Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Ingmarmed.com
Effect of Face Mask Design on Inhaled Mass of Nebulized Albuterol,
Hui-Ling Lin MSc RN RRT, Ruben D Restrepo MD RRT, Douglas S Gardenhire MSc RRT-NPS,
BACKGROUND: Aerosol face mask design and the distance at which the face mask is held from the face affect the delivery of nebulized medication to pediatric patients. OBJECTIVE: To measure the inhaled mass of nebulized albuterol with 3 types of pediatric face mask, at 3 different distances from the face, with a model of a spontaneously breathing infant. METHODS: We compared a standard pediatric face mask and 2 proprietary pediatric face masks (one shaped to resemble a dragon face, the other shaped to resemble a fish face). The albuterol was nebulized with a widely used jet nebulizer. Aerosol delivery with each type of mask was measured with the mask at 0 cm (ie, mask directly applied to the mannequin face), 1 cm, and 2 cm from the mannequin face. In each test the nebulizer was filled with a 3-mL unit dose of albuterol sulfate and powered by oxygen at 8 L/min, with a total nebulization time of 5 min. The mannequin face was connected to a lung simulator that simulated a spontaneously breathing infant. We measured inhaled mass by collecting the aerosol on a 2-way anesthesia filter that was attached to the back of the mannequin’s oral opening via a 15-mm silicon adapter. We also measured residual drug left in the nebulizer, and estimated the drug lost to the atmosphere. RESULTS: The mean ؎ SD inhaled percentage of the nominal dose values at 0 cm, 1 cm, and 2 cm, respectively, were 2.18 ؎ 0.53%, 1.45 ؎ 0.46%, and 0.92 ؎ 0.51% with the standard mask; 2.65 ؎ 0.55%, 1.7 ؎ 0.38%, and 1.3 ؎ 0.37% with the dragon mask; and 3.67 ؎ 0.8%, 2.92 ؎ 0.4%, and 2.26 ؎ 0.56% with the fish mask. With all 3 masks there was a statistically significant difference (p < 0.001) in inhaled mass between the 0 cm and 2 cm distance. The fish mask had a significantly higher (p < 0.001) inhaled mass than the dragon mask or the standard mask, at all 3 distances. CONCLUSIONS: The inhaled mass of albuterol is significantly reduced when the mask is moved away from the face. The fish mask had significantly higher inhaled mass than the standard mask or the dragon mask, under the conditions we studied. Mask design may affect nebulized albuterol delivery to pediatric patients. Key words: albuterol, aerosol, face mask, inhaled drug mass, pediatric, jet nebulizer. [Respir Care 2007;52(8):1021–1026. 2007 Daedalus Enterprises]
Hui-Ling Lin MSc RN RRT is affiliated with the Respiratory Care Pro-
IngMar Medical, Pittsburgh, Pennsylvania, provided the Active Servo
gram, Dakota State University, Madison, South Dakota. Ruben D Re-
Lung 5000 simulator used in this research.
strepo MD RRT is affiliated with the Department of Respiratory Care,University of Texas Health Science Center, San Antonio, Texas. DouglasS Gardenhire MSc RRT-NPS and Joseph L Rau PhD RRT FAARC are
The authors report no conflicts of interest related to the content of this paper.
affiliated with the Division of Respiratory Therapy, Georgia State Uni-versity, Atlanta, Georgia.
Correspondence: Ruben D Restrepo MD RRT, Department of Respira-
This study represents the master’s thesis research of Hui-Ling Lin MSc RN
tory Care, University of Texas Health Science Center at San Antonio,
RRT in the Division of Respiratory Therapy at Georgia State University.
7703 Floyd Curl Drive, Mail Code 6248, San Antonio TX 78229-3900.
Hui-Ling Lin MSc RN RRT presented a version of this paper at the 51st
International Respiratory Congress of the American Association for Respi-ratory Care, held December 3–6, 2005, in San Antonio, Texas, at which, forthe paper, Hui-Ling Lin MSc RN RRT was awarded a Fellowship for Aero-sol Technique Development from Monaghan Medical/Trudell.
RESPIRATORY CARE • AUGUST 2007 VOL 52 NO 8
EFFECT OF FACE MASK DESIGN ON INHALED MASS OF ALBUTEROL
Introduction
Gas-powered jet nebulizers are commonly employed to
deliver medications to patients’ airways via a mouthpieceor a face mask. Although no significant difference in clin-ical response has been found in adults between a mouth-piece and a fitted mask,1 administering nebulized medica-tion with a fitted face mask to infants and toddlers can bequite challenging. As infants grow older, they are increas-ingly aware of their surroundings and frequently becomedistressed with the application of a mask. When the childis upset, the seal between the face and the mask is easilybroken, which causes entrainment of ambient air and de-creases the quantity and the concentration of aerosol in-
Fig. 1. Configuration of equipment for simulation of pediatric breath-
ing and nebulized albuterol delivered via face mask, with the mask
An alternative technique for aerosol delivery to the pe-
at 0 cm, 1 cm, and 2 cm from the chin of the mannequin face.
diatric patient is “blow-by,” in which the clinician aims theaerosol flow toward the patient’s face instead of applying
a mask. We previously reported a 43% reduction in theinhaled dose with a 1-cm gap between the mask and the
Lung Model
inhalation hole on a mannequin face, and a 67% reduction
A model of a spontaneously breathing infant was cre-
with 2-cm gap.4 Similar data were previously found by
ated with a lung simulator (ASL [Active Servo Lung]
5000, IngMar Medical, Pittsburgh, Pennsylvania). The sim-ulator was set at a maximum muscle pressure of13.5 cm H O, a resistance of 20 cm H O/L/s, and a com-
pliance of 5 mL/cm H O, to generate a tidal volume of
60 mL. The respiratory rate was set at 20 breaths/min,inspiratory time was 0.7 s, inspiratory-expiratory ratio was1:3, and inspiratory flow was 120 mL/s.
There are several pediatric face masks available for use
A mannequin face with a 15-mm silicon adapter was
with jet nebulizers. Research on the efficiency of face
attached to the inhalation filter (a 2-way, nonconductive
masks with a metered-dose inhaler (MDI) with spacer/
anesthesia filter, model 1T0241, Baxter Healthcare, Deer-
holding chamber suggests that the choice of face mask and
field, Illinois), which collected the inhaled aerosol. A sim-
the integrity of the interface between the mask and the
ilar filter was attached to the lung simulator, for protection
child’s face is critical in determining the inhaled dose in
from inhaled aerosol, but was not used to calculate drug
children.6–11 Newly redesigned masks for MDIs allow a
better seal with the patient’s face. The pediatric face masksused with jet nebulizers have traditionally been smaller
Study Design
versions of the masks used with adults. These pediatricmasks have a considerably larger volume of potential dead
A nebulizer (Misty-Neb, Baxter Healthcare Corpora-
space and relatively large side holes, compared to adult
tion, Valencia, California) was attached to a standard face
face masks. Manufacturers have designed pediatric face
mask (Hudson RCI, Durham, North Carolina), then to a
masks in an effort to improve drug delivery to children. In
mask designed to resemble a dragon face (DragonMask,
our preliminary literature search, we found a paucity of
KidsMED, Hinsdale, Indiana), and then to a mask de-
reports on inhaled drug mass with jet nebulizers attached
signed to resemble a fish face (Bubbles the Fish, PARI
to pediatric face masks of various designs.
Respiratory Equipment, Monterey, California) (Table 1).
The purpose of the present study was to determine the
Each nebulizer was held in a vertical orientation with a
inhaled drug mass, nebulizer residual drug loss, and esti-
metal holder and a clamp to prevent error from misalignment.
mated ambient loss during delivery of nebulized albuterol
All masks were held perpendicular to the inhalation filter
to 3 brands of pediatric face mask, with the mask at 0 cm,
1 cm, and 2 cm from a mannequin face connected to a
Each trial was conducted by placing the face mask at
breathing simulator, with the breathing pattern of a spon-
0 cm (ie, the mask was in contact with the mannequin
face), 1 cm, or 2 cm from the mannequin face, measured
RESPIRATORY CARE • AUGUST 2007 VOL 52 NO 8
EFFECT OF FACE MASK DESIGN ON INHALED MASS OF ALBUTEROL
*Designed specifically for use with PARI nebulizers. †Mask volume was measured by filling the mask with water. ‡Holes on both sides.
from the lower edge of the mask to the chin of the man-
terol, after each trial the mask and the mannequin face
nequin face. Aerosol delivery with each type of mask was
were wiped with an alcohol pad, and the 15-mm silicon
To minimize variations among masks and among distances
Because of the open nature of the model (ie, because of
caused by nebulizers, we used 5 different Misty-Neb nebu-
the open space between the mask and the mannequin face),
lizers. Each nebulizer was used with all 3 mask types and at
some aerosol was lost to the ambient air, so that aerosol
all 3 distances, so each nebulizer was run a total of 9 times,
could not be collected and measured. Instead, it was cal-
in random order; thus, there were 45 separate trials.
culated by subtracting the inhaled drug mass and the dead
All the nebulizers were powered by 50 psi oxygen at
volume drug mass from the starting (nominal) dose of
8 L/min. Gas flow to the nebulizer was started immedi-
ately after the first simulator breath. Then, 100 simulated
A simple linear regression and prediction equation were
breaths were run, in 5 min; then the gas flow was termi-
developed from a known albuterol sulfate solution (Sigma,
nated in synchrony with the simulator. In each trial the
St Louis, Missouri). All drug amounts were analyzed via
nebulizer was filled with a 3.0-mL unit dose of albuterol
spectrophotometry (Beckman Instruments, Fullerton, Califor-
sulfate, which contains 2.5 mg of albuterol base.
nia), at a wavelength of 276 nm. The solvent was 0.1 normalhydrochloric acid solution. The inhalation filter was washed
Measurements
for 1 min, with gentle agitation. The spectrophotometer wascalibrated prior to trials, with a holmium oxide filter (Beck-
The inhaled drug mass was measured by extracting the
man Instruments, Fullerton, California) to determine the wave-
aerosol from the inhalation filter. In bench models, the
length accuracy, and set to zero by running the solvent alone
inhalation filter is placed in the final path of aerosol that
before each analysis. The concentration of the sample solu-
would be inhaled by a patient.12 Each nebulizer was weighed
tion and the amount of albuterol were calculated from a known
before and after filling with albuterol, and following neb-
concentration/absorbency relationship.
ulization, to determine the amount of solution remaining inthe device (dead volume). The dead volume was collectedby washing the nebulizer system components with 0.1 nor-
Statistical Analysis
mal hydrochloric acid solution (JT Baker, Phillipsburg,
Means and standard deviations were calculated
New Jersey). The dead volume was then analyzed via
(SPSS 11.5, SPSS, Chicago, Illinois) for each component
spectrophotometry (Beckman Instruments, Fullerton, Cal-
of the total drug mass, nebulizer loss, and estimated am-
ifornia), using a known amount of solvent added to the
bient loss. A 2-way factorial analysis of variance (ANOVA)
dead volume. To avoid contamination with residual albu-
was performed for the masks and distances, with an alpha
RESPIRATORY CARE • AUGUST 2007 VOL 52 NO 8
EFFECT OF FACE MASK DESIGN ON INHALED MASS OF ALBUTEROL
Fig. 2. Mean inhaled percentage of nominal dose with 3 types of face mask and 3 distances from the mannequin face. The differencesbetween the fish mask and both the standard mask and the dragon mask were significant at all distances. Inhaled percentage of nominaldose was significantly greater with all masks at 0 cm than at 2 cm. * p Ͻ 0.001 for all comparisons of 0 cm versus 2 cm. † p Ͻ 0.001 forfish mask versus standard mask and dragon mask at all distances.
level of 0.05.13 Follow-up comparisons of each device at
the nebulizer, and lost to the ambient air, for each type of
each distance were performed using 1-way ANOVA with
A 1-way factorial ANOVA with Bonferroni adjustment
We calculated the effect size, which is an index of the
for masks and distances indicated a statistically greater
magnitude of a treatment effect. Unlike tests for significance,
inhaled drug mass with the fish mask than with the stan-
measures of effect size in ANOVA determine the degree of
dard mask or the dragon mask, overall (p Ͻ 0.001), and
association between variables and the effect of the dependent
significant decrease in inhaled drug mass as distance in-
variable. We used the partial eta squared (2) value to esti-
mate the degree of association between the samples.
Figure 2 shows the percentage of the nominal dose val-
ues collected on the inhalation filter. Bonferroni compar-
isons of the 3 masks showed significant differences(p Ͻ 0.001) in inhaled drug mass between the standard
Table 2 lists the mean Ϯ SD values for the percent of
mask and the fish mask, and between the fish mask and the
the nominal dose collected on the inhalation filter, left in
dragon mask. However, there was no significant differ-
Drug Mass on the Inhalation Filter, Left in the Nebulizer, and Estimated Ambient Loss
*Significant difference overall (p Ͻ 0.001). †Significant difference overall across distances (p Ͻ 0.001).
RESPIRATORY CARE • AUGUST 2007 VOL 52 NO 8
EFFECT OF FACE MASK DESIGN ON INHALED MASS OF ALBUTEROL
ence between the standard mask and the dragon mask. Thepartial 2 was 0.617 compared among the 3 distances, and0.591 compared among the 3 masks, which indicates thatthe probability of nonoverlap among the 3 groups is ap-proximately 33–38%, according to Cohen’s standard.14
Discussion
The results of this in vitro study indicate that the inhaled
drug mass with the fish mask was significantly higher thanwith the standard mask or dragon mask. Furthermore, ourresults are consistent with previous studies that reported asignificant drop in the inhaled drug mass when the maskwas moved away from the face.4–11,15,16
The standard pediatric aerosol mask is a smaller version
of the adult mask and has a considerably larger dead spacethan the fish mask or dragon mask. The 2-cm side holes inthe standard mask allow more aerosol particles to escape
Fig. 3. Aerosol trajectory with the fish mask. With the fish mask theaerosol is aimed more directly at the nasal/oral area than with the
during nebulization. The side-holes on the dragon mask
are 1 cm in diameter, so, theoretically, less aerosol shouldbe lost than with the standard mask, but our results do notsupport that theory. The lower inhaled drug mass with the
The standard mask and dragon mask direct the aerosol
standard mask and dragon mask may be due to aerosol
to the upper portion of the mask, whereas the fish mask
inertia (the tendency of an object to travel in a straight line
directs the aerosol towards the nasal/oral area (see Fig. 3).
once it is moving). In the standard mask and the dragon
We hypothesize that the difference in angle of aerosol
mask, the aerosol enters the mask traveling upwards, to-
entry into the mask influences inhaled mass, because aim-
wards the top of the mask, and inertia may cause the
ing the aerosol more directly at the nasal/oral area reduces
aerosol particles to impact the inner surface of the mask,
aerosol impact on the mask. A recent 3-dimensional nu-
whereas with the fish mask the aerosol travels directly
merical study by Shakked et al17 on the administration of
toward the nasal/oral area (Fig. 3). In a previous study that
aerosolized drugs to infants via a hood supports our theory
compared inhaled drug mass delivered via T-piece versus
of the importance of directing the aerosol toward the nasal/
via standard pediatric mask, we found a higher inhaled
oral area. Shakked et al found that the number of aerosol
drug mass with the T-piece.4 The T-piece is constructed
particles that penetrated the nostrils of their infant model
with a 90° angle, with a nebulizer that directs the aerosol
significantly decreased the further away the aerosol funnel
stream toward the patient’s face. Because of this physical
design, we hypothesized that the inhaled drug mass with
It is also possible that a better face seal is created with
the T-piece, with or without distancing the mask from the
the fish mask, by the extended cover on the face. Also, the
mannequin face, was greater than with all of the masks we
fish mask’s smaller side holes may keep more aerosol
particles in the mask during the treatment time and reduce
Sangwan and collaborators15 nebulized radiolabeled nor-
mal saline to an infant breathing model. They used 7 com-
Though several studies have reported data on inhaled drug
mercially available face masks interfaced with 3 compat-
mass when the face mask is moved away from the face
ible fitting nebulizers, to compare the facial deposition of
model,4–11,15,16 we found only 3 studies that evaluated the
aerosol. The fish mask in combination with the Pari LC
impact of leak between the pediatric mask and the face on
Plus nebulizer had the highest inhaled drug mass, at 6.0%
inhaled drug mass when the aerosol is generated via jet neb-
of the nominal dose. It also had one of the lowest eye and
ulizer.4,5,16 Our previous study reported data that compared
facial aerosol depositions. The combination of the Hudson
the inhaled drug mass with a standard mask versus with a
mask and the Misty-Neb nebulizer resulted in 66% less
T-piece at 0 cm, 1 cm, and 2 cm from the inhalation filter.4
inhaled drug than the combination of the fish mask and the
However, in that study, albuterol nebulization was run to the
Pari LC Plus nebulizer.15 In a similar study, Smaldone and
onset of sputtering, with no tapping of the nebulizer. The
colleagues nebulized 0.25 mg of budesonide to a pediatric
mean inhaled percentage of the nominal dose with the stan-
breathing model. They found that the combination of the
dard aerosol mask at 0 cm (2.88%), 1 cm (1.61%), and 2 cm
fish mask and the Pari LC Plus yielded about 65% higher
(1.3%) in that study4 compares well to the present results
inhaled drug mass than the combination of the standard
with the standard mask: 2.18%, 1.45%, and 0.92%, respec-
mask and the Hudson Updraft II jet nebulizer.16
tively. The present study values also compare well to those
RESPIRATORY CARE • AUGUST 2007 VOL 52 NO 8
EFFECT OF FACE MASK DESIGN ON INHALED MASS OF ALBUTEROL
found by Everard et al, who nebulized 4 mL (40 mg) of
uated as a clinical strategy for delivering aerosolized medi-
sodium cromoglycate. Their mean percentage of the nominal
cation to children. Also, the design of the face mask affects
dose values at 0 cm, 1 cm, and 2 cm were 3.13%, 1.2%, and
nebulized aerosol delivery to pediatric patients. Clinical re-
0.45%, respectively.5 Smaldone et al16 quantified in vitro the
search is necessary to determine whether the design of nebu-
influence of the face mask on the inhaled mass of budesonide
lizers or face masks affects clinical response. These findings
from jet nebulizers and pressurized MDIs with valved hold-
may be useful for interpreting future clinical studies on face
ing chambers. The configuration that lacked mask/face seal
mask delivery of aerosolized drugs to pediatric patients.
was associated with significantly lower inhaled mass than thesealed mask/face configuration, with both the MDIs and the
ACKNOWLEDGMENTS
A recent report by Shah et al, which evaluated force-
Thanks to Stefan Frembgen PhD, IngMar Medical, Pittsburgh, Pennsyl-
dependent static dead space of face masks used with valved
vania, for instruction and assistance with the Active Servo Lung 5000
holding chambers, reinforced the importance of both the
mask design and the integrity of the mask/face seal.8 Themask’s ability to seal to the face was evaluated by apply-
REFERENCES
ing different forces. Although the masks that allowed moreforce to obtain a better seal were more flexible and asso-
1. Hess D. Nebulizers: principles and performance. Respir Care 2000;
ciated with a greater reduction of the mask dead space
2. Collies GG, Cole CH, LeSouef PN. Dilution of nebulised aerosols by
volume, Shah et al cautioned about the possible impact of
air entrainment in children. Lancet 1990;336(8711):341–343.
the mask pressure on the child’s face, because the mask
3. Iles R, Lister P, Edmunds AT. Crying significantly reduces absorption
pressure could offset the benefit of the improved aerosol
of aerosolised drug in infants. Arch Dis Child 1999;81(2):163–165.
delivery obtained by a better mask/face seal.
4. Restrepo RD, Dickson SK, Rau JL, Gardenhire DS. An investigation
of nebulized bronchodilator delivery using a pediatric lung model of
There are several limitations to the present study. Erratic
spontaneous breathing. Respir Care 2006;51(1):56–61.
breathing because of crying is frequent in infants and toddlers
5. Everard ML, Clark AR, Milner AD. Drug delivery from jet nebu-
receiving aerosol.3 The steady-state nature of an in vitro study
lizers. Arch Dis Child 1992;67(5):586–591.
does not reflect the potential differences one might expect
6. Hayden JT, Smith N, Woolf DA, Barry PW, O’Callaghan C. A
when studying human subjects. A second limitation was the
randomised crossover trial of facemask efficacy. Arch Dis Child2004;89(1):72–73.
lack of a true mass/balance measurement, because we were
7. Amirav I, Mansour Y, Mandelberg A, Bar-Ilan I, Newhouse MT.
unable to capture aerosol lost to the ambient air. It is theo-
Redesigned facemask improves “real life” aerosol delivery for Ne-
retically possible that some aerosol collected on the filter
buchamber. Pediatr Pulmonol 2004;37(2):172–177.
could be lost during exhalation back through the filter, which
8. Shah SA, Berlinski AB, Rubin BK. Force-dependent static dead
would lead to underestimation of the inhaled drug mass. How-
space of face masks used with holding chambers. Respir Care 2006;51(2):140–144.
ever, we believe such loss is negligible, because liquid aero-
9. Amirav I, Newhouse MT. Aerosol therapy with valved holding cham-
sol particles are collected on the filter. Another limitation was
bers in young children: importance of the face mask seal. Pediatrics
our use of a preset nebulization time, instead of nebulizing
until sputter. According to a study by Rau et al, the expected
10. Amirav I, Mansour Y, Mandelberg A, Bar-Ilan I, Newhouse MT.
average nebulization time with the Misty-Neb with 3 mL at
Redesigned face mask improves “real life” aerosol delivery for Ne-buchamber. Pediatr Pulmonol 2004;37(2):172–177.
8 L/min is approximately 12 min.18 We used a preset nebu-
11. Esposito-Festen JE, Ates B, van Vliet FJ, Verbraak AF, de Jongste
lization time of 5 min to provide a consistent aerosol output,
JC, Tiddens HA. Effect of a facemask leak on aerosol delivery from
for better comparison. Hence, the percentage of inhaled drug
a pMDI-spacer system. J Aerosol Med 2004;17(1):1–6.
mass on the inhalation filter in the present study may under-
12. Smaldone GC. Drug delivery via aerosol systems: concept of “aero-
estimate the real percentage patients actually get, because our
sol inhaled.” J Aerosol Med 1991;4(3):229–235.
13. Kirk RE. Experimental design: procedures for the behavioral sci-
nebulization time is probably shorter than actual nebulization
ences. Belmont CA: Brooks/Cole Publishing Co; 1994:237–244.
time in the clinic, and nebulization might therefore be con-
14. Cortina JM, Nouri H. Effect size for ANOVA designs. Iowa City:
sidered incomplete. And, finally, we did not measure aerosol
particle size. Although particle size measurements can be
15. Sangwan S, Gurses BK, Smaldone GC. Facemasks and facial dep-
obtained separately, such measurements may not be repre-
osition of aerosols. Pediatr Pulmonol 2004;37(5):447–452.
16. Smaldone GC, Berg E, Nikander K. Variation in pediatric aerosol de-
sentative of particle sizes in in vitro testing or actual lung
livery: importance of facemask. J Aerosol Med 2005;18(3):354–363.
17. Shakked T, Broday DM, Katoshevski D, Amirav I. Administration
of aerosolized drugs to infants by a hood: a three-dimensional nu-
Conclusions
merical study. J Aerosol Med 2006;19(4):533–542.
18. Rau JL, Ari A, Restrepo RD. Performance comparison of nebulizer
Our data suggest that holding the aerosol mask away from
designs: constant-output, breath-enhanced, and dosimetric. Respir
the child’s face (the “blow-by” technique) should be reeval-
RESPIRATORY CARE • AUGUST 2007 VOL 52 NO 8
MARCIALIO EPIGRAMOS TEATRAS Skirmantë Packoèinaitë-Birþietienë Vilniaus universiteto Kauno humanitarinio fakulteto lektorë Ðios publikacijos tikslas yra glaustai apþvelgtiLaiðkas skamba kaip savotiðkas literatûrinis ma-romënø epigramø autoriaus Marcialio poetiniønifestas. Nors jis nëra pakankamai iðsamus, betkûrinëliø ryðá su antikinio teatro komikos for-palieèia
NCCI 2010 -National Conference on Computational Instrumentation CSIO Chandigarh, INDIA, 19-20 March 2010 ANALYSIS OF AUTO DYNAMIC INTENSITY VARIATION FOR ACTIVE DISPLAY INTENSITY CONTROL FOR WIDE BACKGROUND INTENSITY Upasna, Mandal Danvir, Karar Vinod*, Saini Surender Singh * Institute of Engineering and Technology, Bhaddal, Ropar, Punjab *Central Scientific Instruments Organisation, Chandig
 EFFECT OF FACE MASK DESIGN ON INHALED MASS OF ALBUTEROL
Introduction
EFFECT OF FACE MASK DESIGN ON INHALED MASS OF ALBUTEROL
Introduction

 EFFECT OF FACE MASK DESIGN ON INHALED MASS OF ALBUTEROL
*Designed specifically for use with PARI nebulizers.
EFFECT OF FACE MASK DESIGN ON INHALED MASS OF ALBUTEROL
*Designed specifically for use with PARI nebulizers. EFFECT OF FACE MASK DESIGN ON INHALED MASS OF ALBUTEROL
Fig. 2. Mean inhaled percentage of nominal dose with 3 types of face mask and 3 distances from the mannequin face. The differencesbetween the fish mask and both the standard mask and the dragon mask were significant at all distances. Inhaled percentage of nominaldose was significantly greater with all masks at 0 cm than at 2 cm. * p Ͻ 0.001 for all comparisons of 0 cm versus 2 cm. † p Ͻ 0.001 forfish mask versus standard mask and dragon mask at all distances.
EFFECT OF FACE MASK DESIGN ON INHALED MASS OF ALBUTEROL
Fig. 2. Mean inhaled percentage of nominal dose with 3 types of face mask and 3 distances from the mannequin face. The differencesbetween the fish mask and both the standard mask and the dragon mask were significant at all distances. Inhaled percentage of nominaldose was significantly greater with all masks at 0 cm than at 2 cm. * p Ͻ 0.001 for all comparisons of 0 cm versus 2 cm. † p Ͻ 0.001 forfish mask versus standard mask and dragon mask at all distances.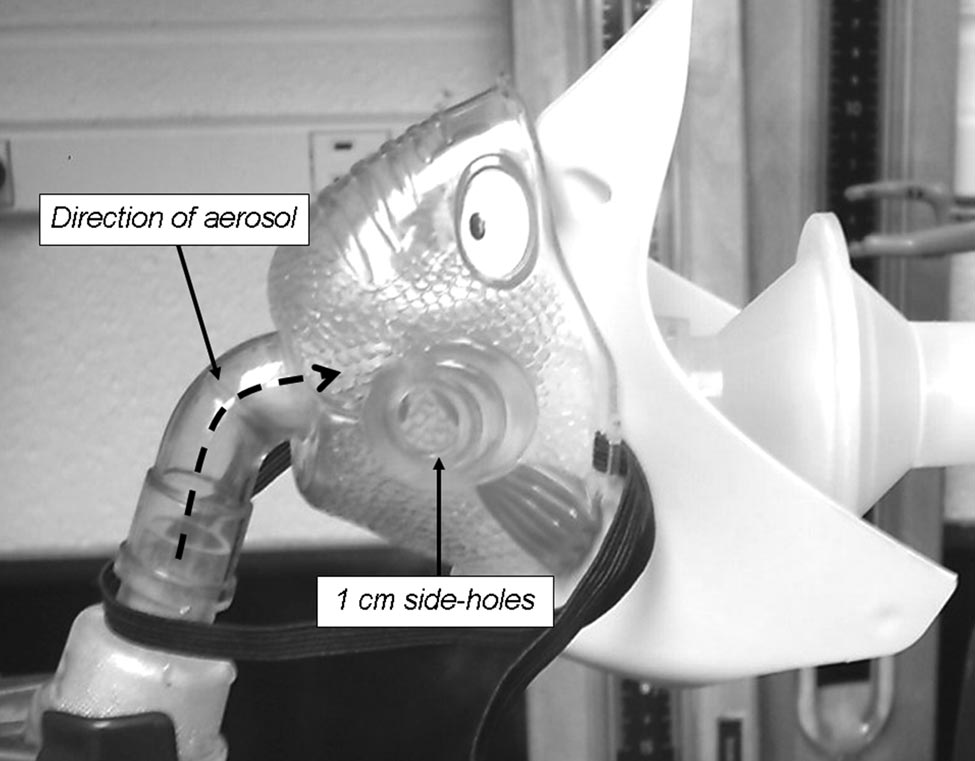 EFFECT OF FACE MASK DESIGN ON INHALED MASS OF ALBUTEROL
ence between the standard mask and the dragon mask. Thepartial 2 was 0.617 compared among the 3 distances, and0.591 compared among the 3 masks, which indicates thatthe probability of nonoverlap among the 3 groups is ap-proximately 33–38%, according to Cohen’s standard.14
Discussion
EFFECT OF FACE MASK DESIGN ON INHALED MASS OF ALBUTEROL
ence between the standard mask and the dragon mask. Thepartial 2 was 0.617 compared among the 3 distances, and0.591 compared among the 3 masks, which indicates thatthe probability of nonoverlap among the 3 groups is ap-proximately 33–38%, according to Cohen’s standard.14
Discussion