Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Effect of cigarette smoking on oral elastase activity in adult periodontitis patients
9012_IPC_AAP_553060 2/15/00 11:02 AM Page 58
Effect of Cigarette Smoking on Oral Elastase Activity in Adult Periodontitis Patients Nathalie C. Pauletto,* Kirsti Liede,† Anja Nieminen,† Hannu Larjava,* and Veli-Jukka Uitto* Background: We have previously reported that elastase activ-
ity in oral fluids is significantly increased in most adult peri-odontitis patients. In some patients, however, elastase levelsremain low despite the presence of deep periodontal pockets. In this study we explored whether or not smoking is related tothe unexpected low elastase values in these patients. Methods: We determined what proportion of the periodonti-
tis patients that showed low oral elastase values were smokers.
Paraffin-stimulated saliva or oral rinse samples (3 ml of water,
30 second rinse) were assayed for elastase activity by incubat-
ing with 1 mM succinyl-alanyl-alanyl-valine-p-nitroanilide for
epithelial cells, following their activation.1
20 hours at 37°C, and the color formation read with a spec-
trophotometer. Neutrophil numbers were analyzed by staining the
cells in the oral rinse smear samples. Results: In 2 patient groups, one in Helsinki, Finland (n =
studied for their possible use as indica-
46) and the other in Vancouver, British Columbia (n = 25), 63%
and 83%, respectively, of the adult periodontitis patients who
had one or more pockets ≥6 mm and had low oral elastase val-
ues (increase of optical density <0.5) were smokers. Non-smok-
ing periodontitis patients had elevated neutrophil numbers com-
pared to healthy subjects, while the smoking patients showed
ies indicate that neutrophil elastase lev-
no significant change. Next we analyzed elastase levels in stim-
els in gingival crevicular fluid, saliva, or
ulated whole saliva in a group of smokers (n = 300) and those
who had quit smoking (n = 102). Smokers had significantly
lower oral elastase levels than former smokers in both advanced
and moderate periodontitis groups. In this subject group, 56%
normal levels following healing.13-16 Our
of all smokers with periodontitis (at least one pocket ≥6 mm)
had oral elastase values less than 0.5 U while only 31% of those
periodontitis patients have elevated oral
patients who had quit smoking had low values. Conclusions: Cigarette smoking leads to lowered elastase
and neutrophil levels in the oral cavity. The oral neutrophil elas-
tase assay, therefore, cannot be used to measure the periodon-
surement was tested for detection of peri-
tal status of smokers. J Periodontol 2000;71:58-62.KEY WORDS
point of 0.5 U, about 28% of the patientswith one or more pockets ≥6 mm tested
Periodontal pockets/diagnosis; periodontitis/diagnosis; neutrophils; elastase; smoking/adverse effects; tobacco/adverse effects; saliva/enzymology.
tory factor for that finding. Smoking hasmany tissue effects that appear to play
* Department of Oral Biological and Medical Sciences, Faculty of Dentistry, University of
† Department of Periodontology, Institute of Dentistry, University of Helsinki, Helsinki,
demonstrates that oral elastase valuesand neutrophil counts are lower in smok-ing periodontitis patients than in non-smokers with the same degree of dis-
9012_IPC_AAP_553060 2/15/00 11:02 AM Page 59
Pauletto, Liede, Nieminen, Larjava, Uitto
ease. It also shows that when the smoking is stopped,
ifest.16 Change in optical density of 0.5 (0.5 U) was
the oral elastase values return to the level of non-
taken as the cut-off value for the positive test result.
Both free elastase in the oral fluid samples and elas-tase released from neutrophils during the procedure
MATERIALS AND METHODS Study Population Neutrophil Count
A total of 493 adults, aged 31 to 80, were included in
Following the collection of the oral fluid samples, 10
the study. Initially 2 groups consisting of 46 and 25
µl of the samples were smeared on a glass slide and
patients with moderate to severe periodontitis were
fixed with cytospray.§ The cells were stained using a
analyzed for oral rinse elastase activity at the Univer-
modification of the Wright-Giemsa technique. Two
sity of Helsinki and the University of British Columbia,
drops of 0.15% Wright-Giemsa stain‡ were placed on
respectively. The number of gingival pockets >5 mm
the fixed smears for 1 minute followed by a 30-sec-
in depth varied from 5 to 28. Twenty subjects with
ond rinse under tap water. The number of neutrophils
healthy periodontium who were non-smokers served
(PMN) and epithelial cells in the samples was mea-
as controls. Subsequently, a group of adults who were
sured by counting 40 randomly selected squares of
either smokers (n = 300) or former smokers (n = 102)
0.5 cm2 under light microscopy. Accuracy and repro-
were randomly selected from a large pool of subjects
ducibility of the measurements were assessed by
participating in a cancer prevention study of the
repeated counting of 10 randomly selected slides.
National Public Health Institute of Finland.19 The exclu-sion criteria were cancer, severe coronary disease,
Statistical Analysis
chronic renal hypofunction, hepatic cirrosis, antico-
Significance of the differences in the test groups was
agulant medication, A or E vitamin supplement intake,
analyzed by one-way analysis of variance test
and alcohol abuse. All subjects had at least 15 natural
(ANOVA). Spearman rank correlation test was used
teeth. They were analyzed for their periodontal condi-
to analyze the relationship of elastase activity and num-
tion and salivary elastase activity. In this group, 95%
of the smokers and 88% of the former smokers had
probing depths ≥5 mm or more. None of the patients
We have repeatedly observed that most of the patients
were undergoing periodontal therapy at the time of the
with moderate to advanced periodontitis have high oral
study. The patients were examined and tested either
elastase values. In this study, 80% of the patients, both
by periodontists (KL ar A.N.) or a periodontal gradu-
smokers and non-smokers, who had gingival pockets
>5 mm had oral elastase activity higher than 0.5 U, a
Oral Elastase Assay
cut-off value for the test selected based on our previ-
In the first study elastase was measured either in stim-
ous studies.16,17 When exploring reasons for the low
ulated saliva (Helsinki group) or in oral rinse samples
elastase activity in the remaining patients, we observed
(Vancouver group). Stimulated saliva was collected by
that in 2 periodontitis patient groups, one examined in
allowing the subjects to chew paraffin for 30 seconds
Helsinki and the other in Vancouver, 83% and 63% of
and then collecting the whole saliva. For oral rinse
the patients, respectively, who had low oral elastase
specimens, subjects rinsed their mouths with 3 ml of
values were smokers (Table 1). Data analysis showed
tap water for 30 seconds. In the study on oral elastase
that periodontitis patients who smoked had a signifi-
of smokers, stimulated whole saliva samples were col-
cantly lower salivary elastase than non-smoking pa-
lected as above. Our previous study has shown that
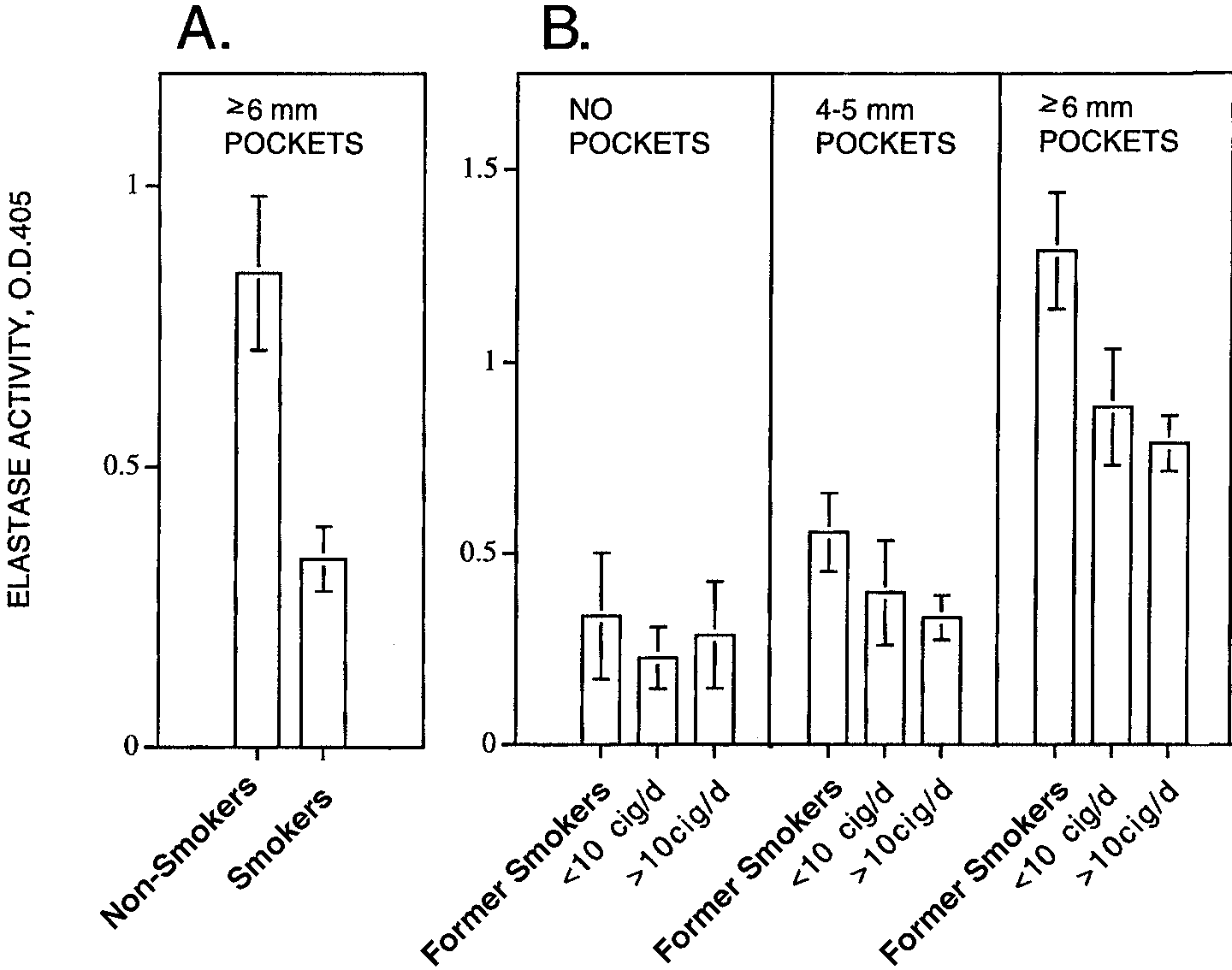
tients with similar disease severity (Fig. 1A). Because
both whole saliva and oral rinse samples measure
oral elastase is primarily derived from neutrophils, we
equally well the activity of neutrophil elastase that is
investigated whether the number of these cells was
transferred into the oral cavity along with crevicular
altered in oral rinse samples of the smokers compared
fluid.16 The collected samples were stored at −20°C
to non-smokers with a similar degree of periodontitis.
until assayed. After thawing, the samples were cen-
Indeed, while the number of neutrophils in periodon-
trifuged at 2,700 × g for 10 minutes and 100 µl of the
titis patients who did not smoke was about twice that
supernate was incubated for 20 hours at 37°C in 0.01
of the healthy group, the neutrophil count was only
M tris-HCl-0.2 M NaCl-buffer, pH 7.5, containing 1 mM
slightly elevated in the smoking periodontitis group
succinyl-alanyl-alanyl-valine-p-nitroanilide‡ as the sub-
(Table 2). In this population there was a significant
strate for neutrophil elastase.20 The intensity of the
correlation between the elastase activity and the num-
color formed was read spectrophotometrically. Based
ber of neutrophils in the rinse specimens (r = 0.358,
on our earlier studies, the 20-hour incubation time wasselected because some oral samples with a low elas-
‡ Sigma Chemical Co., St. Louis, MO. § Fisher Scientific Ltd., Nepean, ON.
tase activity required a longer incubation time to man-
Zeiss, Axioskop, Oberkochen, Germany.
9012_IPC_AAP_553060 2/15/00 11:02 AM Page 60
Oral Elastase in Smokers P <0.01; Spearman rank correlation test). By com-parison, the number of epithelial cells in the rinse spec-
Percentage of Smokers in Periodontitis
imens was increased in both non-smoking and smok-
Patients With Low Oral Elastase Levels
ing periodontitis patients (Table 2).
In order to determine the relation of oral elastase
values to smoking frequency, 402 subjects weregrouped as heavy smokers (>10 cigarettes per day);
moderate smokers (<10 cigarettes per day); and for-
mer smokers. In both smoking groups, patients withat least one pocket ≥6 mm had markedly lower elas-
tase values than similar patients who were formersmokers (Fig. 1B). The same trend was observed in
patients with 4 to 5 mm pockets. Nosignificant differences were observedin oral elastase levels of smokers andnon-smokers without periodontalpockets. The overall effect of smok-ing on oral elastase levels of peri-odontitis patients was highly signifi-cant (P <0.001; ANOVA). It is evidentthat the salivary elastase levels ofpatients who had quit smoking arenot significantly different than thosesubjects who had never smoked, inboth periodontitis (0.85 ± 0.79 ver-sus 1.10 ± 0.59) and healthy groups(0.34 ± 0.58 versus 0.20 ± 0.41).
with one or more pockets ≥6 mm andlow elastase values were calculated,we observed that 56% of all smokershad elastase values less than 0.5 Uwhile only 31% of patients who hadquit smoking had low elastase val-ues. When smokers were excludedfrom the initial study populations thatconsisted of moderate to severe peri-
Figure 1. Oral elastase activity in cigarette smokers with adult periodontitis. A. Elastase activity was measured in stimulated whole saliva of 18 non-smoking and 27 smoking periodontitis patientswith at least one 6 mm gingival pocket. B. Oral elastase activity in 300 smokers and 102 former smokers.The results are mean ± S.E.M.
patients with lower than predicted oralelastase activity. DISCUSSION Neutrophil and Epithelial Cell Counts in Smoking and
Oral elastase activity has the potentialto serve as an important adjunctive
Non-Smoking Periodontitis Patients
method in screening for periodontitisand monitoring treatment outcomes.
water rinse samples is a non-invasive,easy to perform, and relatively spe-
* Significant difference compared to healthy group (P <0.01; ANOVA test).
9012_IPC_AAP_553060 2/15/00 11:02 AM Page 61
Pauletto, Liede, Nieminen, Larjava, Uitto
released from neutrophils during the experimental pro-
alpha 1-protease inhibitor have been found to be
cedure provides an easy way to approximate the num-
lower in the gingival crevicular fluid of smokers than
ber of oral leukocytes which is known to increase with
non-smokers.41 Thus, all the information on the effects
periodontitis.21 The drawback is that a certain pro-
of smoking on neutrophils and tissue elastase levels
portion of patients do not test positive with this method,
obtained from previous studies and the present appear
even though they have deep periodontal pockets. Fol-
to point to the conclusion that in periodontitis patients
lowing our first studies we assumed that the unex-
who smoke, neutrophils and possibly macrophages,
pected negative results may be partially explained by
rather than migrating via the gingival crevice to the
limited sensitivity of the test that reflects the sum of
oral cavity, are accumulated in periodontal tissue where
active elastase derived from all periodontal sites dur-
they release their constituents leading to increased
ing the sample collection period, and partially by indi-
degradation of connective tissue components. This
vidual fluctuation of neutrophil migration rate into the
hypothesis needs to be explored in detail. While the pri-
oral cavity. In certain periodontitis patients, however,
mary goal of periodontal therapy in individuals who
the low elastase values were thought to reflect the
smoke should be directed to cessation of cigarette
actual disease process that deviates from the normal
smoking, other approaches aiming at minimizing the
inflammatory response. In this study we were able to
harmful effects of leukocyte products on the peri-
demonstrate that tobacco smoking decreases signifi-
odontium should also be considered. In this context,
cantly the oral elastase levels. We observed that heavy
drugs that stabilize neutrophils and inhibit elastase and
smokers had clearly lower oral elastase activity than
other proteases should also be tested for their benefi-
moderate smokers or non-smokers with similar sever-
cial effects in periodontal treatment.
ity of periodontitis. It is well demonstrated that ciga-
To conclude, the present study shows that a signif-
rette smoking has a significant impact on the risk for
icant proportion of periodontitis patients who have low
developing periodontal disease. Both the incidence and
elastase levels in oral fluids are smokers. When the
severity of periodontitis is greater in smokers than in
oral elastase test is performed exclusively on adult
non-smokers.22-25 The odds ratio for moderate smok-
periodontitis patients who do not smoke tobacco, very
ers (15 to 30 packs per year) is reported to be 2.8 and
good sensitivity values can be obtained. The low oral
for heavy smokers (≥30 packs per year), 4.8.24,25
elastase values of smokers should not be interpreted
Tobacco users do not respond to periodontal treat-
to indicate lack of periodontitis activity. In contrast, it
ment as well as non-smokers, reflecting the general
may indicate an abnormal leukocyte function and
impairment of the tissue repair process.26-28 The effect
of smoking seems reversible, because the risk of devel-oping periodontitis is clearly reduced upon cessation
ACKNOWLEDGMENTS
of smoking.29 Accordingly, in our study the elastase
This study was supported by grants from the Medical
values for former smokers were comparable with those
Research Council of Canada and the Finnish Dental
There are several ways that tobacco substances can
act on oral tissues. Tobacco causes constriction and
REFERENCES
reduced permeability of peripheral blood vessels.30
1. Birkedal-Hansen H. Role of matrix metalloproteinases in
Migration of neutrophils through capillary walls is inhib-
human periodontal diseases. J Periodontol 1993;94:474-
ited due to paralysis of the cell membrane and inhibi-
tion of the inactivator of chemotaxis.31-33 At the same
2. Gangbar S, Overall CM, McCulloch CAG, Sodek J. Iden-
time, there is an increase of about 25% in the number
tification of polymorphonuclear leukocyte collagenase
of leukocytes in peripheral blood.34 For these reasons
and gelatinase activities in mouthrinse samples: Corre-lation with periodontal disease activity in adult and juve-
there is an abnormal accumulation of neutrophils and
nile periodontists. J Periodont Res 1990;25:257-267.
macrophages in inflamed tissues, which has been best
3. Lamster IB. In-office diagnostic tests and their role in
documented in lung tissue.35,36 Tobacco smoking has
supportive periodontal treatment. Periodontol 2000
been found to activate neutrophils to release tissue-
damaging substances such as elastase and active oxy-
4. Villela B, Cogen RB, Bartolucci AA, Birkedal-Hansen H.
Collagenolytic activity in crevicular fluid from patients
gen species.37,38 Elastase plays a key role in cigarette
with chronic adult periodontitis, localized juvenile peri-
smoke-induced emphysema. Elastase-deficient mice
odontitis and gingivitis, and from healthy control subjects.
do not develop emphysema when exposed to ciga-
J Periodont Res 1987;22:381-389.
rette smoke.39 Due to the action of active oxygen
5. Louie H, Larjava H. A critical evaluation of diagnostic
species, the tissue levels of alpha 1-protease inhibitor
tests for periodontal disease. Can Dent J 1994;60:1042-1049.
are lowered allowing elastase and other proteases to
6. Palcanis KG, Larjava IK, Wells BR, et al. Elastase as an
remain longer in tissue in an active state.40 Levels of
indicator of periodontal disease progression. J Periodontol
both functional elastase and elastase complexed with
9012_IPC_AAP_553060 2/15/00 11:02 AM Page 62
Oral Elastase in Smokers
7. Uitto V-J, Appelgren R, Robinson PJ. Collagenase activ-
27. Preber H, Linder L, Bergstöm J. Periodontal healing and
ity in extracts of inflamed human gingiva. J Periodont Res
periopathogenic microflora in smokers and non-smok-
ers. J Clin Periodont 1995;22:946-952.
8. Uitto V-J, Suomalainen K, Sorsa T. Salivary collagenase.
28. Nakamura Y, Romberger DJ, Tate L, Ertl RF, Kawamoto
Origin, characteristics and relationship to periodontal
M, Adashi Y. Cigarette smoking inhibits lung fibroblast
health. J Periodont Res 1990;25:135-142.
proliferation and chemotaxis. Am J Res Crit Care Med
9. Janoff A. Elastase in tissue injury. Ann Rev Med 1985;
29. Haber J, Kent RL. Cigarette smoking in periodontal prac-
10. Herrick S, Ashcroft G, Ireland G, Horan M, McCollum
tice. J Periodontol 1992;63:100-106.
C, Ferguson M. Upregulation of elastase in acute wounds
30. Powell JT. Vascular damage from smoking: Disease
of healthy aged humans and chronic venous leg ulcers
mechanisms at the arterial wall. Vasc Med 1998;3:21-
are associated with matrix degradation. Lab Invest
31. Lannan S, McLean A, Drost E, Gillooly M, Donaldson K,
11. Smedly LA, Tonnesen MG, Sandhaus RA, et al. Neu-
Lamb D. Changes in neutrophil morphology and mor-
trophil-mediated injury to endothelial cells. Enhance-
phometry following exposure to cigarette smoke. Int J
ment by endotoxin and essential role of neutrophil elas-
tase. J Clin Invest 1986;4:1233-1243.
32. MacNee W, Bridgeman MM, Marsden M, Dorst E, Lan-
12. Uitto V-J, Haapasalo M. The origin of collagenase and
nan S, Selby C. The effects of N-acetylcysteine and glu-
elastase in dental plaque. In: Lehner T, Climasoni G, eds.
tathione on smoke-induced changes in lung phagocytes
Borderland Between Caries and Periodontal Disease.
and epithelial cells. Am J Med 1991;91:60-66.
Geneva: Editions Medicine et Hygiene; 1986:175-170.
33. Robbins RA, Nelson KJ, Gossman GL, Koyama S, Ren-
13. Armitage GC, Jeffcoat MK, Chadwick DE, et al. Longi-
nard SI. Complement activation by cigarrette smoke.
tudinal evaluation of elastase as a marker for the pro-
Am J Physiol 1991;260:254-259.
gression of periodontitis. J Periodontol 1994;65:120-
34. Bain BJ, Rothwell M, Feher MD, Robinson R, Brown J,
Sever PS. Acute changes in haematological parameters
14. Gustafsson A, Asman B, Bergström K. Granulocyte elas-
on cessation of smoking. J Roy Soc Med 1992;85:80-
tase in gingival crevicular fluid. J Clin Periodontol
35. Bosken CH, Doerscchuck CM, English D, Hogg JC. Neu-
15. Palcanis KG, Larjava IK, Wells BR, et al. Elastase as an
trophil kinetics during active cigarette smoking in rab-
indicator of periodontal disease progression. J Peri-
bits. J Appl Physiol 1991;67:609-611.
36. Wallace JM, Oishi JS, Barber RG, Simmons MS, Tashkin
16. Uitto V-J, Nieminen A, Coil J, Hurttia H, Larjava H. Oral
DP. Lymphocytic subpopulation profiles in broncho-
fluid elastase as an indicator of periodontal health. J
alveolar lavage fluid and peripheral blood from tobacco
Clin Periodontol 1996;23:30-37.
and marijuana smokers. Chest 1994;105:847-852.
17. Nieminen A, Nordlund L, Uitto V-J. The effect of treat-
37. Renkema TE, Postma DS, Noordhoek JA, Sluiter HJ,
ment on the activity of salivary proteases and glycosi-
Kauffman HF. Influence of in vivo prednisolone on
dases in adults with advanced periodontitis. J Periodontol
increased in vitro O2 generation by neutrophils in emphy-
sema. Eur Resp J 1993;6:90-95.
18. Barbour ES, Nakashima K, Zhang J, et al. Tobacco and
38. Hind CR, Joyce H, Tennent GA, Pepys MB, Pride NB.
smoking: Environmental factors that modify the host
Plasma leukocyte elastase concentrations in smokers. J
response (immune system) and have impact on peri-
odontal health. Crit Rev Oral Biol Med 1997;8:437-460.
39. Hautamäki RD, Kobayashi DK, Senior RM, Shapiro SD.
19. The ATBC Cancer Prevention Study Group. The alpha-
Requirement of macrophage elastase for cigarette
tocopherol, beta-carotene lung cancer prevention study:
smoke-induced emphysema in mice. Science 1997;
Design, methods, participant characteristics and com-
pliance. Ann Epidemiol 1994;4:1-10.
40. Ogushi F, Hubbard RC, Vogelmeier C, Fells GA, Crys-
20. Bieth J, Spiess B, Wermuth CG. The synthesis and ana-
tal RG. Risk factors for emphysema. Cigarette smoking
lytical use of a highly sensitive and convenient substrate
is associated with reduction in the association rate con-
for elastase. Biochem Med 1974;11:350-357.
stant of lung alpha1-antitrypsin for neutrophil elastase.
21. Klinkhamer JM. Quantitative evaluation of gingivitis and
J Clin Invest 1991;87:1060-1065.
periodontal disease. The orogranulocytic migratory rate.
41. Alavi AL, Palmer RM, Odell EW, Coward PY, Wilson RF.
Elastase in gingival crevicular fluid from smokers and
22. Beck JD. Methods of assessing risk for periodontitis and
non-smokers with chronic inflammatory periodontal dis-
developing multifactorial models. J Periodontol 1994;
ease. Oral Dis 1995;3:110-114.
23. Bergström J, Preber H. Tobacco use as a risk factor. J
Send reprint requests to: Dr. Veli-Jukka Uitto, Department
of Oral Biological and Medical Sciences, University of British
24. Grossi SG, Zambon JJ, Ho AW, et al. Assessment of
Columbia, 2199 Wesbrook Mall, Vancouver, BC, V6T 1Z3.
risk for periodontal disease. I. Risk indicators for attach-
ment loss. J Periodontol 1994;65:260-267.
25. Grossi SG, Genco RJ, Machtei EE, et al. Assessment of
Accepted for publication May 10, 1999.
risk for periodontal disease. II. Risk indicators for alve-olar bone loss. J Periodontol 1995;66:23-29.
26. Ah MKB, Johnson GK, Kaldahl WB, Patil KD, Kalkwarf
KL. The effect of smoking on the response to periodontaltherapy. J Clin Periodontol 1994;21:91-97.
NEWTOWN PUBLIC SCHOOLS CHECK RUN 06/07/2013 VENDOR NAME ACCOUNT DESCRIPTION DESCRIPTION CI-PA419 iPod Wireless PA System remainder of price. M-319 Califone Belt pack Transmitter. 371201 Total 371202 Total INSTALL BATHROOM DOOR LOCKS / DOOR REPAIRS - HOM 371203 Total 371204 Total LOCAL TRANSPORTATIONFOR SCHOOL YEAR 2012-13ST. ROSE TRANS - 29 BUSES FOR SCHOOL YEAR 2012-
TRAITEMENT MEDICAMENTEUX DE L’OSTEOPOROSE CORTISONIQUE – RECOMMANDATIONS – Recommandation de Bonne Pratique TRAITEMENT MEDICAMENTEUX DE L’OSTÉOPOROSE CORTISONIQUE RECOMMANDATIONS AGENCE FRANÇAISE DE SECURITE SANITAIRE DES PRODUITS DE SANTETRAITEMENT MEDICAMENTEUX DE L’OSTEOPOROSE CORTISONIQUE – RECOMMANDATIONS – GROUPE DE TRAVAIL Docteur Christian ROUX, Président
 9012_IPC_AAP_553060 2/15/00 11:02 AM Page 60
Oral Elastase in Smokers
9012_IPC_AAP_553060 2/15/00 11:02 AM Page 60
Oral Elastase in Smokers