Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Http:
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
Licensed to University of California - SF New Search Contents Feedback
Official reprint from UpToDate® www.uptodate.com The surgical patient taking glucocorticoids
Gail A Welsh, MD Ellen F Manzullo, MD, FACP Lynnette K Nieman, MD
UpToDate performs a continuous review of over 375 journals and other resources. Updates are added asimportant new information is published. The literature review for version 15.1 is current throughDecember 2006; this topic was last changed on May 8, 2006. The next version of UpToDate (15.2) willbe released in June 2007.INTRODUCTION — Chronic glucocorticoid therapy can suppress the hypothalamic-pituitary-adrenal (HPA) axis and, during times of stress such as surgery, the adrenal glands may not respond appropriately. Protocols for "stress dose" steroids followed reports in the 1950s of possible surgery-associated adrenal insufficiency due to sudden preoperative withdrawal of glucocorticoids. However, recent studies have questioned both the need for and current dosage regimens of supplemental perioperative glucocorticoids [1-3].
In addition to HPA axis suppression, chronic glucocorticoid therapy may cause a number of otherproblems in the perioperative period:
Impaired wound healing [4]Increased friability of skin, superficial blood vessels, and other tissues (eg, mild pressure may cause
hematoma or skin ulceration, removing adhesive tape may tear the skin, and sutures may tear the gutwall)
Increased risk of fracture, infections, gastrointestinal hemorrhage, or ulcer [5,6]. (See "Major side
effects of systemic glucocorticoids").
The management of the surgical patient on chronic glucocorticoid therapy is reviewed here. Perioperativeglucocorticoid regimens for patients taking replacement glucocorticoid for primary adrenal insufficiencyare addressed separately. (See "Treatment of adrenal insufficiency"). CORTISOL SECRETION DURING STRESS — Acute physical or psychological stress activates the HPA axis, resulting in increased plasma corticotropin (ACTH) and serum cortisol concentrations. Stress exerts its effects by stimulating the hypothalamus to release ACTH secretagogues, with corticotropin-releasing hormone (CRH) and arginine vasopressin (AVP) being the most important [7,8]. (See "ACTH and cortisol secretion in health and disease").
Surgery is one of the most potent activators of the HPA axis. Plasma ACTH concentrations increase at
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
the time of incision and during surgery, but the greatest ACTH and cortisol secretion occurs duringreversal of anesthesia, extubation, and in the immediate postoperative recovery period, primarily itappears, in response to pain [9,10]. The response is mediated by afferent nerve impulses, since it canbe abolished by interrupting the neural connections from the operative site, such as by sectioning thespinal cord [11], epidural anesthesia [12], or local anesthesia. The plasma ACTH and serum cortisolresponses to surgery can also be reduced by opiate drugs [10,13].
There is considerable variation in the increase in cortisol secretion among individuals undergoingsurgery; this variability is in part due to concomitant medication use, age, and concurrent illness. Ingeneral, the adrenal gland produces about 50 mg/day of cortisol during a minor procedure or surgery(normal basal secretion is 8 to 10 mg/day), while 75 to 100 mg/day are produced with major surgery[14]. The cortisol secretion rate can reach 200 to 500 mg/day with severe stress, but secretion ratesgreater than 200 mg/day in the 24 hours after surgery are rare [2]. Effect of exogenous glucocorticoids — Both endogenous and exogenous glucocorticoids exert negative feedback control on the HPA axis by suppressing CRH secretion and, consequently, ACTH secretion. This leads to adrenal atrophy and loss of cortisol secretory capability.
Prednisone doses of less than 5 mg/day given in the morning do not suppress the HPA axis. Patients ondoses of 5 mg/day or higher have considerable variability in HPA axis suppression that does notcorrelate well with age, sex, dose, or duration of therapy [15,16]. This variability is probably due todifferences in rates of glucocorticoid metabolism (show figure 1). It can be assumed that equivalentmorning dosages of other glucocorticoids (eg, 4 mg/day of methylprednisolone, 0.5 mg/day ofdexamethasone, or 20 mg/day of hydrocortisone) have a similar effect. (show table 1). (See "Pharmacologicuse of glucocorticoids").
The following patients can be considered not to have suppression of their hypothalamic-pituitary-adrenalaxis:
Any patient who has received any dose of glucocorticoid for less than three weeks.
Patients who have received morning doses of less than 5 mg/day of prednisone or its equivalent.
Patients treated with alternate-day glucocorticoid therapy [17-19].
In contrast, patients who should be assumed to have functional suppression of hypothalamic-pituitary-adrenal function include:
Any patient who has received more than 20 mg/day of prednisone or its equivalent (eg, 16 mg/day of
methylprednisolone, 2 mg/day of dexamethasone, or 80 mg/day of hydrocortisone) for more than threeweeks [20].
Any patient who has clinical Cushing's syndrome.
The intermediate categories of patients are more problematic; specific testing may be necessary todetermine the presence of HPA axis suppression (see "Evaluation of HPA axis suppression" below). Inhaled and topical glucocorticoids — Chronic use of inhaled or high potency topical glucocorticoids
A meta-analysis of 21 studies of urinary cortisol excretion and 13 studies of morning serum cortisol
concentrations in patients taking inhaled glucocorticoids found evidence of HPA axis suppression thatwas most common with glucocorticoid doses greater than 0.8 mg/day, but was often absent even athigher doses [21]. HPA axis suppression was seen with lower doses of fluticasone than withbeclomethasone, triamcinolone, or budesonide.
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
A new inhaled agent, ciclesonide, is hydrolyzed to its active metabolite, desisobutyryl-CIC (des-CIC),
in the lungs, limiting systemic availability. A meta-review of four studies using the agent at doses of 160to 640 mcg/d did not show evidence for suppression of morning or 24-hour urinary cortisol [22].
Class I topical glucocorticoids (the most potent) in doses as little as 2 g/day can cause significant
HPA axis suppression [23,24]. In one report, temporary reversible HPA axis suppression was noted in 8of 40 patients (20 percent) with psoriasis treated with superpotent topical glucocorticoid for three weeksor more [25]. Factors that predispose to HPA axis suppression include use of high potencyglucocorticoids, chronic use, application to the scalp or intertriginous areas, treatment of large areas,occlusion with impermeable dressings, poor skin integrity, liver failure, and young age. (See"Pharmacologic use of glucocorticoids"). EVALUATION OF HPA AXIS SUPPRESSION — Patients taking 5 to 20 mg/day of prednisone or its equivalent for more than three weeks may or may not have suppression of the HPA axis. The patient who has discontinued glucocorticoids in the year prior to surgery presents another problem. Early studies found that profound suppression of the HPA axis could take up to one year to recover fully [26,27]. This led some to recommend the administration of glucocorticoids to any patient who had been on prednisone doses of more than 5 mg/day for more than one week in the 6 to 12 months prior to surgery, but this is clearly unwarranted. (See "Glucocorticoid withdrawal").
In patients whose HPA axis status is uncertain, one can give glucocorticoids perioperatively or, if timepermits, test for the responsiveness of the adrenal to ACTH stimulation. (See "Evaluation of the responseto ACTH in adrenal insufficiency"). A normal serum cortisol response to ACTH stimulation is predicated onthe assumption that the adrenal gland has been stimulated with sufficient endogenous ACTH each day toprevent adrenal atrophy and to maintain the activity of the steroidogenic enzymes.
However, some have questioned whether the high-dose (250 microgram) ACTH stimulation testaccurately predicts the ability of a patient to respond adequately to stress, since occasional patientshave normal responses to ACTH, but subnormal serum cortisol responses to insulin-inducedhypoglycemia (a sensitive measure of HPA axis suppression) [28,29]. Some studies found that the ACTHstimulation test predicted both the response to stress and surgical complications [30], but severalsubsequent reports have shown that patients who have laboratory evidence of HPA axis suppression mayhave a normal clinical response to surgical stress [1,31,32].
In a prospective study of 40 renal allograft recipients admitted with significant physiologic stress,
including sepsis, metabolic abnormalities, and surgery, the patients received only their baselineprednisone (5 to 10 mg/day) and no stress doses of glucocorticoids [1]. The clinical course of thepatients revealed no evidence of adrenal insufficiency. Five episodes of hyponatremia and seveninstances of hypotension were attributed to primary disease processes and responded promptly tospecific treatment without steroid supplementation. Biochemical evaluation during stress revealedsuppression of the plasma ACTH concentration in 75 percent of episodes, elevation of urinary freecortisol excretion in 79 percent, and elevation of the serum cortisol concentration in 56 percent. Thesefindings suggest that these patients had physiologically adequate adrenal function. The ACTH stimulationtest overestimated the incidence and degree of clinically significant adrenal dysfunction (63 percent ofpatients) and was not a useful indication of a requirement for additional glucocorticoids.
In a study of 18 patients who had been taking at least 7.5 mg/day of prednisone for several months
and had secondary adrenal insufficiency as defined by ACTH stimulation testing, the patients wererandomly assigned to two groups: one group received perioperative injections of saline solution alone(n=12) and the other received perioperative saline solution and hydrocortisone (n=6) [31]. All patientsreceived their usual daily prednisone dose throughout the study. Most subjects underwent majoroperations such as joint replacements and abdominal operations. One patient in each group hadhypotension that resolved with volume replacement alone. The average pulse rates and blood pressureswere similar in the two groups during the perioperative period.
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
Rare patients who respond normally to the high-dose ACTH test have a subnormal serum cortisolresponse to surgery [33]. Nevertheless, they tolerate surgery well [34], presumably because more thanbasal daily cortisol secretion is not necessary to survive surgery [35].
Thus, with one exception, any patient who responds normally to the high-dose ACTH test does notrequire glucocorticoid supplementation perioperatively. The exception is the patient who is acutely ACTH-deficient, as might occur soon after pituitary surgery [29]. In these cases the low-dose (1 microgram)ACTH stimulation test, insulin tolerance test or metyrapone stimulation test may detect adrenalinsufficiency better than the high-dose test, and similar considerations perioperatively likely apply. (See"Diagnosis of adrenal insufficiency"). RECOMMENDATIONS — Several authors have recommended that patients on chronic glucocorticoids undergoing surgery receive only their usual daily dose of glucocorticoid perioperatively. These recommendations are based upon studies that have shown that no surgical patient who was treated with his usual steroid dose developed intraoperative or postoperative hypotension or any other perioperative signs of adrenal insufficiency [1,31,32]. However, the clinician may decide that even a small risk of adrenal insufficiency outweighs the risk of 24 to 48 hours of stress doses of glucocorticoid.
In general, patients who have taken any dose of glucocorticoids for less than three weeks or who havetaken chronic alternate day therapy are unlikely to have a suppressed HPA axis and should continue ontheir usual dose of glucocorticoids perioperatively.
HPA axis suppression should be assumed to be present in patients taking prednisone at a dose greaterthan 20 mg/day for three weeks or more, and in patients with a Cushingoid appearance. Two groupssuggested guidelines for glucocorticoid coverage in these individuals that takes into account themagnitude of the stress based upon type and duration of surgery, and the known glucocorticoidproduction rates associated with it (show table 2) [2,36]. However, a replacement dosage ofglucocorticoid appears to be sufficient for most patients even during major surgery. If higher dosagesare used, patients should revert to the usual replacement dose within 48 hours of surgery, unless othercircumstances intervene.
Patients on intermediate doses of glucocorticoids should undergo testing. A normal response tocortrosyn, 250 ug, does not exclude adrenal insufficiency, but a subnormal response indicates adrenalsuppression [37]. The low-dose ACTH stimulation test, insulin tolerance test or metryrapone stimulationtest may be used to assess possible HPA axis suppression. (See "Diagnosis of adrenal insufficiency"). Whilethese tests do not absolutely predict the stress response to surgery, it is generally safe to assume thatpatients who respond normally do not require increased doses of glucocorticoid perioperatively. Theexception is the patient who is acutely ACTH-deficient, as might occur soon after pituitary surgery [29]. Patients with a subnormal response to the ACTH stimulation test should receive glucocorticoid (show table1).
Physicians should be aware of the potential for subclinical adrenal suppression in any patient who hasbeen using prolonged high-dose inhaled or topical glucocorticoids [21,23-25]. Nevertheless, it seemsreasonable to withhold glucocorticoids in these patients unless they appear Cushingoid or exhibit signsor symptoms of adrenal insufficiency perioperatively.
Patients who are taking glucocorticoids should be monitored carefully for infection postoperatively,because glucocorticoids may suppress the fever response.
Use of UpToDate is subject to the Subscription and License Agreement. REFERENCES
Bromberg, JS, Alfrey, EJ, Barker, CF, et al. Adrenal suppression and steroid supplementation in
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
renal transplant recipients. Transplantation 1991; 51:385.
Salem, M, Tainsh, RE, Bromberg, J, et al. Perioperative glucocorticoid coverage: a reassessment 42years after the emergence of a problem. Ann Surg 1994; 219:416.
Shaw, M, Mandell, BF. Perioperative management of selected problems in patients with rheumaticdiseases. Rheum Dis Clin North Am 1999; 25:623.
Anstead, GM. Steroids, retinoids, and wound healing. Adv Wound Care 1998; 11:277.
Stuck, AE, Minder, CE, Frey, FJ. Risk of infectious complications in patients takingglucocorticosteroids. Rev Infect Dis 1989; 11:954.
BOLLET, AJ, BLACK, R, BUNIM, JJ. Major undesirable side-effects resulting from prednisolone andprednisone. J Am Med Assoc 1955; 158:459.
Antoni, FA. Hypothalamic control of adrenocorticotropin secretion: Advances since the discovery of41-residue corticotropin-releasing factor. Endocr Rev 1986; 7:351.
Aguilera, G. Regulation of pituitary ACTH secretion during chronic stress. Front Neuroendocrinol1994; 15:321.
Udelsman, R, Norton, JA, Jelenich, SE, et al. Responses of the hypothalamic-pituitary-adrenal andrenin- angiotensin axes and the sympathetic system during controlled surgical and anestheticstress. J Clin Endocrinol Metab 1987; 64:986.
10. Raff, H, Norton, AJ, Flemma, RJ, Findling, JW. Inhibition of the adrenocorticotropin response to
surgery in humans: Interaction between dexamethasone and fentanyl. J Clin Endocrinol Metab1987; 65:295.
11. Redgate, ES. Spinal cord and ACTH release in adrenalectomized rats following electrical stimulation.
12. Brandt, M, Kehlet, H, Binder, C, et al. Effect of epidural analgesia on the glycoregulatory endocrine
response to surgery. Clin Endocrinol (Oxf) 1976; 5:107.
13. George, JM, Reier, CE, Lanese, RR, Rower, JM . Morphine anesthesia blocks cortisol and growth
hormone response to surgical stress in humans. J Clin Endocrinol Metab 1974; 38:736.
14. Lamberts, SW, Bruining, HA, deJong, FH. Corticosteroid therapy in severe illness. N Engl J Med
15. LaRochelle, GE, LaRochelle, AG, Ratner, RE, Borenstein, DG. Recovery of the hypothalamic-
pituitary-adrenal (HPA) axis in patients with rheumatic diseases receiving low-dose prednisone. AmJ Med 1993; 95:258.
16. Schlaghecke, R, Kornely, E, Santen, RT, et al. The effect of long-term glucocorticoid therapy on
pituitary-adrenal responses to exogenous corticotropin-releasing hormone. N Engl J Med 1992;326:226.
17. Harter, JG, Reddy, WJ, Thorn, GW. Studies on an intermittent corticosteroid dosage regimen. N
18. Fauci, AS. Alternate-day corticosteroid therapy. Am J Med 1978; 64:729. 19. Ackerman, GL, Nolsn, CM. Adrenocortical responsiveness after alternate-day corticosteroid therapy.
20. Christy, NP. corticosteroid withdrawal. In: Current Therapy in Endocrinology and Metabolism, 3d ed,
Bardin, CW (Ed), BC Decker, New York 1988, p. 113.
21. Lipworth, BJ. Systemic adverse effects of inhaled corticosteroid therapy: a systematic review and
meta-analysis. Arch Intern Med 1999; 159:941.
22. Dahl, R. Systemic side effects of inhaled corticosteroids in patients with asthma. Respir Med 2006.
23. Walsh, P, Aeling, Jl, Huff, L, Weston, WL. Hypothalamus-pituitary-adrenal axis suppression by
superpotent topical steroids. J Am Acad Dermatol 1993; 29:501.
24. Keipert, JA, Kelly, R. Temporary Cushing's syndrome from percutaneous absorption of
betamethasone 17-valerate. Med J Aust 1971; 1:542.
25. Katz, HI, Hien, NT, Prawer, SE, et al. Superpotent topical steroid treatment of psoriasis vulgaris -
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
clinical efficacy and adrenal function. J Am Acad Dermatol 1987; 16:804.
26. Livanou, T, Ferriman, D, James, VH. Recovery of hypothalamo-pituitary-adrenal function after
corticosteroid therapy. Lancet 1967; 2:856.
27. Graber, AL, Ney, RL, Nicholson, WE, et al. Natural history of pituitary-adrenal recovery following
long-term suppression with corticosteroids. J Clin Endocrinol Metab 1965; 25:11.
28. Lindholm, J, Kehlet, H. Re-evaluation of the clinical value of the 30 min ACTH test in assessing the
hypothalamic-pituitary-adrenocortical function. Clin Endocrinol 1987; 26:53.
29. Borst, GC, Michenfelder, HJ, O'Brian, JT. Discordant cortisol response to exogenous ACTH and
insulin-induced hypoglycemia in patients with pituitary disease. N Engl J Med 1982; 306:1462.
30. Jasani, MK, Freeman, PA, Boyle, JA, et al. Cardiovascular and plasma cortisol responses to surgery
in corticosteroid-treated R. A. patients. Acta Rheumatol Scand 1968; 14:65.
31. Glowniak, JV, Loriaux, DL. A double-blind study of perioperative steroid requirements in secondary
adrenal insufficiency. Surgery 1997; 121:123.
32. Kehlet, H, Binder, C. Adrenocortical function and clinical course during and after surgery in
unsupplemented glucocorticoid-treated patients. Br J Anaesth 1973; 45:1043.
33. Kehlet, H, Binder, C. Value of an ACTH test in assessing hypothalamic-pituitary-adrenocortical
function in glucocorticoid-treated patients. Br Med J 1973; 2:147.
34. Jasani, MK, Freeman, PA, Boyle, JA, et al. Studies of the rise in plasma 11-hydroxycorticosteroids
(11-OHCS) in corticosteroid-treated patients with rheumatoid arthritis during surgery: Correlationswith the functional integrity of the hypothalamo-pituitary-adrenal axis. Q J Med 1968; 37:407.
35. Udelsman, R, Ramp, J, Gallucci, WT, et al. Adaptation during surgical stress: A reevaluation of the
role of glucocorticoids. J Clin Invest 1986; 77:1377.
36. Coursin, DB, Wood, KE. Corticosteroid supplementation for adrenal insufficiency. JAMA 2002;
37. Dorin, RI, Qualls, CR, Crapo, LM. Diagnosis of adrenal insufficiency. Ann Intern Med 2003; 139:194.
Erratum in: Ann Intern Med 2004; 140:315. GRAPHICS Prednisone metabolism toxicity Prednisolone metabolism may influence side effects
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
Disappearance curves of tritiated prednisolone in five patients whodid not develop side effects while taking prednisone and in eightwho did. The patients who developed side effects clearedprednisolone from the circulation more slowly. Data fromKozower, M, Veatch, L, Kaplan, MM, J Clin Endocrinol Metab 1974;38:407.Corticosteroid preparations Comparison of commonly corticosteroid preparations Approximate equivalent dose, mg Relative potency Corticosteroid coverage surgery Corticosteroid coverage for surgery in patients taking exogenous corticosteroids
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
For minor procedures or surgery under local anesthesia (eg, inguinal hernia repair) take usualmorning steroid dose. No extra supplementation is necessary.
For moderate surgical stress (eg, lower extremity revascularization, total joint replacement) take usualmorning steroid dose. Give 50 mg hydrocortisone intravenously just before the procedure and 25 mgof hydrocortisone every 8 hours for 24 hours. Resume usual dose thereafter.
For major surgical stress (eg, esophagogastrectomy, total proctocolectomy) take usual am steroiddose. Give 100mg of intravenous hydrocortisone before induction of anesthesia, and 50mg every 8hours for 24 hours. Taper dose by half per day to maintenance level. New Search Contents Feedback
Licensed to University of California - SF
SupportTag: [web008-64.54.54.65-D7F19E7B56-1487]
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
●Perspectives on the Integration of Music Informatics, Performance and Aesthetics● Room C113, Aalborg University Esbjerg, Niels Bohrs Vej 8, 6700 Esbjerg, Denmark ● 12:30-13:00 The Universatory: A Presentation. Jens Arnspang, Professor, Medialogy, Aalborg University Esbjerg ● 13:00-13:30 Presentation of (1) The Research Program The Aesthetics of Music and Sound - Cro
Tumour M2-pyruvate kinase: a gastrointestinal cancer markerYogesh Kumar, Niteen Tapuria, Naveed Kirmani and Brian R. DavidsonBackground Gastrointestinal cancer tumour markers areethylenediaminetetraacetic acid (EDTA) plasma tumourvaluable in the detection of recurrence following resectionM2-pyruvate kinase were analysed together as a smallor in monitoring response to chemotherapy. CEA, CA19-9
 http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
Licensed to University of California - SF
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
Licensed to University of California - SF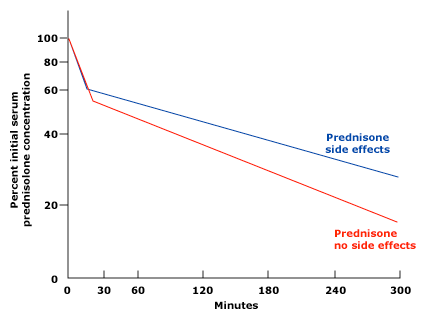 http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
Disappearance curves of tritiated prednisolone in five patients whodid not develop side effects while taking prednisone and in eightwho did. The patients who developed side effects clearedprednisolone from the circulation more slowly. Data fromKozower, M, Veatch, L, Kaplan, MM, J Clin Endocrinol Metab 1974;38:407.
Corticosteroid preparations
http://www.utdol.com/utd/content/topic.do?topicKey=adrenal/21421&view=print
Disappearance curves of tritiated prednisolone in five patients whodid not develop side effects while taking prednisone and in eightwho did. The patients who developed side effects clearedprednisolone from the circulation more slowly. Data fromKozower, M, Veatch, L, Kaplan, MM, J Clin Endocrinol Metab 1974;38:407.
Corticosteroid preparations