Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
1107.pdf
An Approach to Interpreting Spirometry TIMOTHY J. BARREIRO, D.O., and IRENE PERILLO, M.D. University of Rochester School of Medicine and Dentistry, Rochester, New York Spirometry is a powerful tool that can be used to detect, follow, and manage patients with lung dis- orders. Technology advancements have made spirometry much more reliable and relatively simple to incorporate into a routine office visit. However, interpreting spirometry results can be challeng- ing because the quality of the test is largely dependent on patient effort and cooperation, and the interpreter’s knowledge of appropriate reference values. A simplified and stepwise method is key to interpreting spirometry. The first step is determining the validity of the test. Next, the determination of an obstructive or restrictive ventilatory patten is made. If a ventilatory pattern is identified, its severity is graded. In some patients, additional tests such as static lung volumes, diffusing capacity of the lung for carbon monoxide, and bronchodilator challenge testing are needed. These tests can further define lung processes but require more sophisticated equipment and expertise available only in a pulmonary function laboratory. (Am Fam Physician 2004;69:1107-14. Copyright 2004 American Academy of Family Physicians.)
to 1994 found high rates of undiagnosed and untreated COPD in current and for-
nary disease (COPD) is the most common respiratory disease and the fourth lead-
mer smokers.5 Population-based studies have
identified vital capacity (VC) as a powerful
United States.1 Despite preventive efforts,
prognostic indicator in patients with COPD.
has doubled in the past decade, and this
forced vital capacity (FVC) as a risk factor
trend is likely to continue.2,3 Evidence indi-
for premature death.6 The Third National
cates that a patient’s history and physical
Health and Nutritional Examination Survey
examination are inadequate for diagnosing
showed potential benefits for patients with
early identification, intervention, and treat-
pulmonary function test provides the most
was the first study to show that early iden-
impairment, spirometry is the preferred test
tification and intervention in smokers could
for the diagnosis of COPD because it can
affect the natural history of COPD.7 These
surveys also showed that simple spirometry
could detect mild airflow obstruction, even
ever, the results must be correlated care-
fully with clinical and roentgenographic
data for optimal clinical application. This
article reviews the indications for use of
spirometry, provides a stepwise approach
Organization and the U.S. National Heart,
to its interpretation, and indicates when
lished the Global Initiative for Chronic Obstructive Lung Disease to increase
Background
Downloaded from the American Family Physician Web site at www.aafp.org/afp. Copyright 2004 American Academy of Family Physicians. For the pri-
vate, noncommercial use of one individual user of the Web site. All other rights reserved. Contact copyrights@aafp.org for copyright questions and/or
tion, followed by a forced expiration that rapidly
Normal lungs can empty more than 80 percent of their
empties the lungs. Expiration is continued for as long as possible or until a plateau in exhaled
volume is reached. These efforts are recorded and graphed. (A glossary of terms used in this article can be found in Table 1.)
Lung function is physiologically divided into
and to provide comprehensive treatment guide-
four volumes: expiratory reserve volume, inspira-
lines aimed at decreasing COPD-related morbid-
tory reserve volume, residual volume, and tidal
volume. Together, the four lung volumes equal the total lung capacity (TLC). Lung volumes
Spirometry Measurements
and their combinations measure various lung
and Terminology
capacities such as functional residual capacity
Spirometry measures the rate at which the
(FRC), inspiratory capacity, and VC. Figure 111
lung changes volume during forced breathing
shows the different volumes and capacities of
maneuvers. Spirometry begins with a full inhala-
The most important spirometric maneuver is the
FVC. To measure FVC, the patient inhales maxi-
Glossary
mally, then exhales as rapidly and as completely as possible. Normal lungs generally can empty
Spirometric values
more than 80 percent of their volume in six sec-
FVC—Forced vital capacity; the total volume of air that can be exhaled during a
onds or less. The forced expiratory volume in one
second (FEV1) is the volume of air exhaled in the
FEV1—Forced expiratory volume in one second; the volume of air exhaled in the
first second of the FVC maneuver. The FEV1/FVC
first second under force after a maximal inhalation.
ratio is expressed as a percentage (e.g., FEV1 of 0.5
FEV1/FVC ratio—The percentage of the FVC expired in one second.
L divided by FVC of 2.0 L gives an FEV1/FVC ratio
FEV6—Forced expiratory volume in six seconds. FEF25-75%—Forced expiratory flow over the middle one half of the FVC; the aver-
age flow from the point at which 25 percent of the FVC has been exhaled to the
Lung Volumes and Capacities
point at which 75 percent of the FVC has been exhaled.
MVV—Maximal voluntary ventilation. Lung volumes
ERV—Expiratory reserve volume; the maximal volume of air exhaled from end-
IRV—Inspiratory reserve volume; the maximal volume of air inhaled from end-
RV—Residual volume; the volume of air remaining in the lungs after a maximal
T—Tidal volume; the volume of air inhaled or exhaled during each respiratory
Lung capacities
FRC—Functional residual capacity; the volume of air in the lungs at resting end-
IC—Inspiratory capacity; the maximal volume of air that can be inhaled from the
TLC—Total lung capacity; the volume of air in the lungs at maximal inflation. Reprinted with permission from Gold WM. Pulmonary
VC—Vital capacity; the largest volume measured on complete exhalation after full
function testing. In: Murray JF, Nadel JA, eds. Textbook of respiratory medicine. 3d ed. Philadelphia: Saunders, 2000:783.Spirometry
of 25 percent). The absolute ratio is the value
low FEV1. Normal spirometric parameters are
used in interpretation, not the percent predicted.
Some portable office spirometers replace the
Indications for Office Spirometry
technician ease. The parameter is based on a
Spirometry is designed to identify and quan-
six-second maneuver, which incorporates a stan-
tify functional abnormalities of the respira-
dard time frame to decrease patient variability
tory system. The NLHEP recommends that pri-
and the risk of complications. One of the pit-
mary care physicians perform spirometry in
falls of using this type of spirometer is that it
patients 45 years of age or older who are
must be calibrated for temperature and water vapor. It should be used with caution in patients
Spirograms and Flow Volume Curves
with advanced COPD because of its inability to detect very low volumes or flows. However, the FEV
1/FEV6 ratio provides accurate surrogate
FEV1 and FEV6 values should be rounded to the
nearest 0.1 L and the percent predicted and the
curves are shown in Figure 2.11 It is important to understand that the amount exhaled during the
first second is a constant fraction of the FVC,
regardless of lung size. The significance of the
FEV1/FVC ratio is twofold. It quickly identifies patients with airway obstruction in whom the
FVC is reduced, and it identifies the cause of a
Normal Values of Pulmonary Function Tests
Absolute FEV1/FVC Within 5% of the predicted ratio
DLCO = diffusing capacity of lung for carbon monoxide.
FIGURE 2. Spirograms and flow volume curves. (A) Restrictive ventilatory defect.
Adapted with permission from Salzman SH. Pulmo-(B) Normal spirogram. (C) Obstructive ventilatory defect. nary function testing: tips on how to interpret the Reprinted with permission from Gold WM. Pulmonary function testing. In: Murray JF, Nadel JA, eds. Textbook of respiratory medicine. 3d ed. Philadelphia: Saunders, 2000:805.Indications for Spirometry Contraindications to Use of Spirometry Detecting pulmonary disease
Acute disorders affecting test performance (e.g.,
Hemoptysis of unknown origin (FVC maneuver may
Recent eye surgery (increases in intraocular
Recent myocardial infarction or unstable angina
Thoracic aneurysms (risk of rupture because of
Assessing severity or progression of disease Pulmonary diseases
current or former smokers; in patients who
have a prolonged or progressive cough or
sputum production; or in patients who have a
history of exposure to lung irritants.9 Other indications for spirometry are to determine the
strength and function of the chest, follow dis-
ease progression,15,16 assess response to treat-
ment,17,18 and obtain baseline measurements
before prescribing drugs that are potentially
toxic to the lungs, such as amiodarone (Corda-
rone) and bleomycin (Blenoxane).19 Spirometry
also is helpful in preoperative risk assessment
for many surgeries20-23 and often is used in
Risk stratification of patients for surgery
workers’ compensation and disability claims
to assess occupational exposure to inhalation
hazards.24 Tables 3 and 4 list indications and
Interpreting Spirometry Results
Spirometry requires considerable patient
effort and cooperation. Therefore, results must
be assessed for validity before they can be inter-
preted.17,25 Inadequate patient effort can lead
to misdiagnosis and inappropriate treatment. An
algorithm for interpreting spirometry results is
Evaluating disability or impairment
Social Security or other compensation programs
The clinical context of the test is important
because parameters in patients with mild disease can overlap with values in healthy persons.26 Normal spirometry values may vary, and interpre-
Spirometry
tation of results relies on the parameters used.
very tall patients or patients with missing lower
The normal ranges for spirometry values vary
extremities. FEV1 and FVC are greater in whites
depending on the patient’s height, weight, age, sex,
compared with blacks and Asians. FVC and VC
and racial or ethnic background.27,28 Predicted
values vary with the position of the patient. These
values for lung volumes may be inaccurate in
variables can be 7 to 8 percent greater in patients
Interpreting Spirometry Results
Determine if the test is interpretable.
increase in FEV1 and 200 mL increase in FVC or FEV1,
FIGURE 3. Algorithm for interpreting results of spirometry. (DLCO = diffusing capacity of lung for carbon monoxide; VA = alveolar vol-
and FEV1 are decreased, the distinction between
an obstructive and restrictive ventilatory pat-
1/FVC ratio distinguishes obstructive from
tern depends on the absolute FEV1/FVC ratio.
If the absolute FEV1/FVC ratio is normal or increased, a restrictive ventilatory impairment may be present. However, to make a definitive
who are sitting during the test compared with
diagnosis of restrictive lung disease, the patient
patients who are supine. FVC is about 2 percent
should be referred to a pulmonary laboratory
greater in patients who are standing compared
for static lung volumes. If the TLC is less than
80 percent, the pattern is restrictive, and dis-
To determine the validity of spirometric results,
eases such as pleural effusion, pneumonia, pul-
at least three acceptable spirograms must be
monary fibrosis, and congestive heart failure
obtained. In each test, patients should exhale
for at least six seconds and stop when there is
A reduced FEV1 and absolute FEV1/FVC ratio
no volume change for one second. The test ses-
indicates an obstructive ventilatory pattern,
sion is finished when the difference between the
and bronchodilator challenge testing is recom-
two largest FVC measurements and between the
mended to detect patients with reversible airway
two largest FEV1 measurements is within 0.2 L. If
obstruction (e.g., asthma). A bronchodilator is
both criteria are not met after three maneuvers,
given, and spirometry is repeated after several
the test should not be interpreted. Repeat test-
minutes. The test is positive if the FEV1 increases
ing should continue until the criteria are met or
by at least 12 percent and the FVC increases by
until eight tests have been performed.26
at least 200 mL. The patient should not use any
Figure 425 shows normal flow-volume and
bronchodilator for at least 48 hours before
time-volume curves. Notice that the lines of
the test. A negative bronchodilator response
the flow-volume curve are free of glitches and
does not completely exclude the diagnosis of
irregularities. The volume-time curve extends
longer than six seconds, and there are no signs
The mid-expiratory flow rate (FEF25-75%) is the
average forced expiratory flow rate over the
If the test is valid, the second step is to
middle 50 percent of the FVC. It can help in the
determine whether an obstructive or restrictive
diagnosis of an obstructive ventilatory pattern.
ventilatory pattern is present. When the FVC
Because it is dependent on FVC, the FEF25-75% is highly variable. In the correct clinical situation, a reduction in FEF25-75% of less than 60 percent
of that predicted and an FEV1/FVC ratio in
TIMOTHY J. BARREIRO, D.O., is a second-year pulmonary disease and critical care medi-
the low to normal range may confirm airway
cine fellow at the University of Rochester (N.Y.) School of Medicine and Dentistry, Strong
Memorial Hospital. Dr. Barreiro earned his medical degree from Ohio University College of Osteopathic Medicine, Athens, and completed an internal medicine residency at
Allegheny General Hospital in Pittsburgh, Pa.
maneuver is another test that can be used to
IRENE PERILLO, M.D., is assistant professor of medicine and director of the outpatient
confirm obstructive and restrictive conditions.
pulmonary clinic at the University of Rochester School of Medicine and Dentistry, Strong
The patient is instructed to breathe as hard
Memorial Hospital. Dr. Perillo earned her medical degree from State University of New
and fast as possible for 12 seconds. The result
York Upstate Medical University, Syracuse, and completed an internal medicine resi-dency, and pulmonary and critical care fellowship at the University of Rochester School
is extrapolated to 60 seconds and reported
in liters per minute. MVV generally is approxi-
Address correspondence to Timothy J. Barreiro, D.O., University of Rochester School of
mately equal to the FEV1 40. A low MVV
Medicine and Dentistry, 601 Elmwood Ave., Box 692, Rochester, NY 14642 (e-mail: Timo-
can occur in obstructive disease but is more
thy_Barreiro@urmc.rochester.edu). Reprints are not available from the authors.
common in restrictive conditions. If the MVV is low but FEV1 and FVC are normal, poor patient
Spirometry Spirometric Flow Diagram
The final step in interpreting spirometry is
to determine if additional testing is needed to further define the abnormality detected by spi-rometry. Measurement of static lung volumes,
including FRC, is required to make a definitive
diagnosis of restrictive lung disease. Final Comment
Basic spirometry can be performed in the
family physician’s office with relative ease and
inexpensive equipment. In most cases, office spi-
rometry provides an adequate assessment of pulmonary function. In addition, spirometry may
be used to address major issues in clinical man-
The authors indicate that they do not have any con-flicts of interest. Sources of funding: none reported.
1. Murray CJ, Lopez AD. Evidence-based health pol-
icy—lessons from the Global Burden of Disease
2. Murray CJ, Lopez AD. Alternative projections of
mortality and disability by cause 1990-2020: Global
Burden of Disease Study. Lancet 1997;349: 1498-
3. Murray CJ, Lopez AD. Global mortality, disability,
and the contribution of risk factors: Global Burden
of Disease Study. Lancet 1997;349:1436-42.
4. Holleman DR Jr, Simel DL. Does the clinical exami-
nation predict airflow limitation? JAMA 1995;273:
5. Mannino DM, Gagnon RC, Petty TL, Lydick E. Obstruc-
tive lung disease and low lung function in adults in
FIGURE 4. Normal spirometric flow diagram. (A)
the United States: data from the National Health
Flow-volume curve. (B) Volume-time curve. The
and Nutrition Examination Survey, 1988-1994. Arch
smooth lines, expiratory time of greater than six
6. Kannel WB, Hubert H, Lew EA. Vital capacity as a
seconds, and quick peak of the peak expiratory flow
predictor of cardiovascular disease: the Framingham
rate indicate a good spirometric effort.
Reprinted with permission from Crapo RO. Pulmonary-
7. Anthonisen NR, Connett JE, Kiley JP, Altose MD,
function testing. N Engl J Med 1994;331:28.
Bailey WC, Buist AS, et al. Effects of smoking inter-vention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1. The
Lung Health Study. JAMA 1994;272:1497-505.
8. Harris T, Woteki C, Briefel RR, Kleinman JC. NHANES
III for older persons: nutrition content and method-
effort, a neuromuscular disorder, or major
ological considerations. Am J Clin Nutr 1989;50(5
Once the ventilatory pattern is identified, the
9. Petty TL, Weinmann GG. Building a national strat-
egy for the prevention and management of and
severity of the disease must be determined. The
research in chronic obstructive pulmonary disease.
American Thoracic Society has developed a scale
National Heart, Lung, and Blood Institute Workshop
to rate the severity of disease based on predicted
Summary. Bethesda, Maryland, August 29-31, 1995. JAMA 1997;277:246-53.
10. Pauwels RA, Buist AS, Calverley PM, Jenkins CR,
Spirometry
Hurd SS; GOLD Scientific Committee. Global strategy
for the diagnosis, management, and prevention of
21. Celli BR. What is the value of preoperative pulmonary
chronic obstructive pulmonary disease. NHLBI/WHO
function testing? Med Clin North Am 1993;77:309-
Global Initiative for Chronic Obstructive Lung Dis-
ease (GOLD) Workshop summary. Am J Respir Crit
22. Culver BH. Preoperative assessment of the thoracic
surgery patient: pulmonary function testing. Semin
11. Gold WM. Pulmonary function testing. In: Murray JF,
Thorac Cardiovasc Surg 2001;13:92-104.
Nadel JA, eds. Textbook of respiratory medicine, 3d
23. Powell CA, Caplan CE. Pulmonary function tests in
ed. Philadelphia: Saunders, 2000:781-871.
preoperative pulmonary evaluation. Clin Chest Med
12. Hankinson JL, Odencrantz JR, Fedan KB. Spiromet-
ric reference values from a sample of the general
24. Sood A, Redlich CA. Pulmonary function tests at
U.S. population. Am J Respir Crit Care Med 1999;
work. Clin Chest Med 2001;22:783-93.
25. Crapo RO. Pulmonary-function testing. N Engl J Med
13. Ferguson GT, Enright PL, Buist AS, Higgins MW.
Office spirometry for lung health assessment in
26. Crapo RO, Morris AH. Pulmonary function testing:
adults: A consensus statement from the National
sources of error in measurement and interpretation.
Lung Health Education Program. Chest 2000;117:
27. Petty TL. Simple office spirometry. Clin Chest Med
14. Salzman SH. Pulmonary function testing: tips on how
to interpret the results. J Respir Dis 1999;20:809-22.
28. Margolis ML, Montoya FJ, Palma WR Jr. Pulmonary
15. Alhamad EH, Lynch JP 3d, Martinez FJ. Pulmonary
function tests: comparison of 95th percentile-based
function tests in interstitial lung disease: what role
and conventional criteria of normality. South Med J
do they have? Clin Chest Med 2001;22:715-50,ix.
16. Flaherty KR, Martinez FJ. The role of pulmonary func-
29. Lung function testing: selection of reference values
tion testing in pulmonary fibrosis. Curr Opin Pulm
and interpretative strategies. American Thoracic Soci-
ety. Am J Respir Crit Care Med 1991;144:1202-18.
17. Colp CR. Interpretation of pulmonary function tests.
18. Rosenberg DM, Weinberger SE, Fulmer JD, Flye MW,
Fauci AS, Crystal RG. Functional correlates of lung involvement in Wegener’s granulomatosis. Use of pulmonary function tests in staging and follow-up. Am J Med 1980;69:387-94.
19. Kanji Z, Sunderji R, Gin K. Amiodarone-induced pul-
monary toxicity. Pharmacotherapy 1999;19:1463-6.
20. Dunn WF, Scanlon PD. Preoperative pulmonary func-
tion testing for patients with lung cancer. Mayo Clin
Enantioselective Synthesis of a-Hydroxy Ketones via Benzaldehyde Lyase-Catalyzed CÀC Bond Formation ReactionAyhan S. Demir,a,* ÷zge SÀesÀenoglu,a Elif Eren,a Birsu Hosrik,a Martina Pohl,b,dElena Janzen,b Doris Kolter,c Ralf Feldmann,c Pascal D¸nkelmann,c Michael M¸llerc,*Department of Chemistry, Middle East Technical University, 06531 Ankara, Turkey,Fax: ( 90)-312-2101280, e-mail: asdem
Lääkeaine- ja huumausaineanalytiikka Drug and Drugs of abuse analytics 05.07.2013 Päätöksen päiväys / Date of decision Päätöksen viimeinen voimassaolopäivä / Date of expiry Voimassaoleva pätevyysalue / Current scope of accreditation YHTYNEET MEDIX LABORATORIOT OY UNITED MEDIX LABORATORIES LTD Tunnus Yksikkö tai toimintoala Puh./fax/e-mail/www Co
 An Approach to Interpreting Spirometry
An Approach to Interpreting Spirometry 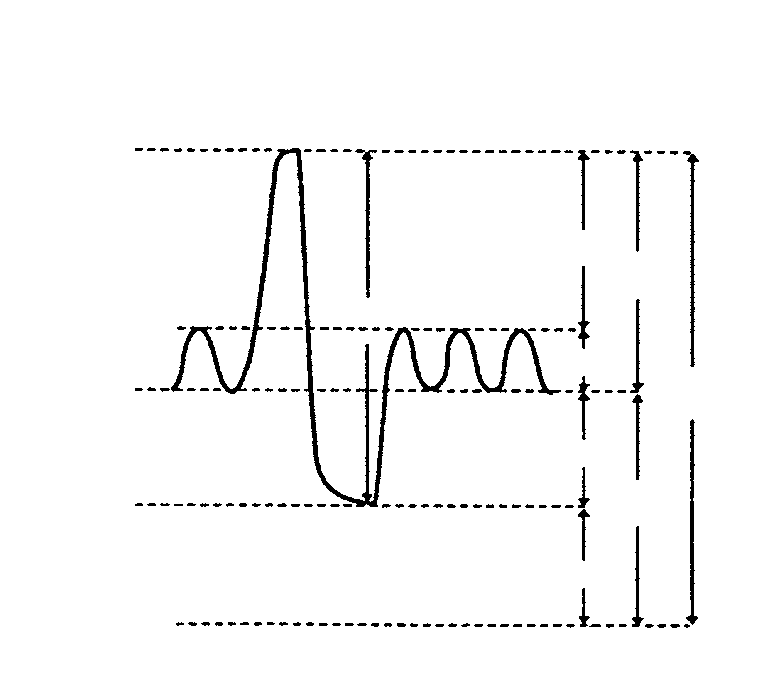 tion, followed by a forced expiration that rapidly
Normal lungs can empty more than 80 percent of their
empties the lungs. Expiration is continued for as long as possible or until a plateau in exhaled
volume is reached. These efforts are recorded and graphed. (A glossary of terms used in this article can be found in Table 1.)
Lung function is physiologically divided into
and to provide comprehensive treatment guide-
four volumes: expiratory reserve volume, inspira-
lines aimed at decreasing COPD-related morbid-
tory reserve volume, residual volume, and tidal
volume. Together, the four lung volumes equal the total lung capacity (TLC). Lung volumes
Spirometry Measurements
tion, followed by a forced expiration that rapidly
Normal lungs can empty more than 80 percent of their
empties the lungs. Expiration is continued for as long as possible or until a plateau in exhaled
volume is reached. These efforts are recorded and graphed. (A glossary of terms used in this article can be found in Table 1.)
Lung function is physiologically divided into
and to provide comprehensive treatment guide-
four volumes: expiratory reserve volume, inspira-
lines aimed at decreasing COPD-related morbid-
tory reserve volume, residual volume, and tidal
volume. Together, the four lung volumes equal the total lung capacity (TLC). Lung volumes
Spirometry Measurements 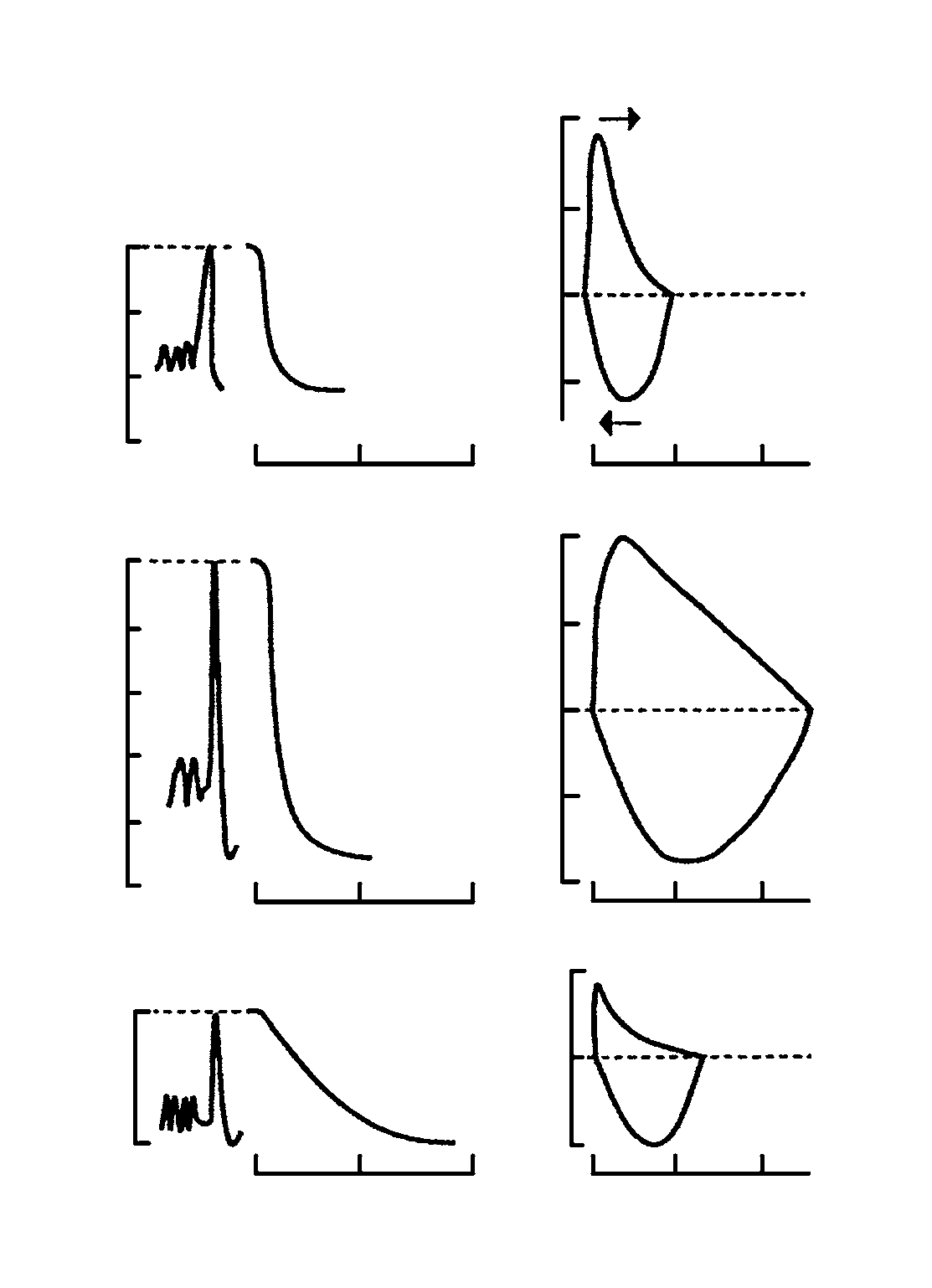 Spirometry
Spirometry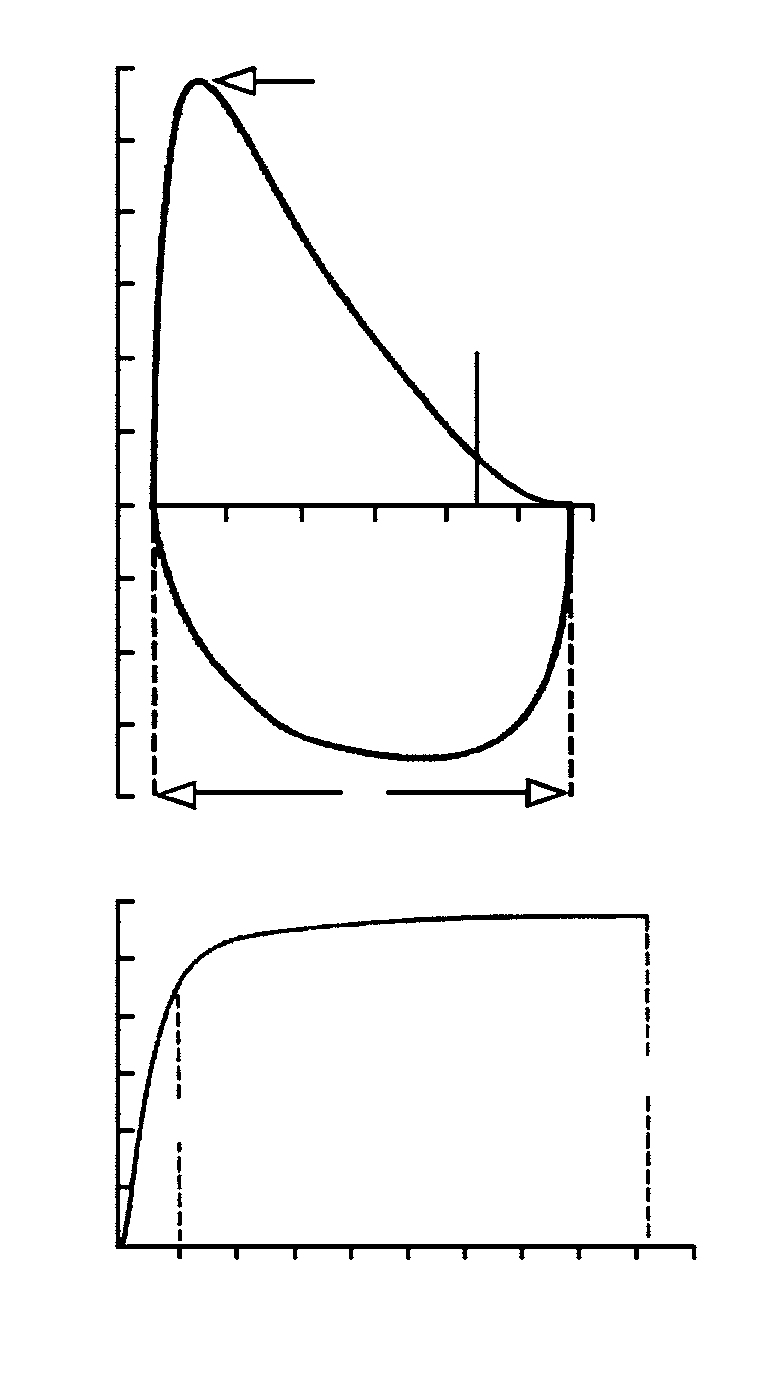 Spirometry
Spirometry