Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Imperialendo.co.uk2
The Journal of Clinical Endocrinology & Metabolism 90(1):135–141
Copyright 2005 by The Endocrine Society
Cinacalcet Hydrochloride Maintains Long-Term Normocalcemia in Patients with Primary Hyperparathyroidism
Munro Peacock, John P. Bilezikian, Preston S. Klassen, Matthew D. Guo, Stewart A. Turner, andDolores Shoback
Department of Medicine (M.P.), Indiana University School of Medicine, Indianapolis, Indiana 46202; Department ofMedicine (J.P.B.), College of Physicians and Surgeons, Columbia University, New York, New York 10032; Amgen Inc. (P.S.K., M.D.G., S.A.T.), Thousand Oaks, California 91320; and Department of Veterans Affairs Medical Center (D.S.),Department of Medicine, University of California, San Francisco, California 94121Calcimimetics increase the sensitivity of parathyroid calci- chemistry, biochemical measures of bone turnover, bone min- um-sensing receptors to extracellular calcium, thereby reduc- eral density, and safety were also assessed. Seventy-three ing PTH secretion. This multicenter, randomized, double- percent of cinacalcet-treated patients vs. only 5% of placebo- blind, placebo-controlled study assessed the ability of the oral treated patients achieved the primary endpoint (P < 0.001). calcimimetic cinacalcet HCl to achieve long-term reductions Fasting predose plasma PTH decreased 7.6% in cinacalcet pa- in serum calcium and PTH concentrations in patients with tients but increased 7.7% in placebo patients (P < 0.01). Bone primary hyperparathyroidism (HPT). Patients (n ؍ 78) were mineral density was unchanged by cinacalcet, but bone re- randomized to cinacalcet or placebo. Cinacalcet was titrated sorption and formation markers increased (P < 0.05). Adverse from 30 –50 mg twice daily during a 12-wk dose-titration events were mild and similar between treatment groups. Ci- phase. Efficacy was assessed during 12-wk maintenance and nacalcet rapidly normalizes serum calcium and reduces PTH 28-wk follow-up phases. The primary endpoint was the in patients with primary HPT, and these effects are main- achievement of normocalcemia [serum calcium < 10.3 mg/dl tained with long-term treatment. Cinacalcet may be an effec- (2.57 mmol/liter)] with at least 0.5 mg/dl (0.12-mmol/liter) re- tive, nonsurgical approach for management of primary HPT. duction from baseline. Plasma PTH, serum and urine bio- (J Clin Endocrinol Metab 90: 135–141, 2005)
PRIMARY HYPERPARATHYROIDISM (HPT) is a com- calcet HCl, hereafter referred to as cinacalcet, is a calcimi-
mon disorder characterized by chronically elevated se-
metic that has been shown to lower plasma PTH, serum
rum calcium and PTH concentrations. In the United States,
calcium, and serum phosphorus in patients with secondary
many patients with primary HPT have mild, asymptomatic
HPT (6, 7). In an earlier study, we showed that cinacalcet also
disease and do not meet the criteria for surgery (1). Patients
had efficacy in the short-term reduction of serum calcium
with moderate to severe disease can experience worsening
and PTH concentrations in patients with primary HPT (8).
hypercalcemia, nephrolithiasis, loss of bone mineral density
We conducted this 52-wk, randomized, double-blind,
(BMD), neuromuscular weakness, and neurobehavioral
placebo-controlled study to investigate the long-term effi-
symptoms including easy fatigability and impaired cognitive
cacy and safety of cinacalcet in reducing serum calcium and
function (2). Parathyroidectomy is usually curative, but there
PTH levels in patients with mild to moderate primary HPT.
are few nonsurgical treatment alternatives for patients who
In addition, the impact of cinacalcet on bone turnover and
fail surgery, have contraindications to surgery, do not wish
to have surgery, or do not meet current guidelines for sur-gery. Thus, there is a need for therapeutic agents that directly
Patients and Methods
reduce serum calcium and PTH concentrations in patientswith primary HPT.
The calcium-sensing receptor (CaR) located on cells of the
The study was conducted at 18 centers in the United States. Seventy-
parathyroid gland is the principal regulator of PTH secretion
eight adult patients, 21 men and 57 women, aged 27– 83 yr, with primary
(3). Type II calcimimetics are a novel class of compounds that
HPT were enrolled in the study over 14 wk between 1999 and 2000. Eligibility requirements included serum calcium concentration greater
directly reduce PTH levels by binding to the CaR and in-
than 10.3 mg/dl (2.57 mmol/liter) and less than 12.5 mg/dl (3.12 mmol/
creasing its sensitivity to extracellular calcium (4, 5). Cina-
liter) and plasma PTH concentration greater than 45 pg/ml (4.73 pmol/liter). PTH was measured on at least two occasions at least 7 d apartduring the 12-month period before baseline. Exclusion criteria included
First Published Online November 2, 2004
pregnancy, creatinine clearance less than 50 ml/min (0.83 ml/sec) (9),
Abbreviations: BALP, Bone-specific alkaline phosphatase; BMD,
treatment with bisphosphonates or fluoride in the 90 d before baseline,
bone mineral density; CaR, calcium-sensing receptor; DPD, deoxypyr-
familial hypocalciuric hypercalcemia, or fasting urine calcium/creati-
idinoline; HPT, hyperparathyroidism; NTx, N-telopeptide.
nine in milligrams (molar) ratio less than 0.05 (0.14). Because cinacalcet
JCEM is published monthly by The Endocrine Society (http://www.
inhibits cytochrome P450 2D6 (CYP2D6), patients were excluded if they
endo-society.org), the foremost professional society serving the en-
required drugs that are metabolized by this enzyme and have a narrow
docrine community.
therapeutic index, such as flecainide, thioridazine, and many tricyclic
J Clin Endocrinol Metab, January 2005, 90(1):135–141
Peacock et al. • Cinacalcet for Primary Hyperparathyroidism
antidepressants. Women on stable doses of selective estrogen receptor
modulators or estrogen replacement therapy were eligible. The Insti-tutional Review Board at each center approved the study, and written
The proportion of patients achieving a serum calcium less than or
informed consent was obtained from all patients.
equal to 10.3 mg/dl (2.57 mmol/liter) and a reduction in serum calciumof at least 0.5 mg/dl (0.12 mmol/liter) from baseline was determinedusing mean values for each patient derived from up to three measure-
ments obtained during the maintenance phase. The difference in theproportion of patients achieving the primary endpoint in the cinacalcet
This was a multicenter, randomized, double-blind, placebo-con-
and placebo groups was determined using logistic regression and in-
trolled study. Patients were randomized in a 1:1 ratio to receive either
cluded all randomized patients. For this analysis, patients leaving the
cinacalcet or placebo after a 30-d screening period. The study included
study before the maintenance phase were considered not to have
a 12-wk dose-titration phase, a 12-wk maintenance phase during which
achieved the primary endpoint, regardless of serum calcium values at
the primary efficacy endpoint was measured, and a 28-wk follow-up
the time of withdrawal. An additional analysis was performed using the
phase to gather additional safety and efficacy information. Patients
last on-study serum calcium value for patients who withdrew before the
initially received 30 mg cinacalcet or placebo twice daily. The dose was
maintenance phase. Biochemical and BMD variables were compared
increased sequentially to 40 and 50 mg twice daily at study wk 4 and 8
between placebo and cinacalcet groups at wk 24 and 52 using one-way
if patients were still hypercalcemic (serum calcium Ͼ 10.3 mg/dl).
ANOVA. Adverse events were tabulated by treatment group and an-
Patient visits occurred weekly during the titration phase (wk 1–12) and
alyzed using descriptive statistics.
monthly during the maintenance (wk 13–24) and follow-up (wk 25–52)phases. Pharmacodynamic data were collected at wk 3, 12, and 24 after
the morning dose of study drug to assess effects of study drug on serumcalcium and PTH concentrations over 8 h.
A total of 78 patients with primary HPT were randomized
The primary endpoint was the proportion of patients achieving a
(40 cinacalcet, 38 placebo). One patient who was randomized
mean serum calcium less than or equal to 10.3 mg/dl (2.57 mmol/liter)and a reduction from baseline of at least 0.5 mg/dl (0.12 mmol/liter)
to placebo withdrew before receiving the study drug. The
during the maintenance phase. Secondary endpoints included changes
mean age was 62 yr in both groups (range, 27– 83 yr), and the
from baseline in serum and urine biochemistries and BMD. Adverse
majority of patients were women (70% cinacalcet, 76% pla-
events were recorded throughout the study.
cebo). Nine patients in each group had a prior history ofparathyroidectomy. Twenty-eight of 40 patients (70%) in the
cinacalcet group and 28 of 38 patients (74%) in the placebogroup completed the 52-wk study.
Blood samples were collected for measurement of serum calcium and
PTH at each study visit after an overnight fast and before the morning
Mean baseline biochemical values were similar between
dose of study drug. Samples for serum calcium and PTH were also
treatment groups and characteristic of patients with mild to
collected at 2, 4, and 8 h after the morning dose of study drug at wk 3,
moderate primary HPT (Table 1). In the cinacalcet group, the
12, and 24 for pharmacodynamic analysis. Serum calcium [coefficient of
mean baseline serum calcium level was 10.7 Ϯ 0.5 mg/dl
variation (CV) ϭ 1.4 –1.5%] was measured by standard methods. Intact
(2.67 Ϯ 0.12 mmol/liter), and the mean PTH level was 105 Ϯ
PTH (CV ϭ 4.2– 6.4%) was measured using a double-antibody immu-noradiometric assay (Allegro PTH, Nichols Institute Diagnostics, San
36 pg/ml (11.0 Ϯ 3.78 pmol/liter) compared with 10.7 Ϯ 0.4
mg/dl (2.67 Ϯ 0.10 mmol/liter) and 120 Ϯ 54 pg/ml (12.6 Ϯ
Serum phosphorus (CV ϭ 2.2–2.4%), creatinine (CV ϭ 1.6 –13.5%),
5.68 pmol/liter), respectively, in placebo-treated patients.
1,25-dihydroxyvitamin D (CV ϭ 9.1–20.3%), bone-specific alkaline phos-
Mean (sd) baseline Z scores for cinacalcet were 0.15 (2.20)
phatase (BALP) (CV ϭ 9.9 –11.4%), and N-telopeptide (NTx) (CV ϭ6.4 –9.5%) were measured at baseline and at wk 24 and 52. Serum 1,25-
at the lumbar spine, – 0.31 (0.91) at the total femur, and – 0.46
dihydroxyvitamin D was measured by radioreceptor assay (Endocrine
(1.41) at the 1/3 distal radius. For placebo patients, the base-
Sciences, Calabasas Hills, CA). Serum NTx levels were determined by
line Z scores were – 0.10 (2.27) at the lumbar spine, – 0.33
ELISA (Osteomark NTx assay, Ostex International, Seattle, WA). Urine
(0.96) at the total femur, and – 0.31 (1.38) at the 1/3 distal
was collected over 24 h and after an overnight fast at baseline and at wk
radius. Mean (sd) baseline T scores for the cinacalcet group
24 and 52 for the measurement of calcium (CV ϭ 3.4 – 4.9%), phosphorus(CV ϭ 1.7–1.9%), NTx (CV ϭ 5.1–11.3%), and deoxypyridinoline (DPD)
were – 0.90 (1.55) at the lumbar spine, –1.20 (1.02) at the total
(CV ϭ 8.6 –17.1%), which were expressed as a ratio with urine creatinine.
femur, and –1.61 (1.58) at the 1/3 distal radius. For placebo
Urine calcium, phosphorus, creatinine, and urine-free DPD were mea-
patients, the baseline T scores were –1.22 (1.57) at the lumbar
sured by Covance Central Laboratories (Indianapolis, IN). Tubular re-
spine, –1.32 (1.07) at the total femur, and –1.79 (1.62) at the
absorption of calcium (TmCa ϭ [total plasma calcium ϫ 0.59 – urinecalcium ϫ plasma creatinine/urine calcium]/1 – 0.08 log
calcium ϫ 0.59/{urine calcium ϫ plasma creatinine/urine calcium}])
During the maintenance phase, 73% of patients in the
and tubular reabsorption of phosphorus (TmP ϭ [plasma phosphate
cinacalcet group achieved the primary endpoint [predose
– urine phosphate ϫ plasma creatinine/urine phosphate]/1 – 0.1 loge
serum calcium Յ 10.3 mg/dl (2.57 mmol/liter) and a de-
[plasma phosphate/{urine phosphate ϫ plasma creatinine/urine phos-
crease from baseline of Ն0.5 mg/dl (0.12 mmol/liter)] com-
phate}]) were calculated from the calcium and phosphate (in milligrams)values in the respective fasting blood and urine samples using the
pared with 5% of the placebo group (P Ͻ 0.001). When serum
calcium values from patients who withdrew during the dose-
BMD of the lumbar spine, total femur, and 1/3 distal radius was
titration phase were included in the analysis, 88% of the
measured either by dual-energy x-ray absorptiometry at baseline and at
cinacalcet group achieved the primary endpoint, compared
wk 24 and 52 using a Hologic densitometer (Hologic, Waltham, MA)(n ϭ 27, cinacalcet; n ϭ 26, placebo) or a Lunar densitometer (Lunar Inc.,
with 5% of the placebo group (P Ͻ 0.001). Mean serum
Madison, WI) (n ϭ 13, cinacalcet; n ϭ 12, placebo). For each patient, BMD
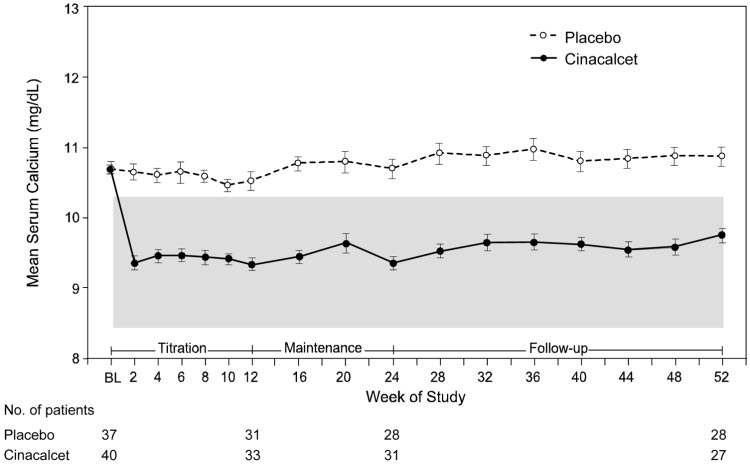
calcium levels were reduced to the normal range within the
was measured on the same densitometer throughout the study. To
first 2 wk of treatment with cinacalcet (Fig. 1) and remained
combine measurements in men and women over a wide age range made
normal throughout the 52 wk of the study. In the placebo
on either Hologic or Lunar machines, BMD was expressed as a Z score.
group, the mean serum calcium levels did not change sig-
To examine for longitudinal changes, the changes in Z score for eachindividual were calculated, and the mean changes for the placebo and
nificantly from baseline levels throughout the study.
cinacalcet groups were presented as mean change in Z score.
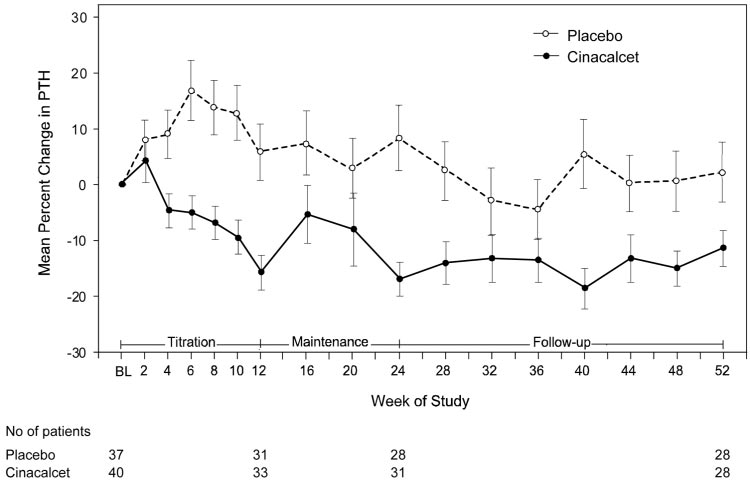
Corresponding modest but significant reductions in fast-
Peacock et al. • Cinacalcet for Primary Hyperparathyroidism
J Clin Endocrinol Metab, January 2005, 90(1):135–141
ing plasma PTH (measured ϳ12 h after administration of
study drug) were observed in the cinacalcet group. Mean
plasma predose PTH decreased by 7.6% from 105 Ϯ 36 pg/ml
Ϯ 3.78 pmol/liter) to 95 Ϯ 34 pg/ml (10.0 Ϯ 3.55 pmol/
liter) during the maintenance phase compared with a 7.7%increase from 120 Ϯ 54 to 127 Ϯ 53 pg/ml (12.6 Ϯ 5.69 to13.3
Ϯ 5.52 pmol/liter) in the placebo group (P Ͻ 0.01; Fig.
2). In the cinacalcet group, predose plasma PTH reductions
were maintained throughout the follow-up period.
Pharmacodynamic data collected at wk 24 demonstrated
that the serum calcium concentrations remained unchanged
after the morning dose of cinacalcet, whereas the correspond-
ing plasma PTH concentrations underwent cyclic changeswith dosing. At wk 24, mean serum calcium was normal,
whereas mean plasma PTH remained elevated at the predose
measurement. After the morning dose of cinacalcet, serum
calcium was unchanged at all time points measured (Fig. 3A),
whereas PTH decreased by 37% into the normal range at 2 h
after dose (P Ͻ 0.0001) and gradually returned toward pre-
dose levels by 8 h (Fig. 3B). In the placebo group, no changes
in calcium or PTH concentrations were observed over thecorresponding time period. Results were similar at wk 3 and
12 (data not shown), indicating that no changes in serum
calcium occurred once steady state had been achieved,
but plasma PTH continued to undergo pharmacodynamic
Mean fasting predose biochemistries at baseline and at wk
24 and 52 are shown in Table 1. Serum phosphorus increasedin the cinacalcet group and at wk 52 was higher (P Ͻ 0.001)
than in the placebo group. The fasting urine calcium-creat-
inine ratio and the 24-h urine calcium-creatinine ratio de-
creased in the cinacalcet group, although the difference be-
tween treatment groups was statistically significant only for
the fasting calcium-creatinine ratio (P
tubular reabsorption of calcium decreased (P
phosphorus reabsorption increased (P Ͻ 0.001) from baseline
in the cinacalcet group, whereas there were no changes in the
placebo group. Serum 1,25-dihydroxyvitamin D concentra-
tions were similar in both groups at wk 52 and unchanged
from baseline. Serum creatinine and 24-h urine creatinine
remained relatively constant and similar in both groups
Some markers of bone turnover—serum BALP, serum
NTx, and the urine NTx-creatinine ratio—were increased
(P Ͻ 0.05) at wk 52 in the cinacalcet group compared with
placebo, but remained in the normal range. The urine DPD-
creatinine ratio increased in the cinacalcet group, but at wk
52, it was not significantly higher than in the placebo group.
In the placebo group, there was no significant change in any
of the biochemical markers of bone turnover during the
BMD was measured at baseline and at wk 24 and 52 and
expressed as a Z score. In general, few differences in mean
change in Z score occurred between the cinacalcet and pla-
cebo groups after 24 or 52 wk of treatment. At wk 24, the
mean change in Z score at the lumbar spine was significantly
lower in the cinacalcet group compared with the placebo
group (P Ͻ 0.05) (Table 2); however, no difference between
groups was observed at wk 52. No other significant differ-
ences for the lumbar spine, total femur, or 1/3 distal radius
J Clin Endocrinol Metab, January 2005, 90(1):135–141
Peacock et al. • Cinacalcet for Primary Hyperparathyroidism
FIG. 1. Comparison of predose serumcalcium concentrations in patients re-ceiving cinacalcet or placebo. The nor-mal serum calcium concentration range(8.4 –10.3 mg/dl) is indicated by theshaded area. Patients receiving cinacal-cet experienced a significant reductionin serum calcium compared with pa-tients
0.001). BL, Baseline value. Data arepresented as mean Ϯ SE.
at wk 24 or 52 were observed between treatment groups
lyzed separately for these patients, the data were not differ-
ent from the treatment groups as a whole (data not shown).
Nine patients in each treatment group (23% of the study
Cinacalcet was well tolerated in this study, and occurrence
population) had previously undergone unsuccessful para-
of adverse events was similar between treatment groups. The
thyroidectomy. Seven of these patients in the cinacalcet
two most common adverse events were nausea (28% cina-
group normalized their serum calcium and achieved the
calcet, 16% placebo) and headache (23% cinacalcet, 41% pla-
primary outcome, compared with one patient in the placebo
cebo). Similar numbers of patients in each group withdrew
group. In the cinacalcet group, mean serum calcium de-
from the study because of adverse events (eight cinacalcet,
creased from 10.8 mg/dl (2.70 mmol/liter) at baseline to 9.5
six placebo). Three of these patients from the cinacalcet group
mg/dl (2.38 mmol/liter) at wk 52. In placebo-treated patients
experienced serum calcium levels less than 8.0 mg/dl (2.00
who had previous parathyroidectomy, serum calcium re-
mmol/liter) while receiving the lowest dose of study drug
mained at baseline levels [11.1 mg/dl (2.78 mmol/liter)]
and, in accordance with the study protocol, were withdrawn
throughout the study. PTH levels decreased by 10.5% in
from the study. Two cinacalcet-treated patients experienced
cinacalcet-treated patients with a previous parathyroidec-
mild paresthesias that were considered treatment related.
tomy and increased 3.1% in placebo-treated patients with
Serum calcium values were 7.9 mg/dl (1.98 mmol/liter) in
previous parathyroidectomy. When BMD data were ana-
the three patients who withdrew because of asymptomatic
FIG. 2. Comparison of percent changeof predose plasma PTH concentrationsin patients receiving cinacalcet or pla-cebo. Patients receiving cinacalcet ex-perienced a 7.6% reduction in plasmaPTH compared with a 7.7% increase inthe placebo group (P Ͻ 0.01) duringthe maintenance phase. BL, Baselinevalue. Data are presented as mean Ϯ SE.
Peacock et al. • Cinacalcet for Primary Hyperparathyroidism
J Clin Endocrinol Metab, January 2005, 90(1):135–141
ous short-term study (15 d plus a 7-d follow-up) that showedcinacalcet is effective in reducing serum calcium in patientswith primary HPT (8). During the maintenance phase, 73%of cinacalcet-treated patients achieved normocalcemia witha decrease of at least 0.5 mg/ml (0.12 mmol/liter) frombaseline, whereas only 5% of placebo-treated patientsachieved this target. The proportion increased to 88% in thecinacalcet group compared with 5% in the placebo groupwhen serum calcium values for patients who withdrew be-fore the maintenance phase were included. In 90% of pa-tients, the lowest dose of cinacalcet, 30 mg twice daily, wassufficient to induce normocalcemia, and no patients requiredtitration to the maximum permitted dose of 50 mg twicedaily.
During the maintenance phase, predose plasma PTH con-
centrations were reduced by approximately 8% with cina-calcet treatment. It should be noted that this value, whichreflects hormone concentration before the morning dose ofcinacalcet, underestimates PTH reduction over 24 h. At wk24, pharmacodynamic data demonstrated that plasma PTHconcentration 2 h after dosing decreased into the normalrange (Fig. 3B), corresponding to a 60% reduction from base-line. Assuming that the decrease in PTH after the eveningdose was similar to that after the morning dose, the areaunder the curve indicates that there was an approximately20% reduction in plasma PTH over each 24-h cycle. Further-more, there was no indication from the pharmacodynamicdata that this response changed with length of time on drug.
FIG. 3. Response to cinacalcet or placebo before (0), and at 2, 4, and
In contrast to the cyclic change seen in PTH, serum calcium
8 h after the morning dose for serum calcium (A) and plasma PTH (B).
remained unchanged over the 8-h sampling period after the
Data were collected at wk 24. The normal ranges for serum calcium(8.4 –10.3 mg/dl) and plasma PTH (10 – 65 pg/ml) are indicated by the
morning dose of cinacalcet. These serum calcium results
shaded areas. BL, Baseline value. Data are presented as mean Ϯ SE.
indicate that once steady state has been achieved, no sharpdeclines in serum calcium occur after individual doses; thus
hypocalcemia and 7.8 mg/dl (1.95 mmol/liter) and 8.1
the risk of acute hypocalcemia and accompanying symptoms
mg/dl (2.02 mmol/liter) in the patients who experienced
appears to be avoided with twice-daily dosing with cinacal-
Drugs to manage the hypercalcemia of primary HPT, such
Discussion
as estrogens, selective estrogen receptor modulators, and
In this study, cinacalcet administered twice daily rapidly
bisphosphonates, have shown a limited ability to treat the
normalized predose serum calcium in the majority of pa-
disorder (11–14). These agents act primarily by inhibiting
tients and caused modest reductions in predose PTH con-
bone resorption, although their effects on serum calcium are
centrations in patients with mild to moderate primary HPT.
relatively small. Cinacalcet treatment was highly effective in
The effect of cinacalcet was sustained over 52 wk with no
reducing serum calcium levels in this study, and suppression
evidence of fluctuations in serum calcium concentration after
was maintained during 1 yr of treatment, suggesting that
individual doses once steady state had been established.
cinacalcet may be an important therapeutic agent for man-
These results confirm and extend the findings of our previ-
aging primary HPT, particularly when parathyroidectomy isnot a viable option. Indeed, nine patients in each group (23%
TABLE 2. Mean change in Z score from baseline at wk 24 and 52
of the study population) had previously undergone unsuc-cessful parathyroidectomy. Seven of these patients in the
cinacalcet group normalized their serum calcium and
achieved the primary outcome, compared with one patient
in the placebo group. Although this study did not include
patients with severe primary HPT or parathyroid carcinoma,
our preliminary reports indicate that cinacalcet may also
successfully reduce serum calcium in these patients (15, 16).
In addition to normalizing serum calcium, cinacalcet treat-
ment increased serum phosphorus. By wk 12, serum phos-phorus levels and tubular reabsorption of phosphorus had
increased, and the fasting urine calcium-creatinine ratio and
ϭ 0.023 for change in cinacalcet compared with change in
tubular reabsorption of calcium had decreased in the cina-
J Clin Endocrinol Metab, January 2005, 90(1):135–141
Peacock et al. • Cinacalcet for Primary Hyperparathyroidism
calcet group, probably reflecting the renal effect of the overall
wise asymptomatic mild hypercalcemia, and what the choice
decrease in plasma PTH over a 24-h cycle of dosing. The
of such therapy should be, require additional study before a
observation that serum calcium and tubular reabsorption of
change from the current management of watchful waiting
calcium were normal while predose PTH levels remained
elevated suggests that cinacalcet, in addition to its effects on
In conclusion, in these patients with primary HPT, cina-
PTH secretion, also alters the relationship between PTH and
calcet was highly effective in normalizing serum calcium
its action on tubular calcium reabsorption. In kidney, this
levels and reducing PTH, and this effect was maintained over
could be through a shift in the dose-response curve of PTH
long-term administration. The drug was well tolerated and
on tubular calcium reabsorption and/or by a direct effect of
may provide a valuable and effective management option for
cinacalcet on the CaR in the renal tubule. The decrease in
fasting urine calcium excretion was not accompanied by acorresponding significant decrease in 24-h calcium excretion. Acknowledgments
Because 24-h urine calcium has a component from intestinalabsorption of calcium, this lack of decrease is consistent with
Received May 7, 2004. Accepted October 25, 2004.
the finding that the predose serum 1,25-dihydroxyvitamin D
Address all correspondence and requests for reprints to: Munro Pea-
levels were not altered by cinacalcet.
cock, M.D., Director, General Clinical Research Center, University Hos-
Bone turnover may be increased in primary HPT. In our
pital, 550 University Boulevard, UH5595, Indianapolis, Indiana 46202.
HPT patients, the biochemical markers of bone turnover for
This study was sponsored by Amgen Inc.
the group were in the normal range at baseline, reflecting the
The following primary investigators also participated in the 990120
relative mildness of the disease. After treatment, some bone
Study: M. Block (Phoenix, AZ), M. Bolognese (Bethesda, MD), B. Esayag-
turnover markers significantly increased in the cinacalcet
Tendler (Farmington, CT), A. Firek (Loma Linda, CT), W. Greth (West
group, although the mean value remained in the normal
Reading, PA), H. Katzeff (New Hyde Park, NY), M. Kipnes (San Antonio,
range. The increase in bone turnover markers is of interest
TX), R. Lang (Hamden, CT), R. Levy (Olympia, WA), R. Marcus (PaloAlto, CA), R. Rude (Los Angeles, CA), S. Scumpia (Austin, TX), S.
because it occurred in conjunction with an overall decrease
Silverman (Beverly Hills, CA), F. Singer (Santa Monica, CA), R. Small-
of approximately 20% in plasma PTH levels. A possible ex-
ridge (Jacksonville, FL), J. Tucci (Providence, RI), and S. Wallach (New
planation is the effect of daily fluctuating plasma PTH levels
on bone turnover induced by the twice-daily dosing of ci-nacalcet, because it is known that daily injected PTH (1–34)
References
has a stimulatory effect on bone turnover (17). A direct effect
1. Bilezikian JP, Potts Jr JT, Fuleihan G-H, Kleerekoper M, Neer R, Peacock M,
of cinacalcet on bone turnover cannot be excluded, however,
Rastad J, Silverberg SJ, Udelsman R, Wells SA 2002 Summary statement from
and additional studies will be needed in this area.
a workshop on asymptomatic primary hyperparathyroidism: a perspective for
In our patients, spine BMD was normal, but hip and fore-
the 21st century. J Bone Miner Res 17:N2–N11
2. Chan AK, Duh QY, Katz MH, Siperstein AE, Clark OH 1995 Clinical man-
arm BMDs were in the osteopenic range, as expected in
ifestations of primary hyperparathyroidism before and after parathyroidec-
patients with this degree of primary hyperparathyroidism.
tomy. A case-control study. Ann Surg 222:402– 412
Over the 52 wk of the study, no clinically significant differ-
3. Brown EM, Gamba G, Riccardi D, Lombardi M, Butters R, Kifor O, Sun A, Hediger MA, Lytton J, Hebert SC 1993 Cloning and characterization of an
ences in change in BMD were observed between the cina-
extracellular Ca(2ϩ)-sensing receptor from bovine parathyroid. Nature 366:
4. Nemeth EF, Steffey ME, Hammerland LG, Hung BC, Van Wagenen BC,
Cinacalcet was well tolerated in this study. Occurrences of
DelMar EG, Balandrin MF 1998 Calcimimetics with potent and selective
adverse events and treatment-related adverse events were sim-
activity on the parathyroid calcium receptor. Proc Natl Acad Sci USA 95:
ilar between the placebo and cinacalcet groups. Adverse events
5. Nemeth EF, Fox J 1999 Calcimimetic compounds: a direct approach to con-
reported during the study were generally mild or moderate and
trolling plasma levels of parathyroid hormone in hyperparathyroidism.
resulted in only a small number of withdrawals.
The comparative utility and cost-benefit between cinacal-
6. Lindberg JS, Moe SM, Goodman WG, Coburn JW, Sprague SM, Liu W, Blaisdell PW, Brenner RM, Turner SA, Martin KJ 2003 The calcimimetic AMG
cet and parathyroidectomy as treatment modalities for pri-
073 reduces parathyroid hormone and calcium x phosphorus in secondary
mary HPT have yet to be established. Although parathy-
hyperparathyroidism. Kidney Int 63:248 –254
7. Quarles LD, Sherrard DJ, Adler S, Rosansky SJ, McCary LC, Liu W, Turner
roidectomy is usually curative and reverses abnormal
SA, Bushinsky DA 2003 The calcimimetic AMG 073 as a potential treatment
biochemistry and symptoms, there is a pressing need for
for secondary hyperparathyroidism of end-stage renal disease. J Am Soc Neph-
medical therapy to normalize serum calcium in patients who
8. Shoback DM, Bilezikian JP, Turner SA, McCary LC, Guo MD, Peacock M
have either a contraindication to or have failed parathyroid-
2003 The calcimimetic cinacalcet normalizes serum calcium in subjects with
ectomy. Disease severity in this study ranged from symp-
primary hyperparathyroidism. J Clin Endocrinol Metab 88:5644 –5649
tomatic, with 18 of the 79 patients having previously had a
9. Cockcroft DW, Gault MH 1976 Prediction of creatinine clearance from serum
failed parathyroidectomy, to asymptomatic. In patients who
10. Peacock M 2002 Primary hyperparathyroidism and the kidney: biochemical
had symptoms, had a failed parathyroidectomy, or who were
and clinical spectrum. J Bone Miner Res 17:N87–N94
11. Selby PL, Peacock M 1996 Ethinyl estradiol and norethindrone in the treat-
apparently asymptomatic, cinacalcet was equally effective in
ment of primary hyperparathyroidism in postmenopausal women. N Engl
normalizing serum calcium. Although mild primary HPT
with no apparent symptoms is currently managed by regular
12. Rubin MR, Lee KH, McMahon DJ, Silverberg SJ 2003 Raloxifene lowers
serum calcium and markers of bone turnover in postmenopausal women with
medical follow-up, i.e. watchful waiting, the long-term ef-
primary hyperparathyroidism. J Clin Endocrinol Metab 88:1174 –1178
fects of mild hyperparathyroidism (18, 19) and hypercalce-
13. Reasner CA, Stone MD, Hosking DJ, Ballah A, Mundy GR 1993 Acute
mia (20) on increasing premature cardiovascular death is of
changes in calcium homeostasis during treatment of primary hyperparathy-roidism with risedronate. J Clin Endocrinol Metab 77:1067–1071
concern. Whether therapy should be considered for other-
14. Chow CC, Chan WB, Li JK, Chan NN, Chan MH, Ko GT, Lo KW, Cockram
Peacock et al. • Cinacalcet for Primary Hyperparathyroidism
J Clin Endocrinol Metab, January 2005, 90(1):135–141
CS 2003 Oral alendronate increases bone mineral density in postmenopausal
2001 Effect of parathyroid hormone (1–34) on fractures and bone mineral
women with primary hyperparathyroidism. J Clin Endocrinol Metab 88:581–
density in postmenopausal women with osteoporosis. N Engl J Med 334:1434 –
15. Peacock M 2002 Normalization of hypercalcemia with calcimimetic AMG 073
18. Lundgren E, Lind L, Palmer M, Jakobsson S, Ljunghall S, Rastad J 2001
in a patient with metastatic parathyroid cancer. J Bone Miner Res 17:S381
Increased cardiovascular mortality and normalized serum calcium in patients
16. Silverberg SJ, Faiman JP, Bilezikian JP, Shoback DM, Rubin MR, McCary
with mild hypercalcemia followed up for 25 years. Surgery 130:978 –985
LC, Olson KA, Turner SA, Peacock M 2003 The effects of cinacalcet HCl (AMG
19. Nilsson IL, Yin L, Lundgren E, Rastad J, Ekbom A 2002 Clinical presen-
073) on serum calcium levels in patients with parathyroid carcinoma or re-
tation of primary hyperparathyroidism in Europe–nationwide cohort anal-
current primary hyperparathyroidism after parathyroidectomy. J Bone Miner
ysis on mortality from nonmalignant causes. J Bone Miner Res 17(Suppl
17. Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, Reginster JY,
20. Leifsson BG, Ahren B 1996 Serum calcium and survival in a large health Hodsman AB, Eriksen EF, Ish-Shalom S, Genant HK, Wang O, Mitlak BH
screening program. J Clin Endocrinol Metab 81:2149 –2153
JCEM is published monthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving the endocrine community.
Shyam-Vidya Ayurved P.G. Entrance Coaching Center, Bhopal (M.P.) Hyderabad PG - 2009 By- Dr. Neelima Singh (M.D.) Mob. 09993961427, 09826438399 (1) According to Caraka which mahabootha is not necessary in punarjanam - (A) Akas (B) Vayu (C) Agni (D) Pruthvi (2) Which is Auloukya darsana - (A) Nyaya (B) Vaisheshik (C) Sankhya (D)Yoga (3) Bhoomika of Chitta is (A) Anu (
REGISTER 2006 HANDBOKEN Bevara och förnya en äldre trädgård 04/61Höststicklingar – ett lönsamt gratisnöje 14/61Julens alla blommor – levande pynt inne och ute 15/06Kom ihåg i februari – inomhus/i västhuset/i trädgården/i förrådet/källaren 02/06Kom ihåg i mars – i trädgården – inomhus 03/06Litet köksland – lättodlat och ätbart 07/75Orkidéer – från ly
 J Clin Endocrinol Metab, January 2005, 90(1):135–141
Peacock et al. • Cinacalcet for Primary Hyperparathyroidism
FIG. 1. Comparison of predose serumcalcium concentrations in patients re-ceiving cinacalcet or placebo. The nor-mal serum calcium concentration range(8.4 –10.3 mg/dl) is indicated by theshaded area. Patients receiving cinacal-cet experienced a significant reductionin serum calcium compared with pa-tients
0.001). BL, Baseline value. Data arepresented as mean Ϯ SE.
J Clin Endocrinol Metab, January 2005, 90(1):135–141
Peacock et al. • Cinacalcet for Primary Hyperparathyroidism
FIG. 1. Comparison of predose serumcalcium concentrations in patients re-ceiving cinacalcet or placebo. The nor-mal serum calcium concentration range(8.4 –10.3 mg/dl) is indicated by theshaded area. Patients receiving cinacal-cet experienced a significant reductionin serum calcium compared with pa-tients
0.001). BL, Baseline value. Data arepresented as mean Ϯ SE.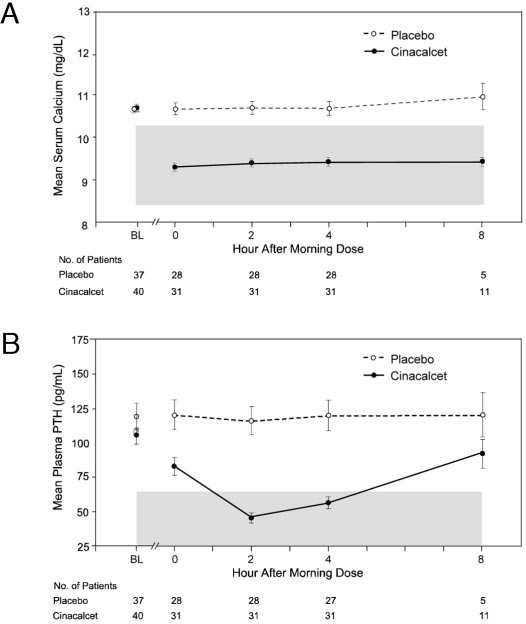 Peacock et al. • Cinacalcet for Primary Hyperparathyroidism
J Clin Endocrinol Metab, January 2005, 90(1):135–141
ous short-term study (15 d plus a 7-d follow-up) that showedcinacalcet is effective in reducing serum calcium in patientswith primary HPT (8). During the maintenance phase, 73%of cinacalcet-treated patients achieved normocalcemia witha decrease of at least 0.5 mg/ml (0.12 mmol/liter) frombaseline, whereas only 5% of placebo-treated patientsachieved this target. The proportion increased to 88% in thecinacalcet group compared with 5% in the placebo groupwhen serum calcium values for patients who withdrew be-fore the maintenance phase were included. In 90% of pa-tients, the lowest dose of cinacalcet, 30 mg twice daily, wassufficient to induce normocalcemia, and no patients requiredtitration to the maximum permitted dose of 50 mg twicedaily.
Peacock et al. • Cinacalcet for Primary Hyperparathyroidism
J Clin Endocrinol Metab, January 2005, 90(1):135–141
ous short-term study (15 d plus a 7-d follow-up) that showedcinacalcet is effective in reducing serum calcium in patientswith primary HPT (8). During the maintenance phase, 73%of cinacalcet-treated patients achieved normocalcemia witha decrease of at least 0.5 mg/ml (0.12 mmol/liter) frombaseline, whereas only 5% of placebo-treated patientsachieved this target. The proportion increased to 88% in thecinacalcet group compared with 5% in the placebo groupwhen serum calcium values for patients who withdrew be-fore the maintenance phase were included. In 90% of pa-tients, the lowest dose of cinacalcet, 30 mg twice daily, wassufficient to induce normocalcemia, and no patients requiredtitration to the maximum permitted dose of 50 mg twicedaily.