Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Improving bph symptoms and sexual dysfunctions with a saw palmetto preparation? results from a pilot trial
PHYTOTHERAPY RESEARCHPhytother. Res. (2012)Published online in Wiley Online Library(wileyonlinelibrary.com) DOI: 10.1002/ptr.4696
Improving BPH symptoms and sexualdysfunctions with a saw palmetto preparation?Results from a pilot trial
Andreas Suter,1,4* Reinhard Saller,2 Eugen Riedi3 and Michael Heinrich41Medical Department, A. Vogel Bioforce AG, Roggwil, Switzerland2Institute of Natural Medicine, Zurich University Hospital, Zurich, Switzerland3Urological practice, Chur, Switzerland4School of Pharmacy, University of London, University College London, London, United Kingdom
In elderly men, benign prostatic hyperplasia (BPH) is a major risk factor for sexual dysfunctions (SDys). Additionally, the standard treatments for BPH symptoms, alpha blockers and 5-alpha-reductase inhibitors, causeSDys themselves. Preparations from saw palmetto berries are an efficacious and well-tolerated symptomatictreatment for mild to moderate BPH and have traditionally been used to treat SDys. We conducted an openmulticentric clinical pilot trial to investigate whether the saw palmetto berry preparation ProstasanW influencedBPH symptoms and SDys. Eighty-two patients participated in the 8-week trial, taking one capsule of 320 mg sawpalmetto extract daily. At the end of the treatment, the International Prostate Symptom Score was reduced from14.4 Æ 4.7 to 6.9 Æ 5.2 (p < 0.0001); SDys measured with the brief Sexual Function Inventory improved from22.4 Æ 7.2 to 31.4 Æ 9.2 (p < 0.0001), and the Urolife BPH QoL-9 total improved from 162.7 Æ 47.9 to105.0 Æ 56.3 (p < 0.0001). Investigators’ and patients’ assessments confirmed the good efficacy, and treatmentwas very well tolerated and accepted by the patients. Correlation analyses confirmed the relationship betweenimproved BPH symptoms and reduced SDys. This was the first trial with saw palmetto to show improvementin BPH symptoms and SDys as well. Copyright 2012 John Wiley & Sons, Ltd.
Keywords: benign prostatic hyperplasia; sexual dysfunctions; clinical trial; saw palmetto; Serenoa repens.
and clinically significant association between LUTS and
various types of sexual dysfunctions in ageing menworldwide. From epidemiological data, Rosen et al.
The prostate is a fibromuscular glandular organ that lies
(2005) concluded that, compared with patients without
between the urinary bladder and the pelvic floor and
BPH-symptoms, patients with BPH-symptoms were at
surrounds the prostatic urethra (Dixon, 2005). Starting
a 3.7-fold higher risk of developing erectile dysfunction
around the age of 40, the prostatic tissue enclosing the
during the 2-year period following the onset of BPH-
urethra starts growing; this nonmalignant growth is
symptoms. Additionally, the severity of the LUTS
known as benign prostate hyperplasia (BPH) (Isaacs
symptoms was correlated with more frequent and more
and Coffey, 1989). It leads to constriction of the
severe occurrence of erectile and ejaculatory dysfunctions
urethra and gives rise to associated lower urinary tract
symptoms (LUTS), such as urgency, frequency, noc-
The main medical treatments for BPH symptoms
turia, incomplete bladder emptying and weak urine
include alpha blockers such as tamsulosin, doxazosin
stream. LUTS occur in about one third of all men in
and alfuzosin (Novara et al., 2006) that provide fast
their 60s and half of men older than 80 (McVary,
relief of the LUTS symptoms (Kaplan, 2004) or the
2006), even though the histological presence of BPH is
5-alpha-reductase-inhibitors finasteride and dutasteride,
observed in more than 90% of men in this age group
which lead to symptom relief after 6–9 months and are
most favourable in patients with large prostates (Dull
In addition to obstructive and irritative symptoms,
et al., 2002). Both treatment options show beneficial
BPH also negatively influences sexual functions (Gur
effects on the BPH symptoms; however, they also each
et al., 2008). Epidemiological studies show that, along
have a significant negative impact on sexual functions.
with the general ageing process, BPH-related LUTS
The main sexual dysfunction reported under alpha
are a key factor in development of erectile dysfunctions
blocker therapy is retrograde or abnormal ejaculation,
and ejaculatory disorders (Braun et al., 2003; Boyle
which occurs in 4–18% of patients taking tamsulosin, with
et al., 2004), representing a stronger risk factor than
rise to 30% during long-term use (Carbone and Hodges,
diabetes, hypertension, heart disease or hyperlipidemia
2003). Studies on 5-alpha-reductase inhibitors report
(Rosen et al., 2003). Overall, there appears to be a clear
sexual dysfunctions with a frequency of 2.1–38%,with erectile dysfunctions being most prominent, followedby decreased libido and ejaculatory disorders (Erdemir
* Correspondence to: Andreas Suter, A. Vogel Bioforce AG, MedicalDepartment, Roggwil, Switzerland.
et al., 2008). Sexual dysfunctions are the most
often reported adverse events under 5-alpha-reductase-
Copyright 2012 John Wiley & Sons, Ltd.
inhibition, with similar frequencies reported for finasteride
willingness to honestly answer questions on sexuality
and dutasteride (Naslund and Miner, 2007).
and written informed consent given by the patient.
Preparations made from the berries of saw palmetto
Exclusion criteria included lack of libido because of a
Serenoa repens (W. Bartram) Small (synonym Sabal
psychiatric disease or a depressive mood, occurrence of
serrulata (Michx.) Schult.f.) have a long standing use in
lack of libido in the judgement of the investigator within
the treatment of mild to moderate BPH symptoms.
the last 2 months, patients with severe vascular disorders
The plant, which is indigenous to Florida, was first used
(microangiopathies), severe diabetes mellitus, patients
by white settlers in the United States not only for treat-
with hypertension who were on a stable antihypertensive
ment of LUTS but, interestingly, also as a treatment for
medication for less than 2 months, known neuropathies,
erectile dysfunctions, to improve testicular atrophy and
known poor compliance of the patient, participation in
sperm production, and as a genitourinary and sexual
a clinical trial within the last 2 months prior to the study
stimulant (Bennett and Hicklin, 1998). More than 30
start, alcohol and drug abuse and planned surgeries
controlled clinical trials have been conducted to investi-
within the observation period. The participants were
gate BPH treatment with saw palmetto preparations,
prohibited from regular application (>1 unit/2 weeks) of
which generally consist of 320 mg lipophilic berry
phosphodiesterase-5-phosphodiesterase-5-inhibitors (PDE)
extract per day (Ulbricht et al., 2006). Compared with
inhibitors and intake of PDE-5-inhibitors less than 4 days
placebo, the studies demonstrate good efficacy of long-
prior to the first study visit. If not taken continuously for
term saw palmetto use to treat BPH symptoms; the
3 months as stable medication, the following concomitant
results are similar to finasteride (Carraro et al., 1996)
medications were also not allowed: 5-alpha-reductase in-
and tamsulosin (Debruyne et al., 2004), but saw
hibitors, alpha-antagonists, nonsteroidal anti-inflammatory
palmetto has a much better safety profile than these
drugs (NSAIDs) (synthetics and phytochemicals), para-
substances particularly in regards to sexual dysfunctions
cetamol and synthetic antidepressive agents.
(Wilt et al., 2002). As modes of action, in vitro andin vivo inhibition of both isoforms of the 5-alpha-reductase (Habib et al., 2005; Abe et al., 2009) and
anti-inflammatory activities (Breu et al., 1992; Iglesias-Gato et al., 2011) have been reported, as well as
This was an open clinical trial with total study duration
inhibition of autonomous receptors in the lower urinary
of 9 weeks per patient, which consisted of a 1-week
untreated run-in phase and a subsequent treatment
It is very desirable to find a treatment that not only
period of 8 weeks. At each visit, efficacy parameters
improves the symptoms of BPH but also has no negative
were recorded as detailed in the succeeding text. The
or possibly even a beneficial impact on sexual dysfunctions
run-in phase was carried out to observe if BPH
(Skolarus and Wei, 2009). With this as a goal, we carried
symptoms and sexual dysfunctions remained stable.
out a clinical pilot trial investigating whether a standar-
The test medication was a lipophilic saw palmetto berry
dized saw palmetto product influenced sexual dysfunctions
extract with a daily dosage of one capsule, containing
in patients with mild to moderate BPH.
320 mg extract (ProstasanW, batch nr. 025070, drugextractant ratio 9–12 : 1, extractant ethanol 96% V/V;manufactured by A. Vogel Bioforce AG, Roggwil,Switzerland. The berries are from A. Vogel Bioforce’sown organic certified cultivation in Florida, USA.) The
extract complied with the provisions of the EuropeanPharmacopoeia for saw palmetto fruit. One capsule of
this batch contained 275 mg fatty acids, which comprisedof 29.5% lauric acid, 39.2% oleic and linoleic acid,
The study was carried out between June 2009 and
13.5% myristic acid and 10% palmitic acid.
October 2010 in two urological and four general
At the second visit, each patient received one bottle
practices in Switzerland, in patients with at least moder-
with 90 capsules and compliance was checked by count-
ate BPH symptoms and sexual dysfunctions, such as
ing the remaining tablets at the final study visit.
erectile dysfunctions or lack of drive. The trial was
Changes in BPH symptoms were evaluated using the
approved by the relevant cantonal ethical committees
IPSS, sexual dysfunctions with the bSFI and the Urolife
and was carried out in accordance with the provisions
BPH Quality of Life-9 (Urolife QoL-9) questionnaire.
of good clinical practice and the ethical obligations of
The bSFI is a validated instrument with two questions
the Declaration of Helsinki. The Swiss regulatory
about sexual drive, three on erections, two on ejacula-
authority Swissmedic notified the study that is registered
tion, four on problem assessment and one question on
in the international clinical trial registry ClinicalTrials.
the overall satisfaction. Each question is rated on a
gov, identifier number NCT01021267.
corresponding scale from 0 (most severe problem) to 4
Inclusion criteria were as follows: male patients
(no problem) (O’Leary et al., 1995). The Urolife QoL-9
between 18–80 years of age with International Prostate
questionnaire is also a validated score with one question
Symptom Score (IPSS) >7, presence of BPH symptoms
each on desire, erection and satisfaction; each is rated on
for at least 2 months, patients suffering from sexual
a 100 mm visual analogue scale, ranging from 0 (most
dysfunction (erectile dysfunction and/or decrease of
severe problem) to 100 (no problem at all) (Lukacs
libido) for at least 2 months, sexual drive component
et al., 1997). Two questionnaires were used instead of
of the brief Sexual Function Inventory (bSFI) <5,
only one to achieve a better validity of changes in sexual
desire and possibility of sexual activity (masturbation,
dysfunctions. No validated German version was avail-
sexual partnership), no organic impairment preventing
able for either questionnaire, and thus they were first
sexual practice (physical or vascular impairment, etc.),
translated to German by two independent translators.
Copyright 2012 John Wiley & Sons, Ltd.
SAW PALMETTO IN BPH AND SEXUAL DYSFUNCTIONS
From these two translated versions, one German version
Table 1. Demographic baseline characteristics of the per protocol
was compiled, which was then re-translated to English by
two other translators, to be compared with the originalversion. The German version was then corrected and
used by a German speaking doctor in his daily practice.
Based on his experiences, further corrections were
made, and final versions of the German scores were
completed. At end of the treatment, global assessment
of efficacy by the patient and the investigator was given
on a 4-point scale (very good, good, moderate or bad).
Safety parameters included the occurrence of adverse
events and the global assessment of safety by the patient
and the investigator at the end of the treatment as very
good, good, moderate or poor. Additionally, questions
were asked about the patients’ daily routines. The
patients were asked if they would take the medication
again, how important it was for them to use herbaltreatment, and whether they would prefer a herbal remedy
during the treatment period was assessed as good when
over a synthetic compound. Investigators were asked
80–120% of the test medication was taken; 78.6% of the
if they would use the test medication again and were
patients fulfilled this criterion, only 7.1% of the patients
asked to provide reasons if they answered affirmatively.
took less than 80% of the medication.
As this was an open clinical pilot trial, descriptive statistics
There were no significant differences between the
were used using Excel (Microsoft Corporation, Redmond,
intention to treat population and the per protocol popu-
Washington, USA) and SAS Version 9.2 (SAS Institute,
lation in all parameters; therefore, the results of per
Enhanced Logging Facilities, Cary, NC, USA). For the
protocol population will be shown. There were also no
outcome measures, IPSS, bSFI and Urolife QoL, within
statistical changes in the efficacy parameters during the
group comparisons of changes from visit 1 to visit 2, from
time period without treatment (between visit 1 and visit
visit 1 to visit 3, and from visit 2 to visit 3, were performed
2), showing that the symptoms were stable and did not
using the Wilcoxon test for paired differences. Correla-
alter within a short time frame; thus, only results from
tions between changes in IPSS and bSFI, IPSS and Urolife
visit 2 (the start of treatment) and visit 3 (the end of
QoL-9, and bSFI and Urolife QoL-9 were analysed by
calculating Pearson’s coefficient of correlation.
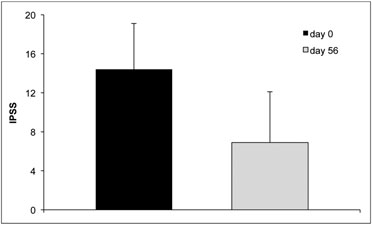
The IPSS was reduced by 51%, from 14.4 Æ 4.7 to6.9 Æ 5.2, after 8 weeks of treatment (p < 0.0001) (Fig. 1).
A score from 0 to 7 is defined as mild, from 8 to 19 as
moderate and from 20 to 35 as severe BPH symptoms.
A total of 82 patients were recruited, forming the
At the beginning of the treatment, 18.8% of all patients
intention-to-treat population. Thirteen patients had at
had severe and 78.3% had moderate symptoms; by the
least one major protocol deviation and were excluded
final visit, this shifted to 63.8% patients with mild, 31.9%
from the per protocol population, which was used for
with moderate, and only 4.3% with severe symptoms.
final analysis. Deviations included one patient with IPSS
Looking at the single items contributing to the score,
<7 at inclusion, one with sexual drive component of
they were all significantly improved to the same extent,
bSFI >5 at inclusion, four patients with disallowedconcomitant medication and seven patients who didnot return to the participating practice after the firstvisit. Reasons for discontinuation of treatment includedone instance of the death of a patient’s wife, two adverseevents (nausea that was seen as related to the studymedication and an unrelated transient ischemic attack)and in four cases the patients did not show up at all tothe follow-up visits. The patients were 57.3 Æ 11.1 yearsold and baseline characteristics as well as the agedistribution in the population were without pathological
findings. Details are shown in Table 1.
One centre recruited the majority of the patients
(n = 54), and the other five centres the remaining 15patients. The baseline characteristics of the patients
Figure 1. Change of International Prostate Symptom Score (IPSS)
from this one centre did not differ significantly
between the start and the end of treatment (per protocol population,
from those that form the other centres. Compliance
Copyright 2012 John Wiley & Sons, Ltd.
and none was superior to another. The average nycturia
the single centre experienced at least some improve-
score changed from 1.7 Æ 1.1 to 1.0 Æ 0.8, the obstructive
subscore from 8.1 Æ to 3.9 to 3.7 Æ 3.7, and the irritativesubscore from 6.3 Æ 2.6 to 3.2 Æ 2.3.
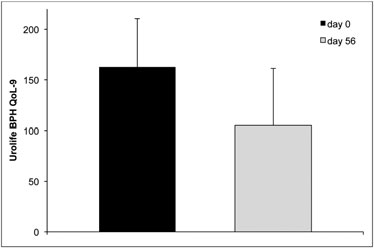
The Urolife QoL-9 total score saw an improvement
from 162.7 Æ 47.9 to 105.0 Æ 56.3 (p < 0.0001) (Fig. 3). Contrary to the bSFI, the improvements in QoL-9 were
The total bSFI score improved from 22.4 Æ 7.2 to
significant at all centres. All three single questions were
31.4 Æ 9.2 (p < 0.0001) (Fig. 2). The single item scores
also statistically significantly improved, as detailed in
for sexual drive, erectile function, ejaculatory function,
problem assessment and sexual satisfaction were eachalso significantly improved (p < 0.0001) (Table 2). Thebiggest relative improvements in single questions wereseen in the problem assessment domain, where ‘getting
Assessments by investigators and patients
and keeping an erection’ improved by 64%, and ‘havingproblems with lack of drive’ and ‘ejaculation’ each
The majority of the patients rated the efficacy as
improved by 54%. ‘Feeling sexual drive within the last
very good (22%) or good (54%) and only 15% saw a
30 days’ improved by 47%, and ‘having an erection firm
small effect. The investigators assessed efficacy more
enough to have sexual intercourse’ was scored as 42%
favourably, reporting 38% of the cases as being very
better, which, in absolute values, is a change from below
good, 44% good and only 7% patients with unchanged
‘fairly often’ to ‘usually’.
condition. When asked on what parameters the study
There was a centre effect, as mean values of the
medication had the best effect, 8% of the patients indi-
centre with the most patients exhibited a significant
cated erectile function, 26% libido and 66% erectile
improvement, whereas the other 15 patients pooled
together from the other centres only exhibited a trend
Of the total 82 patients, 62 patients would take the
(p = 0.12). Of these 15 patients, eight saw an improve-
capsules again (data are missing from six patients); and
ment, four no change and three a worsening of their
in 91% of all cases, the investigators would use the
state, whereas the vast majority of the patients from
Figure 2. Improvement of brief Sexual Function Inventory (bSFI) at
Figure 3. Improvement of the Urolife benign prostate hyperplasia
the start and the end of therapy (per protocol population, n = 69;
(BPH) quality of life-9 (QoL-9) total score between the start and
the end of therapy (per protocol population, n = 69; p < 0.0001).
Table 2. Single item scores of the bSFI and Urolife BPH QoL
BPH, benign prostate hyperplasia; bSFI, brief sexual function inventory.
Copyright 2012 John Wiley & Sons, Ltd.
SAW PALMETTO IN BPH AND SEXUAL DYSFUNCTIONS
Similarly, investigators regarded tolerability in 90.8%of the cases as very good and 5.3% as good.
In this pilot trial, we wanted to assess if a saw palmettoberry preparation had an influence on both, prostatesymptoms and sexual dysfunctions. We first examinedthe improvement in BPH symptoms as measured withthe IPSS, which is the standard instrument to measureseverity of BPH symptoms (Simpson, 1997). Weobserved a greater than 50% reduction, indicating agood treatment response that was in the efficacy rangeobserved for saw palmetto treatments in other trials on
Figure 4. Single item scores of the brief Sexual Function Inventory
BPH and larger than the effect of placebo. A survey of
(bSFI) at the start and the end of treatment, normalized to a scale
seven clinical trials for a lipophilic saw palmetto prepar-
of 0–10 (0 = worst state, 10 = best) (n = 69).
ation describes the observation of a total of 2555patients that were observed with average treatment
For 61% of the patients, it was very important that
duration of 300 days and a mean initial IPSS value of
the medication was of herbal origin and 97% of them
14.72. At the end of the treatment, IPSS was reduced
would, given the same efficacy and safety, prefer herbal
to a synthetic drug. Investigators stated that the most
clinical trials, 320 mg lipophilic saw palmetto berry
important reason to apply this saw palmetto preparation
extract was used daily and, after 6 months, the IPSS
was the good safety observed in 95% of all cases,
followed by the efficacy observed in 93% of patients.
(Bauer et al., 1999) with respective reductions underplacebo of 13.9% and 13.6%.
Secondly and more importantly, we assessed whether
the treatment had a positive influence on concomitantsexual dysfunctions. Four previous clinical trials of saw
We carried out correlation analyses to assess if changes
palmetto treatment for BPH also evaluated changes in
in IPSS, bSFI and Urolife QoL-9 were associated. There
sexual dysfunctions as a secondary parameter, with
was a negative correlation between changes in the IPSS
mixed results. However, the patients in these trials had
score and the bSFI (Pearson’s rho = À0.366; p = 0.002)
mainly BPH symptoms, not necessarily sexual dysfunc-
and a positive correlation between changes in the IPSS
tions (SDys) as well. Using the International Index of
Erectile Function (IIEF), Willetts et al. (2003) observed
p = 0.002), indicating that less urinary problems were
a trend of improvement, with an increase from 51.5 to
associated with better assessment of sexual function.
55.1 after 12 weeks of saw palmetto treatment compared
Furthermore, there was a high negative correlation
with a small decrease from 49.4 to 48.7 with placebo
between the bSFI and Urolife QoL-9, showing that both
(Willetts et al., 2003), and Sinescu et al. (2011) reported
questionnaires were valid for evaluating sexual dysfunc-
a significant improvement of the IIEF from 44.4 to 50.8
tions and consequently assessed changes to the same
after 24 months of treatment (Sinescu et al., 2011). In the
degree (Pearson’s rho = À0.607; p < 0.0001).
trial conducted by Gerber et al. (2001), the patients had
Subgroup analyses confirmed these findings, showing
to fill out a non-specified ‘sexual function question-
that patients with a higher IPSS at inclusion (IPSS 20–35)
naire’; results indicated no change with either placebo
exhibited better improvements in their bSFI (p = 0.029)
or saw palmetto treatment (Gerber et al., 2001). In an
and in their Urolife QoL-9 (p = 0.032) values than did
open trial, Bauer et al. (1999) asked if the treatment
patients with lower IPSS (8–19). Comparing younger
had an influence on patients ‘sexual activity’; responses
patients (21–50 years) to older patients (51–80 years) did
indicated that it mostly remained unchanged with two
not show a significant difference regarding changes of
patients reporting an increase (Bauer et al., 1999).
IPSS, bSFI and Urolife QoL-9, or did concomitant
Taken together, data from these trials are insufficient
medication have an influence on these parameters.
to convincingly show that saw palmetto had a positiveinfluence on BPH-related SDys.
To determine this, it was important to confirm at
inclusion that the patients in our trial definitely sufferedfrom SDys; all the patients in our trial had obvious
Five patients reported six adverse events, including
SDys, based on comparisons of the initial values from
nausea, eructation and acid regurgitation, all of which
the bSFI and the Urolife QoL-9 in our trial with
were mild in nature and seen as related to the study
epidemiological. O’Leary et al. (2003) observed an
medication, and two incidents of a transient ischemic
average total bSFI score of 27.7 in a population of
attack in the same patient and a mild pruritus, which
1883, >50-year-old men in the United States (O’Leary
were not related to the study medication. From the total
et al., 2003), whereas in our study the same age group
82 patients, data from six patients were missing on the
had a lower initial value of 20.1. In another study, the
safety assessment; from the remaining patients, 89.5%
patients with ages of 36.9 Æ 12.0 years displayed an
rated tolerability as very good and 6.6% as good.
average total bSFI of 33.5 Æ 2.2 (Collins et al., 2002)
Copyright 2012 John Wiley & Sons, Ltd.
compared with the total initial bSFI of 26.3 Æ 6.6
from 24.9 to 27.14, and subdomains for erection and
observed in our 21–50-year-old patients. A large study
satisfaction did not change significantly (Kim et al.,
of 2829 LUTS patients with an average age of 65.9 years
2010). In a large open trial with 839 enrolled patients
evaluated Urolife QoL-9 scores and found an initial total
suffering from LUTS caused by BPH, 10 mg alfuzosin
value of 8.8 Æ 0.1 (scale 0–30) (Lukacs et al., 2000),
was taken daily for 2 years. The initial IPSS of 15.5 was
whereas in our study an initial score of 170.3 Æ 47.0 (scale
reduced by 7 points, whereas the total initial bSFI value
0–300) was recorded for the 51–80 year patient group.
of 21.5 improved only slightly during the treatment
period, leading to the assessment by the authors that
success regarding improvement of SDys in this
the treatment at least ‘did not have any deleterious
study population. Both scores for SDys changed sig-
effect on sexual dysfunctions’ (Elhilali et al., 2006). A
nificantly, the bSFI by 40.2% and the Urolife QoL-9
further open clinical trial with 10 mg alfuzosin showed,
by 35.5%. Looking at the subscores, ‘sexual drive’
besides a significant improvement of the IPSS after
and ‘erectile function’, almost the same degree of
1 year of treatment, a significant improvement of the
improvement was seen for both scores, with 35.3%
bother score of the Danish Prostatic Symptom Score
and 37% in the bSFI and 33.9% and 36.7% in the
questionnaire for sexual dysfunction (van Moorselaar
Urolife QoL-9, respectively. The major difference
et al., 2005) whereas a study comparing tamsulosin/
between these two scores is caused by the more
solifenacin either alone or in combination in patients
weighted problem assessment domain of the bSFI. It
with LUTS also saw improved IPSS, but observed no
has been shown that both questionnaires are equally
significant changes in the IIEF (Seo et al., 2011). The
sensitive in assessing sexual dysfunctions, which was
IPSS reductions of about 6 to 7 points found in these
also substantiated by the correlation analysis. Inter-
studies with alpha-blockers were similar to those
estingly, we observed that it was almost impossible
observed in placebo-controlled trials (van Kerrebroeck
for patients to fill out the bSFI without doctor’s help,
et al., 2000; Nordling, 2005), but were not superior to
whereas the Urolife QoL-9 was quite easy for
the improvements in IPSS seen in our study. This is in
patients to fill out alone. In summary, we have shown
line with the trials of Debruyne et al. (2004) and Zlotta
for the first time that a saw palmetto intervention in
et al. (2005), which showed similar IPSS reductions
patients with BPH and SDys had a beneficial influ-
following treatment with a saw palmetto preparation
ence on both BPH symptoms and on SDys.
and tamsulosin (Debruyne et al., 2004; Zlotta et al.,
Our efficacy results are of further importance when
2005). The main difference between our results
considering the other available options for simultaneous
and those of the cited studies on alpha blockers is
treatment of LUTS and SDys. It is currently debated
that patients under saw palmetto treatment may
whether alpha blockers or PDE inhibitors may be
experience an improvement in their SDys, whereas
beneficial for treating symptoms of both disorders.
this effect cannot be expected from alpha-blocking
Experimental models have shown that a1-adrenergic
agents may improve erectile dysfunctions by influencing
It also remains doubtful whether PDE-5 inhibitors
the balance between contraction and relaxation of the
are a good treatment for both LUTS and SDys
corpus cavernosum smooth muscle, of which, relaxation
together. Clinical data for PDE-5 inhibitors has shown
leads to an erection (Hellstrom and Kendirci, 2006). On
a good improvement on erectile dysfunctions, but a
the other hand, experimental data also indicates that
small effect on BPH symptoms. McVary et al. (2007)
NO synthase and NO could play important roles in
saw a significant improvement in the IPSS following
tissue from the urethra, corpus cavernosum, prostate,
12 weeks of treatment with 100 mg sildenafil, with an
vas deferens and bladder neck (Ehren et al., 1994).
IPSS change of À6.3 versus À1.9 with placebo, as well
Reduced concentrations of NOS/NO in the prostate
as a significant improvement of the IIEF erectile func-
and bladder increase smooth muscle tone and may
tion domain (McVary et al., 2007). In the trial of
improve prostatic cell proliferation (Mirone et al., 2011),
Roehrborn et al. (2008), the application of different
indicating that PDE-5-inhibitors, which increase the NO
dosages of tadalafil demonstrated that an increased
concentration, may have positive effects on LUTS.
dosage correlated with increased IPSS improvement,
Initial clinical trials have been carried out with alpha
from +3.9 at 2.5 mg to +5.2 at 20 mg, with a dose of
blockers or PDE-5-inhibitors (Kaminetsky, 2006).
5 mg showing the best benefit/risk ratio. After the
Clinical data with alpha blockers, however, has shown
treatment period of 12 weeks, improvement was also seen
a good treatment effect on BPH symptoms but only a
in the IIEF erectile function subdomain (Roehrborn et al.,
small positive influence on SDys. In a clinical trial where
2008). Vardenafil (20 mg) taken twice daily for 8 weeks
patients with moderate to severe BPH symptoms took
improved the IPSS by 5.9 points, compared with
10 mg alfuzosin for 6 months, the IPSS decreased from
placebo with 3.6 points; significant changes were also
18.93 to 9.59 points, and the Male Sexual Health
seen in the IIEF erectile dysfunction (ED), and the
Questionnaire (MSHQ) ejaculation subscore improved
Urolife QoL-9 improved by 27% compared with 7%
from 23.09 to 21.54; this was statistically significant, but
under placebo (Stief et al., 2008). Although IPSS was
the clinical relevance remains doubtful with an improve-
improved in these trials, interestingly, changes in flow
ment only of about 7%. The overall number of patients
rates were never reported. In total, clinical data for
with moderate to severe erectile dysfunctions decreased
PDE-5-inhibitors show a smaller improvement in LUTS
from 35% to 22% (Leungwattanakij et al., 2010). These
than that observed in our trial following saw palmetto
results were not confirmed in another trial where
treatment, and our trial demonstrates better effects on
patients with BPH symptoms took 10 mg alfuzosin daily
ED. Interestingly, when assessing a broader spectrum
for 12 weeks. Results of this trial showed that IPSS
of SDys, as with the Urolife QoL-9 and not ED alone,
decreased significantly from 17.92 to 12.07, but the
the results of our trials are at least comparable with
MSHQ ejaculatory subdomain worsened significantly
Copyright 2012 John Wiley & Sons, Ltd.
SAW PALMETTO IN BPH AND SEXUAL DYSFUNCTIONS
One solution that has been discussed in the litera-
Association guideline for treatment of BPH symp-
ture for concomitant reduction of BPH symptoms
toms also advocates using a combination of alpha-
and ED is the combination of an alpha blocker with
blockers and 5-alpha-reductase inhibitors (McVary
a PDE-5-inhibitor. Data from three such clinical
et al., 2011), a protocol designed to achieve better
studies are presently available. One small trial inves-
efficacy, but without fully considering the additive
tigated alfuzosin, sildenafil or the combination on
side effect rates of these two drugs as shown in
LUTS and EDs. After 12 weeks of treatment, initial
combination trials (Mirone et al., 2011).
values of IPSS, which were between 16.9 and 17.8,
Our present trial has some limitations; it was
were reduced significantly in all treatment groups
designed as an uncontrolled pilot trial to elucidate if
with the largest reduction (24.1%) in the combination
any effect of a saw palmetto treatment would be
group. The IIEF erectile function score was signifi-
observed. Consequently, the size of the placebo effect
cantly improved by the combination and sildenafil,
can only be estimated. Furthermore, there was a
but not in the alfuzosin group (Kaplan et al., 2007).
strong centre effect, as one centre recruited substan-
Another combination trial with sildenafil or tamsulosin
tially more patients than the others, and these other
showed comparable results, with the largest IPSS
centres did have fewer responders than the main
improvement observed with the combination (À40.1%),
centre. Subgroup analysis did not unveil any significant
differences in patient characteristics between these
(À28.2%); the IIEF improved significantly with
centres; however, these analyses were limited by the
sildenafil and the combination but not with tamsulosin
low number of patients in the other five centres to-
(Tuncel et al., 2010). In further trial, 100 mg udenafil
gether. A further placebo-controlled clinical trial with
was added to a stable alpha-blocking therapy in
a more balanced patient distribution in the centres
patients with BPH and ED for 8 weeks. The IPSS was
would be the next step to confirm our findings.
reduced by 2.8 points, and the IIEF-5 improved bymore than 5 points, indicating that a combination oradd-on therapy of udenafil may be beneficial (Chunget al., 2009). Comparing these data with the results
of our trial, with an IPSS-reduction of 51% andimproved SDys by 40.1% as measured with the bSFI,
This is the first trial ever to indicate that saw palmetto
the saw palmetto treatment yielded efficacy results similar
treatment had not only a good efficacy in reducing
to the combination of an alpha blocker and a PDE-5-
BPH symptoms but also a concomitant effect on SDys.
We demonstrated that a saw palmetto treatment was
Phosphodiesterase-5-inhibitors are expensive treat-
as effective in reducing BPH symptoms as an alpha
ments; therefore, a cost-benefit assessment is warranted
blocker or a 5-alpha-reductase inhibitor, but that, in
for further extensive PDE-prescription. In the USA, a
contrast to those treatments, saw palmetto was asso-
single dose of 25 mg sildenafil costs about eight times
ciated with an improvement of SDys as measured with
as much as an alpha-blocking agent like 1 mg doxazosin
the bSFI and the Urolife QoL-9 score. Compared with
(Stafford and Radley, 2002) or 30 times more than
PDE-5-inhibitors, the saw palmetto treatment did not
0.4 mg tamsulosin in Germany (Schneider and Richling,
have the same efficacy in improving ED, but did have
2008), whereas the cost for a daily dosage of Prostasan
the same treatment effect for overall change of SDys,
is in the lower range of an alpha blocker. These differ-
with a better reduction in IPSS. The cost of daily treat-
ences in price, in addition to the only moderate effi-
ment with saw palmetto is much cheaper than with many
cacy, make it doubtful if PDE-5-inhibitors should be
other medications, for example, in Switzerland, the cost
advocated as standard treatments for BPH symptoms.
would be 0.75 Swiss francs for saw palmetto versus
When looking at safety and tolerability, our data
22.30 Swiss francs for 100 mg sildenafil (Stebler, 2009).
were in accordance with the previous findings and
In our trial, we observed the same efficacy results as have
indicated that saw palmetto was very well tolerated,
been seen for combination therapy with alpha blocker
in contrast to the standard treatments for LUTS. A
and PDE-5-inhibitor, but with much better tolerability
major problem for patients taking an alpha blocker
of the saw palmetto treatment. Based on these promising
and/or a 5-alpha-reductase inhibitor is the occurrence
results, which are also reflected by the good acceptance
of sexual adverse effects that cause many men to
of patients and investigators, we consider saw palmetto
discontinue treatment (Roehrborn, 2004). Study data
to be the first line treatment for patients with mild and
show that 2–16% of all patients under alpha reduc-
moderate BPH symptoms, as it may also improve con-
tase inhibitor therapy experience EDs, decreased
comitant SDys, while having a very good tolerability
libido and decreased volume of ejaculate (twice the
frequency seen with placebo), whereas alpha-blockingagents, particularly tamsulosin, have been frequentlylinked with ejaculatory disorders in around 10% of all
patients (Gacci et al., 2011). In daily practice, theincidence rates may even be higher than in clinical
We would like to thank the following investigators for participating in
trials. In a large epidemiological study carried out with
this trial: Daniel Borer, Moerigen; Eva Ditrych, Bern; Simon Feldhaus,Brunnen; Manfred Hoesle, Zurich; and Felix Trinkler, Zollikon.
urologists and internal medicine physicians in theUnited States, doctors estimated that 18–27% of thepatients taking an alpha-blocking medication suffer
from ejaculatory disorders and 16–22% of men takinga 5-alpha-reductase-inhibitor suffer from EDs (Seftel
The study was financed by A.Vogel Bioforce AG, where A. Suter is
et al., 2007). Nevertheless, the latest American Urology
Copyright 2012 John Wiley & Sons, Ltd.
Abe M, Ito Y, Oyunzul L, Oki-Fujino T, Yamada S. 2009. Pharmaco-
Iglesias-Gato D, Carsten T, Vesterlund M, Pousette A, Schoop R,
logically relevant receptor binding characteristics and 5alpha-
Norstedt G. 2011. Androgen-independent effects of Serenoa
reductase inhibitory activity of free fatty acids contained in
repens extract (Prostasan(R)) on prostatic epithelial cell prolif-
saw palmetto extract. Biol Pharm Bull 32(4): 646–650.
eration and inflammation. Phytother Res 26: 259–264.
Bauer HW, Casarosa C, Cosci M, Fratta M, Blessmann G. 1999.
Isaacs JT, Coffey DS. 1989. Etiology and disease process of
[Saw palmetto fruit extract for treatment of benign prostatic
benign prostatic hyperplasia. Prostate Suppl 2: 33–50.
hyperplasia. Results of a placebo-controlled double-blind
Kaminetsky J. 2006. Comorbid LUTS and erectile dysfunction:
study]. MMW Fortschr Med 141(25): 62.
optimizing their management. Curr Med Res Opin 22(12):
Bennett BC, Hicklin J. 1998. Uses of saw palmetto (Serenoa
repens, Arecaceae) in Florida. Econ Bot 52: 381–393.
Kaplan SA. 2004. AUA guidelines and their impact on the manage-
Berry SJ, Coffey DS, Walsh PC, Ewing LL. 1984. The development
ment of BPH: an update. Rev Urol 6(Suppl 9): S46–S52.
of human benign prostatic hyperplasia with age. J Urol
Kaplan SA, Gonzalez RR, Te AE. 2007. Combination of Alfuzosin
and sildenafil is superior to monotherapy in treating lower
Boyle P, Robertson C, Lowe F, Roehrborn C. 2004. Updated meta-
urinary tract symptoms and erectile dysfunction. Eur Urol
analysis of clinical trials of Serenoa repens extract in the
treatment of symptomatic benign prostatic hyperplasia. BJU
van Kerrebroeck P, Jardin A, Laval KU, van Cangh P. 2000. Effi-
cacy and safety of a new prolonged release formulation of
Braun MH, Sommer F, Haupt G, Mathers MJ, Reifenrath B,
alfuzosin 10 mg once daily versus alfuzosin 2.5 mg thrice daily
Engelmann UH. 2003. Lower urinary tract symptoms and
and placebo in patients with symptomatic benign prostatic
erectile dysfunction: co-morbidity or typical "aging male"
hyperplasia. ALFORTI study group. Eur Urol 37(3): 306–313.
symptoms? Results of the "cologne male survey". Eur Urol
Kim MK, Cheon J, Lee KS, et al. 2010. An open, non-comparative,
multicentre study on the impact of Alfuzosin on sexual
Breu W, Hagenlocher M, Redl K, Tittel G, Stadler F, Wagner H.
function using the male sexual health questionnaire in patients
1992. [Anti-inflammatory activity of sabal fruit extracts
with benign prostate hyperplasia. Int J Clin Pract 64(3):
prepared with supercritical carbon dioxide. In vitro antagonists
Leungwattanakij S, Watanachote D, Noppakulsatit P, et al. 2010.
Arzneimittelforschung 42(4): 547–551.
Sexuality and management of benign prostatic hyperplasia
Carbone DJ, Jr, Hodges S. 2003. Medical therapy for benign
prostatic hyperplasia: sexual dysfunction and impact on
quality of life. Int J Impot Res 15(4): 299–306.
Lukacs B, Comet D, Grange JC, Thibault P. 1997. Construction
Carraro JC, Raynaud JP, Koch G, et al. 1996. Comparison of
and validation of a short-form benign prostatic hypertrophy
phytotherapy (Permixon) with finasteride in the treatment of
health-related quality-of-life questionnaire. BPH group in
benign prostate hyperplasia: a randomized international
general practice. Br J Urol 80(5): 722–730.
study of 1,098 patients. Prostate 29(4): 231–240; discussion
Lukacs B, Grange JC, Comet D. 2000. One-year follow-up of 2829
patients with moderate to severe lower urinary tract symp-
Chung BH, Lee JY, Lee SH, Yoo SJ, Lee SW, Oh CY. 2009. Safety
toms treated with Alfuzosin in general practice according to
and efficacy of the simultaneous administration of udenafil
IPSS and a health-related quality-of-life questionnaire. BPM
and an alpha-blocker in men with erectile dysfunction con-
group in general practice. Urology 55(4): 540–546.
comitant with BPH/LUTS. Int J Impot Res 21(2): 122–128.
McVary KT. 2006. BPH: epidemiology and comorbidities. Am J
Collins S, Upshaw J, Rutchik S, Ohannessian C, Ortenberg J,
Albertsen P. 2002. Effects of circumcision on male sexual
McVary KT, Monnig W, Camps JL, Jr, Young JM, Tseng LJ, van
function: debunking a myth? J Urol 167(5): 2111–2112.
den Ende G. 2007. Sildenafil citrate improves erectile function
Debruyne F, Boyle P, Calais Da Silva F, et al. 2004. Evaluation of
and urinary symptoms in men with erectile dysfunction and
the clinical benefit of permixon and tamsulosin in severe BPH
lower urinary tract symptoms associated with benign prostatic
patients-PERMAL study subset analysis. Eur Urol 45(6):
hyperplasia: a randomized, double-blind trial. J Urol 177(3):
Dixon JS .2005. Macro-anatomy of the prostate. In Textbook of
McVary KT, Roehrborn CG, Avins AL, et al. 2011. Update on AUA
guideline on the management of benign prostatic hyperplasia.
Fitzpatrick JM, Roehrborn CG, Boyle P (eds). Taylor and
Mirone V, Sessa A, Giuliano F, Berges R, Kirby M, Moncada I.
Dull P, Reagan RW, Jr, Bahnson RR. 2002. Managing benign
2011. Current benign prostatic hyperplasia treatment: impact
prostatic hyperplasia. Am Fam Physician 66(1): 77–84.
on sexual function and management of related sexual adverse
Ehren I, Adolfsson J, Wiklund NP. 1994. Nitric oxide synthase activ-
events. Int J Clin Pract 65(9): 1005–1013.
ity in the human urogenital tract. Urol Res 22(5): 287–290.
van Moorselaar RJ, Hartung R, Emberton M, et al. 2005. Alfuzosin
Elhilali M, Emberton M, Matzkin H, et al. 2006. Long-term efficacy
10 mg once daily improves sexual function in men with lower
and safety of alfuzosin 10 mg once daily: a 2-year experience
urinary tract symptoms and concomitant sexual dysfunction.
in ’real-life’ practice. BJU Int 97(3): 513–519.
Erdemir F, Harbin A, Hellstrom WJ. 2008. 5-alpha reductase inhibi-
Naslund MJ, Miner M. 2007. A review of the clinical efficacy and
tors and erectile dysfunction: the connection. J Sex Med
safety of 5alpha-reductase inhibitors for the enlarged prostate.
Gacci M, Eardley I, Giuliano F, et al. 2011. Critical analysis of the
Nordling J. 2005. Efficacy and safety of two doses (10 and 15 mg)
relationship between sexual dysfunctions and lower urinary
of Alfuzosin or Tamsulosin (0.4 mg) once daily for treating
tract symptoms due to benign prostatic hyperplasia. Eur Urol
symptomatic benign prostatic hyperplasia. BJU Int 95(7):
Gerber GS, Kuznetsov D, Johnson BC, Burstein JD. 2001. Rando-
Novara G, Galfano A, Ficarra V, Artibani W. 2006. Anticholinergic
mized, double-blind, placebo-controlled trial of saw palmetto
drugs in patients with bladder outlet obstruction and lower
in men with lower urinary tract symptoms. Urology 58(6):
urinary tract symptoms: a systematic review. Eur Urol 50(4):
Gur S, Kadowitz PJ, Hellstrom WJ. 2008. Guide to drug therapy
O’Leary MP, Fowler FJ, Lenderking WR, et al. 1995. A brief male
for lower urinary tract symptoms in patients with benign
sexual function inventory for urology. Urology 46(5): 697–706.
prostatic obstruction: implications for sexual dysfunction.
O’Leary MP, Rhodes T, Girman CJ, et al. 2003. Distribution of the
brief male sexual inventory in community men. Int J Impot
Habib FK, Ross M, Ho CK, Lyons V, Chapman K. 2005. Serenoa
repens (Permixon) inhibits the 5alpha-reductase activity of
Roehrborn CG. 2004. Lower urinary tract symptoms, benign
human prostate cancer cell lines without interfering with PSA
prostatic hyperplasia, erectile dysfunction, and phospho-
expression. Int J Cancer 114(2): 190–194.
diesterase-5 inhibitors. Rev Urol 6(3): 121–127.
Hellstrom WJ, Kendirci M. 2006. Type 5 phosphodiesterase inhibi-
Roehrborn CG, McVary KT, Elion-Mboussa A, Viktrup L. 2008.
tors: curing erectile dysfunction. Eur Urol 49(6): 942–945.
Tadalafil administered once daily for lower urinary tract
Copyright 2012 John Wiley & Sons, Ltd.
SAW PALMETTO IN BPH AND SEXUAL DYSFUNCTIONS
symptoms secondary to benign prostatic hyperplasia: a dose
finding study. J Urol 180(4): 1228–1234.
Rosen R, Altwein J, Boyle P, et al. 2003. Lower urinary tract symp-
Stief CG, Porst H, Neuser D, Beneke M, Ulbrich E. 2008. A
toms and male sexual dysfunction: the multinational survey of
randomised, placebo-controlled study to assess the efficacy
the aging male (MSAM-7). Eur Urol 44(6): 637–649.
of twice-daily vardenafil in the treatment of lower urinary tract
Rosen RC, Giuliano F, Carson CC. 2005. Sexual dysfunction and
symptoms secondary to benign prostatic hyperplasia. Eur Urol
lower urinary tract symptoms (LUTS) associated with benign
prostatic hyperplasia (BPH). Eur Urol 47(6): 824–837.
Suzuki M, Oki T, Sugiyama T, Umegaki K, Uchida S, Yamada S.
Schneider D, Richling F. 2008. Checkliste Arzneimittel. Georg
2007. Muscarinic and alpha 1-adrenergic receptor binding
characteristics of saw palmetto extract in rat lower urinary
Seftel A, Rosen R, Kuritzky L. 2007. Physician perceptions of
sexual dysfunction related to benign prostatic hyperplasia
Tuncel A, Nalcacioglu V, Ener K, Aslan Y, Aydin O, Atan A. 2010.
(BPH) symptoms and sexual side effects related to BPH
Sildenafil citrate and tamsulosin combination is not superior to
medications. Int J Impot Res 19(4): 386–392.
monotherapy in treating lower urinary tract symptoms and
Seo DH, Kam SC, Hyun JS. 2011. Impact of lower urinary tract
erectile dysfunction. World J Urol 28(1): 17–22.
Ulbricht C, Basch E, Bent S, et al. 2006. Evidence-based system-
tamsulosin and solifenacin combination therapy on erectile
atic review of saw palmetto by the natural standard research
function. Korean J Urol 52(1): 49–54.
collaboration. J Soc Integr Oncol 4(4): 170–186.
Simpson RJ. 1997. Benign prostatic hyperplasia. Br J Gen Pract 47
Willetts KE, Clements MS, Champion S, Ehsman S, Eden JA.
2003. Serenoa repens extract for benign prostate hyperplasia:
Sinescu I, Geavlete P, Multescu R, et al. 2011. Long-term efficacy
a randomized controlled trial. BJU Int 92(3): 267–270.
of Serenoa repens treatment in patients with mild and moder-
Wilt T, Ishani A, Mac Donald R. 2002. Serenoa repens for benign
ate symptomatic benign prostatic hyperplasia. Urol Int 86(3):
prostatic hyperplasia. Cochrane Database Syst Rev CD001423.
Zlotta AR, Teillac P, Raynaud JP, Schulman CC. 2005. Evalu-
Skolarus TA, Wei JT. 2009. Measurement of benign prostatic
ation of male sexual function in patients with lower urinary
hyperplasia treatment effects on male sexual function. Int J
tract symptoms (LUTS) associated with benign prostatic
hyperplasia (BPH) treated with a phytotherapeutic agent
Stafford RS, Radley DC. 2002. The potential of pill splitting to
(Permixon), Tamsulosin or Finasteride. Eur Urol 48(2):
achieve cost savings. Am J Manag Care 8(8): 706–712.
Copyright 2012 John Wiley & Sons, Ltd.
MAGYAR NYELV ÉS IRODALOM MESTERKÉPZÉS A Miskolci Egyetem Bölcsészettudományi Kara (ME BTK) magyar szakos képzéseinek megtervezésekor alapvetően két tényezőt vettünk figyelembe: a hagyományos magyar szakos képzés jellegének megtartását, illetve az újabban jelentkező regionális és országos foglalkoztatási igényeket. A bölcsészek elhelyezkedési lehetőségeiről, esély
SURVEY ON SCHOOL-BASED MEASURES FOR IMMIGRANT CHILDREN 1. NATIONAL DEFINITIONS AND DEMOGRAPHIC CONTEXT OF IMMIGRATION 1.1. National definitions and legislative sources Immigrants in Slovenia can be classified into four categories (1): 1. Slovene citizens who immigrated to Slovenia because of the disintegration of former Yugoslavia (e.g. officers of the Yugoslav Army and their fa
 SAW PALMETTO IN BPH AND SEXUAL DYSFUNCTIONS
From these two translated versions, one German version
Table 1. Demographic baseline characteristics of the per protocol
was compiled, which was then re-translated to English by
two other translators, to be compared with the originalversion. The German version was then corrected and
used by a German speaking doctor in his daily practice.
SAW PALMETTO IN BPH AND SEXUAL DYSFUNCTIONS
From these two translated versions, one German version
Table 1. Demographic baseline characteristics of the per protocol
was compiled, which was then re-translated to English by
two other translators, to be compared with the originalversion. The German version was then corrected and
used by a German speaking doctor in his daily practice.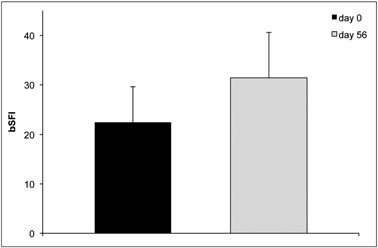
 and none was superior to another. The average nycturia
the single centre experienced at least some improve-
score changed from 1.7 Æ 1.1 to 1.0 Æ 0.8, the obstructive
subscore from 8.1 Æ to 3.9 to 3.7 Æ 3.7, and the irritativesubscore from 6.3 Æ 2.6 to 3.2 Æ 2.3.
and none was superior to another. The average nycturia
the single centre experienced at least some improve-
score changed from 1.7 Æ 1.1 to 1.0 Æ 0.8, the obstructive
subscore from 8.1 Æ to 3.9 to 3.7 Æ 3.7, and the irritativesubscore from 6.3 Æ 2.6 to 3.2 Æ 2.3.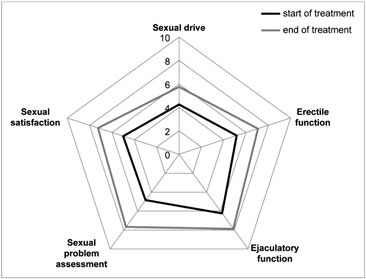 SAW PALMETTO IN BPH AND SEXUAL DYSFUNCTIONS
Similarly, investigators regarded tolerability in 90.8%of the cases as very good and 5.3% as good.
SAW PALMETTO IN BPH AND SEXUAL DYSFUNCTIONS
Similarly, investigators regarded tolerability in 90.8%of the cases as very good and 5.3% as good.