Phase II study of combined chemotherapy, beta-interferon, and
23. Bouterfa H, Picht T, Kess D, et al: Retinoids inhibit human glioma
retinoids. Am J Clin Oncol 21:275-278, 1998
cell proliferation and migration in primary cell cultures but not in established
10. Hirota T, Fujimoto T, Katano N, et al: Treatment results of intermit-
cell lines. Neurosurgery 46:419-440, 2000
tent and cyclic regimen with ATRA and chemotherapy in childhood acute
24. Paillaud E, Costa S, Fages C, et al: Retinoic acid increases prolifer-
promyelocytic leukemia: Children’s Cancer and Leukemia Study Group.
ation rate of GL-15 glioma cells, involving activation of STAT-3 transcrip-
tion factor. J Neurosci Res 67:670-679, 2002
11. MacDonald DR, Cascino TL, Schold SC, et al: Response criteria for
25. Liu J, Guo L, Luo Y, et al: All trans-retinoic acid suppresses in vitro
phase II studies of supratentorial malignant glioma. J Clin Oncol 8:1277-
growth and down-regulates LIF gene expression as well as telomerase
activity of human medulloblastoma cells. Anticancer Res 20:2659-2664,
12. Stevens MF, Hickman JA, Langdon SP, et al: Antitumor activity and
pharmacokinetics in mice of 8-carbamoyl-3-methyl-imidazo[5, 1-d]-1, 2, 3,
26. Alvarez-Dolado M, Gonzalez-Sancho JM, Navarro-Yubero C, et al:
5-tetrazin-4(3H)-one (CCRG 81045; M & B 39831), a novel drug with
Retinoic acid and 1, 25-dihydroxyvitamin D3 inhibit tenascin-C expression
potential as an alternative to dacarbazine. Cancer Res 47:5846-5852, 1987
in rat glioma C6 cells. J Neurosci Res 58:293-300, 1999
13. Clark AS, Stevens MF, Sansom CE, et al: Anti-tumour imidazotet-
27. Carpentier AF, Leonard N, Lacombe J, et al: Retinoic acid modulates
razines: Part XXI. Mitozolomide and temozolomide—Probes for the major
RAR alpha and RAR beta receptors in human glioma cell lines. Anticancer
groove of DNA. Anticancer Drug Des 5:63-68, 1990
14. Tsang LL, Farmer PB, Gescher A, et al: Characterisation of urinary
28. Chattopadhyay N, Butters RR, Brown EM: Agonists of the retinoic
metabolites of temozolomide in humans and mice and evaluation of their
acid- and retinoid X-receptors inhibit hepatocyte growth factor secretion and
cytotoxicity. Cancer Chemother Pharmacol 26:429-436, 1990
expression in U87 human astrocytoma cells. Brain Res Mol Brain Res
15. D’Atri S, Tentori L, Lacal PM, et al: Involvement of the mismatch
repair system in temozolomide-induced apoptosis. Mol Pharmacol 54:334-
29. Chambaut-Guerin AM, Costa SL, Lefrancois T, et al: Effects of
retinoic acid and tumor necrosis factor alpha on GL-15 glioblastoma cells.
16. Kokkinakis DM, Hoffman RM, Frenkel EP, et al: Synergy between
methionine stress and chemotherapy in the treatment of brain tumor
30. Dirks PB, Patel K, Hubbard SL, et al: Retinoic acid and the cyclin
xenografts in athymic mice. Cancer Res 61:4017-4023, 2001
dependent kinase inhibitors synergistically alter proliferation and morphol-
17. Kokkinakis DM, Bocangel DB, Schold SC, et al: Thresholds of
O6-alkylguanine-DNA alkyltransferase which confer significant resistance
ogy of U343 astrocytoma cells. Oncogene 15:2037-2048, 1997
of human glial tumor xenografts to treatment with 1, 3-bis (2-chloroethyl)-
31. Le Doze F, Debruyne D, Albessard F, et al: Pharmacokinetics of
1-nitrosourea or temozolomide. Clin Cancer Res 7:421-428, 2001
all-trans retinoic acid, 13-cis retinoic acid, and fenretinide in plasma and
18. Sankar A, Thomas DG, Darling JL: Sensitivity of short-term cultures
brain of Rat. Drug Metab Dispos 28:205-208, 2000
derived from human malignant glioma to the anti-cancer drug temozolomide.
32. Phuphanich S, Scott C, Fischbach AJ, et al: All-trans-retinoic acid: A
phase II Radiation Therapy Oncology Group study (RTOG 91-13) in patients
19. Bobola MS, Tseng SH, Blank A, et al: Role of O6-methylguanine-
with recurrent malignant astrocytoma. J Neurooncol 34:193-200, 1997
DNA methyltransferase in resistance of human brain tumor cell lines to the
33. Kaba SE, Kyritsis AP, Conrad C, et al: The treatment of recurrent
clinically relevant methylating agents temozolomide and streptozotocin. Clin
cerebral gliomas with all-trans-retinoic acid (tretinoin). J Neurooncol 34:
20. Friedman HS, Dolan ME, Pegg AE, et al: Activity of temozolomide
34. Dillman RO, Shea WM, Tai DF, et al: Interferon-alpha2a and
in the treatment of central nervous system tumor xenografts. Cancer Res
13-cis-retinoic acid with radiation treatment for high-grade glioma. Neuro-
21. Stupp R, Ostermann S, Leyvraz S, et al: Cerebrospinal fluid levels of
35. Van den Bent MJ, Keime-Guiebert F, Brandes AA, et al: Temozolo-
temozolomide as a surrogate marker for brain penetration. Proc Am Soc Clin
mide chemotherapy in recurrent oligodendroglioma. Neurology 57:340-342,
Information downloaded from www.jco.org and provided by UCLA on April 25, 2006 from 149.142.103.13.
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
Appendix 2 - Commissioning Best Value Programme Cash releasing schemes Comments There are two elements to the Falls Programme; a new community falls pathway and NWAS deflections. The primary care falls pathway to pilot in two practices. This has been delayed as one of the practices originally identified has withdrawn from the process. A replacement practice has been identified but is likely
HAMLINE JOURNAL OF PUBLIC LAW & POLICY [Vol. MEDIATION: ITS ORIGIN & GROWTH IN INDIA I. BACKGROUND Mediation is not something new to India. Centuries before the British arrived, India had utilized a system called the Panchayat system, whereby respected village elders assisted in resolving community disputes. Such traditional mediation continues to be utilized even today in vil
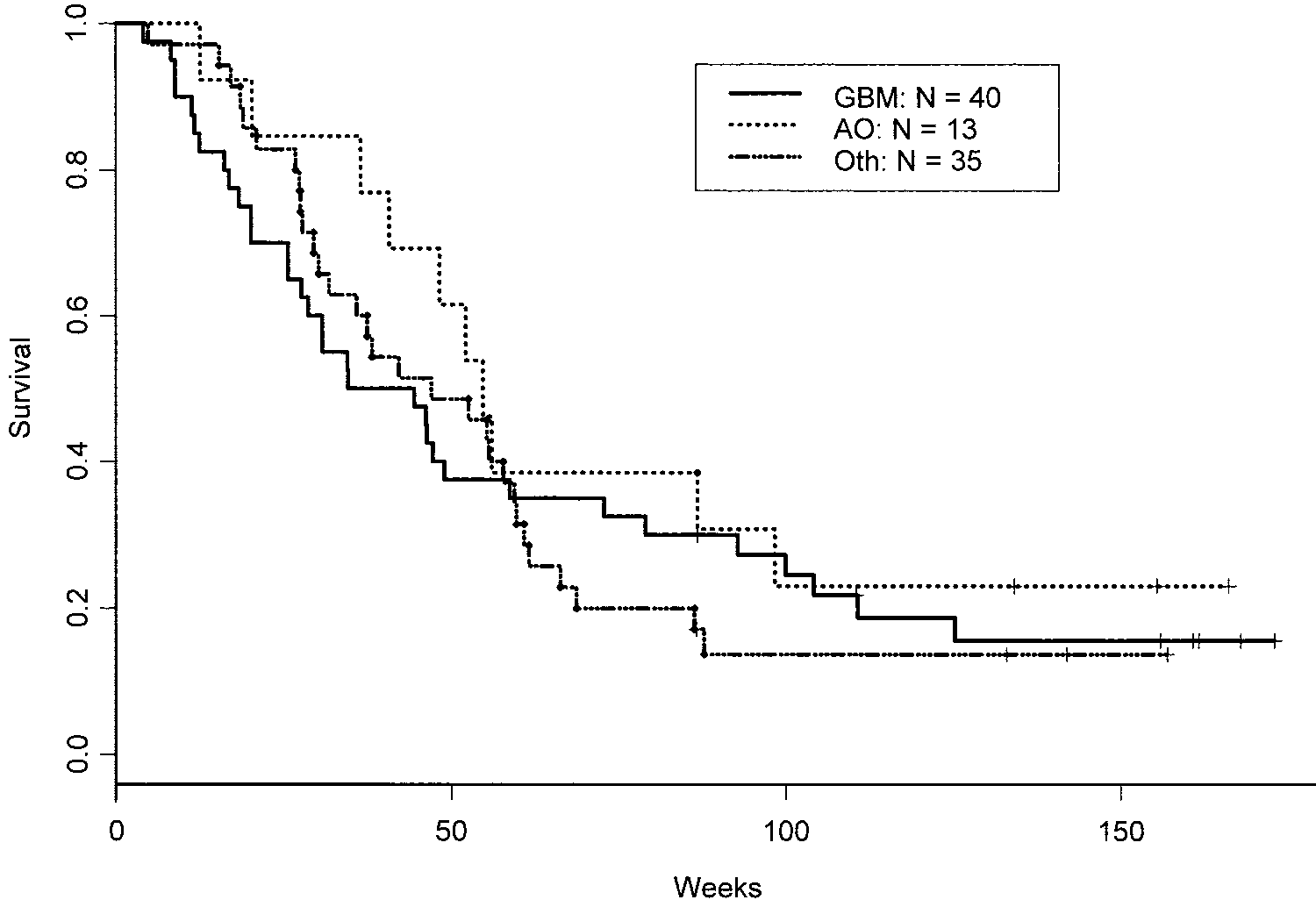 Table 3. Temozolomide and cis-Retinoic Acid in Recurrent Malignant Gliomas: Survival
Table 3. Temozolomide and cis-Retinoic Acid in Recurrent Malignant Gliomas: Survival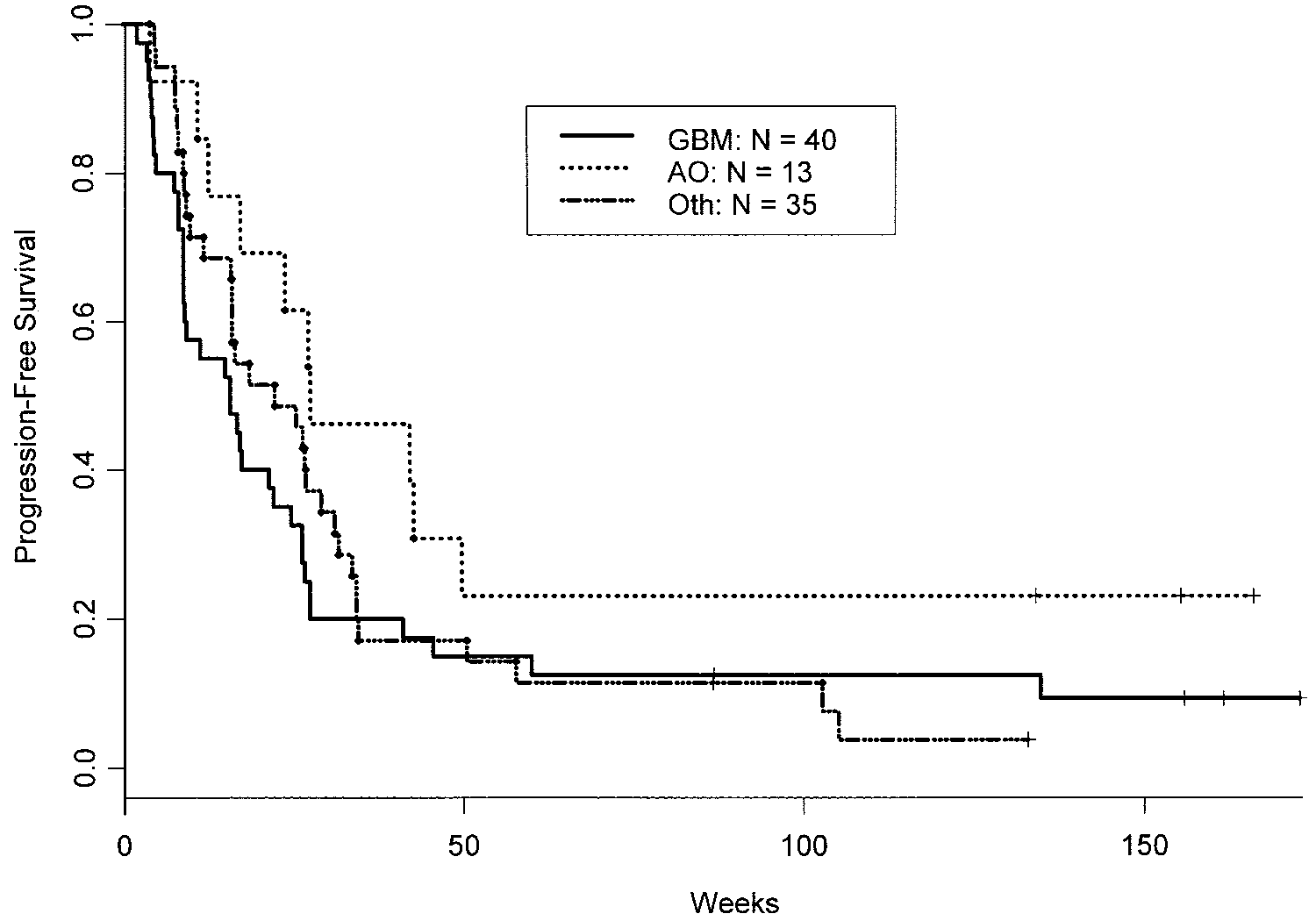 TMZ AND CRA FOR RECURRENT MALIGNANT GLIOMA
Fig 2. Progression-free survival by his-
TMZ AND CRA FOR RECURRENT MALIGNANT GLIOMA
Fig 2. Progression-free survival by his-