Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Navicular syndrome
NAVICULAR SYNDROME
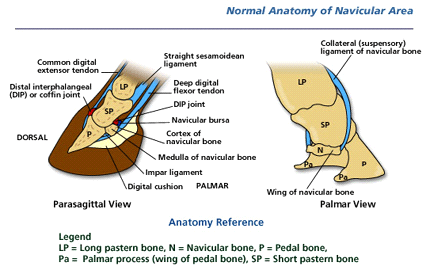
Navicular disease is really a group of related conditions affecting the navicular bone and associated structures in the foot. There are several possible causes of pain in and around the navicular bone. Anatomy of the navicular region The navicular bone is a small flattened bone, which lies across the back of the coffin joint. It attaches to the pedal (coffin) bone via a short strong ligament (the impar ligament) and to the pastern joint by suspensory ligaments. The deep digital flexor tendon runs over the lower surface of the navicular bone, which acts somewhat like a pulley and between these lies a small pocket of fluid, the navicular bursa, which acts like a cushion between the tendon and its pulley. What causes navicular disease? At present, the exact primary cause of Navicular Syndrome is not known. Damage to the navicular bone may occur due to interference with blood supply or trauma to the bone. Damage can occur to the deep flexor tendon, navicular bursa, or navicular ligaments all resulting in pain and lameness. Conformation and unbalanced trimming contribute greatly to the disease. It is somewhat inherited, either directly or in the inherited conformation of the feet that makes a horse more prone to navicular disease. What are the symptoms? Navicular disease affects the front feet of horses causing a low grade bilateral lameness, which usually progresses slowly. The lameness might only occur from time to time or when the horse is exercised on hard ground or in a small circle. In some cases, one foot is affected more than the
other, causing an obvious lameness. Affected horses may stand with the more painful foot in front placed of the other (pointing). How is navicular disease diagnosed? Diagnosis is based on a combination of history, symptoms, nerve blocks and radiography. A history of intermittent low grade or recurrent lameness is suggestive of navicular disease. Affected horses often appear to place the toe down first, as if trying not to put weight on their heels (in contrast to laminitis), and the lameness is worse on the inside leg on a circle. Injection of local anaesthetic (nerve block) around the nerves sensitizing the back half of the foot and/or into the navicular bursa will improve or alleviate the lameness associated with navicular disease. Some cases also improve when the coffin joint is blocked. Radiographs may reveal damage to the navicular bone but bone Radiograph of navicular bone showing
changes can be difficult to interpret, as there are differing
chronic change at lower boarder
opinions on what is normal. Navicular syndrome can exist without demonstrable radiographic abnormality and magnetic resonance imagining (MRI) may reveal injury to the impar or other ligaments or soft tissues. What treatments are available? Navicular disease can be treated and managed, but rarely cured. Corrective trimming and
shoeing is imperative to ensure level foot fall and foot balance. Often a rolled toe egg bar shoe is used to encourage early break over at the toe and good heel support. Medication such as phenylbutazone will elevate pain in many cases and enable work to be resumed. Long term treatment with substances such as isoxsuprine and aspirin may improve blood supply to the navicular bone and improve the condition of the bone. Long term desensitization of the back of the foot can be achieved by performing a neurectomy to cut the heel nerves. This treatment should only be considered as a last resort and then only in full recognition of the implications. Post operative complications are common and include rupture of the deep flexor tendon, painful inflammation of the cut nerve endings (neuromas) and damage to the foot which goes unnoticed by
Post mortem navicular
horse and owner. The nerves often grow back and the lameness returns
bones showing chronic
within 1-2 years of surgery. Treatment options should be discussed in
Can navicular disease be prevented? Horses with all foot shapes can develop navicular disease. Nevertheless, maintaining good foot balance and heel support can help to prevent many foot lamenesses. Prepurchase examinations can help identify affected horses before you buy them.
Daniel P. Keenan, DVM Ron McAlister, DVM Lynsey Makkreel, DVM
165 Third Street Bordentown, New Jersey 08505 609-291-0535 fax 609-291-8899
www.KeenanMcAlister.com KME@KeenanMcAlister.com
Corticoïdes inhalés : Quelle drogue ? Quel système ? Laurent Têtu, Roger Escamilla, Alain Didier Clinique des Voies Respiratoires, Hôpital Larrey, CHU de Toulouse, 31059 Toulouse Les corticoïdes inhalés et leurs effets Les glucocorticoïdes inhalés représentent le meilleur choix pour le traitement anti-inflammatoire de l’asthme. Les différents corticoïdes inhalé
in children, 74environmental control measures and, 42 Note: Page numbers in italics indicate figures. Allergic reactions. See also Inflammatory cascade. Page numbers followed by t refer to tables. Numbers preceded by CP indicate Color Plates. ABRS. See Bacterial rhinosinusitis, acute. causes of, 15t, 32-33. See also Allergens. chronic, 135. See also Rhinosinusitis, chronic. skin tes

 NAVICULAR SYNDROME
NAVICULAR SYNDROME 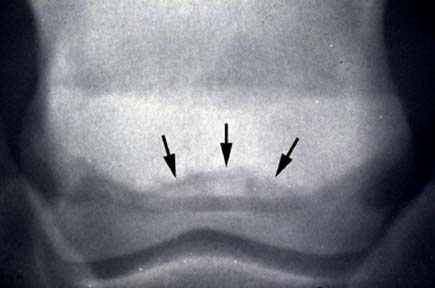
 other, causing an obvious lameness. Affected horses may stand with the more painful foot in front
other, causing an obvious lameness. Affected horses may stand with the more painful foot in front