Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Imap.victorherbert.com
C l i n i c a l C a r e / E d u c a t i o n / N u t r i t i o n O R I G I N A L A R T I C L E Increased Intake of Calcium Reverses Vitamin B Malabsorption Induced by Metformin WILLIAM A. BAUMAN, MD ANN M. SPUNGEN, EDD SPENCER SHAW, MD VICTOR HERBERT, MD, JD ELIZABETH JAYATILLEKE, MS
in vitamin B absorption because of altered
RESEARCH DESIGN AND METHODS OBJECTIVE — Of patients who are prescribed metformin, 10–30% have evidence of reduced vitamin B absorption. B -intrinsic factor complex uptake by ileal cell surface recep-
tors is known to be a process dependent on calcium availability. Metformin affects calcium-
dependent membrane action. The objective of this study was to determine the magnitude and
mechanism of the reduction in serum vitamin B after metformin administration.
an oral sulfonylurea and followed as out-
RESEARCH DESIGN AND METHODS — A comparative study design was employed
patients in the diabetes clinic of the Veter-
using 2 groups (metformin and control). A total of 21 patients with type 2 diabetes received
sulfonylurea therapy; 14 of these 21 patients were switched to metformin. Monthly serum total
York, were recruited for study. The subjects’
measurements and holotranscobalamin (holoTCII) (B -TCII) were performed.
ages were restricted to 30–60 years.
After 3 months of metformin therapy, oral calcium supplementation was administered.
Patients were excluded if they had a historyof alcoholism or other drug abuse, psychi-
RESULTS — Serial serum vitamin B determinations revealed a similar decline in vitamin
atric disease, chronic renal failure, liver dis-
and holoTCII. Oral calcium supplementation reversed the metformin-induced serum
ease, cardiopulmonary disease, pernicious
CONCLUSIONS — Patients receiving metformin have diminished B absorption and low
disease, acid-based disturbance, or cancer,
serum total vitamin B and TCII-B levels because of a calcium-dependent ileal membrane
or if they were receiving antibiotics or any
antagonism, an effect reversed with supplemental calcium.
medications known to influence gastroin-testinal motility. An initial blood sample
Diabetes Care 23:1227–1231, 2000
was obtained to exclude the possibility ofoccult preexisting vitamin B
Metformin, a disubstituted biguanide, exhibit alterations in small bowel motility as [B -TCII]Ͻ50 pg/ml or serum total
well as bacterial overgrowth (5–6). It may
(1). Approximately 10%, but in some stud-
alter bacterial flora through an effect on
excluded; however, none was identified.
ies up to 30%, of patients taking metformin
motility and/or facilitation of bacterial
reduced vitamin B absorption (2–4). The
(4). Alternatively, metformin is known to
their sulfonylurea preparation to metformin;
effect has been unclear and, therefore, a
brane action (7). Of note, B -intrinsic factor
entrance into the study by placing 2 subjects
(IF) complex uptake by the ileal cell surface
on metformin and 1 remaining on his or her
receptor is known to be calcium dependent
sulfonylurea, and so forth. Thus, 7 patients
(8). Some investigators have demonstrated a
continued to receive their usual sulfony-
enhanced bacterial overgrowth, especially
direct effect on B absorption in the absence
lurea preparation and served as control sub-
of any apparent bacterial overgrowth (2,3).
jects. Subjects in the experimental andcontrol groups were men of similar age (48.6± 10.1 vs. 54.0 ± 4.9 years, NS) (Table 1)
From the Department of Medicine (W.A.B., S.S., A.M.S., V.H.), Mount Sinai School of Medicine, New York;
and proportionally similar ethnic distribu-
and the Medical Service (W.A.B., S.S., E.J., V.H.), Veterans Affairs Medical Center, Bronx, New York.
tion (metformin group: 3 white, 4 Hispanic,
Address correspondence and reprint requests to William A. Bauman, MD, Director, Research Center Rm.
1E-02, Veterans Affairs Medical Center, 130 W. Kingsbridge Rd., Bronx, NY 10468. E-mail:
7 African-American; control group: 1 white,
4 Hispanic, 2 African-American), duration
Received for publication 17 November 1999 and accepted in revised form 6 June 2000.
of diabetes (6.9 ± 6.1 vs. 6.0 ± 3.6 years),
Abbreviations: CBC, complete blood count; holoTCII, holotranscobalamin; IF, intrinsic factor; MCTT,
and initial serum total vitamin B levels.
mouth-to-cecum transit time; TC, transcobalamin.
A table elsewhere in this issue shows conventional and Système International (SI) units and conversion
physical examination. Baseline laboratory
DIABETES CARE, VOLUME 23, NUMBER 9, SEPTEMBER 2000
Metformin reduces vitamin B absorption 12
body weights were performed at baselineand 6 months in the metformin-treatedand sulfonylurea-treated groups.
Sample analysisBlood samples obtained as part of the clini-cal evaluation of metformin-treated and con-trol (sulfonylurea-treated) subjects wereanalyzed for total and holoTCII-B . After
separation, serum samples were frozenimmediately at Ϫ20°C until assayed (Simul-TRAC; Becton Dickinson, Orangeberg, NY). Vitamin B
assayed by differential radioassay accordingto the modification by Kolhouse et al. (9) ofthe method of Lau et al. (10) using purifiedIF to measure cobalamin and R-binder tomeasure total corrinoids (9,10). The analogsare measured by the difference between the2 assays; elevated levels of the analogs indi-cate bacterial overgrowth of the small intes-tine, except in rare cases of ingestion of theanalogs themselves from alternative medi-cine sources, e.g., herbs, algae, or seaweed.
ing the difference between serum total vita-min B and B remaining after absorption
onto microfine silica, as previously described(11). HoloTCII levels fall when absorptionof B is reduced, regardless of the etiology of
the decreased B absorption (11–15).
Hydrogen breath testsTo ascertain bacterial overgrowth, a lactu-lose-stimulated hydrogen breath analysiswas performed in patients before enroll-ment and after 4 months of treatment in the
experimental or control groups. A Quintron
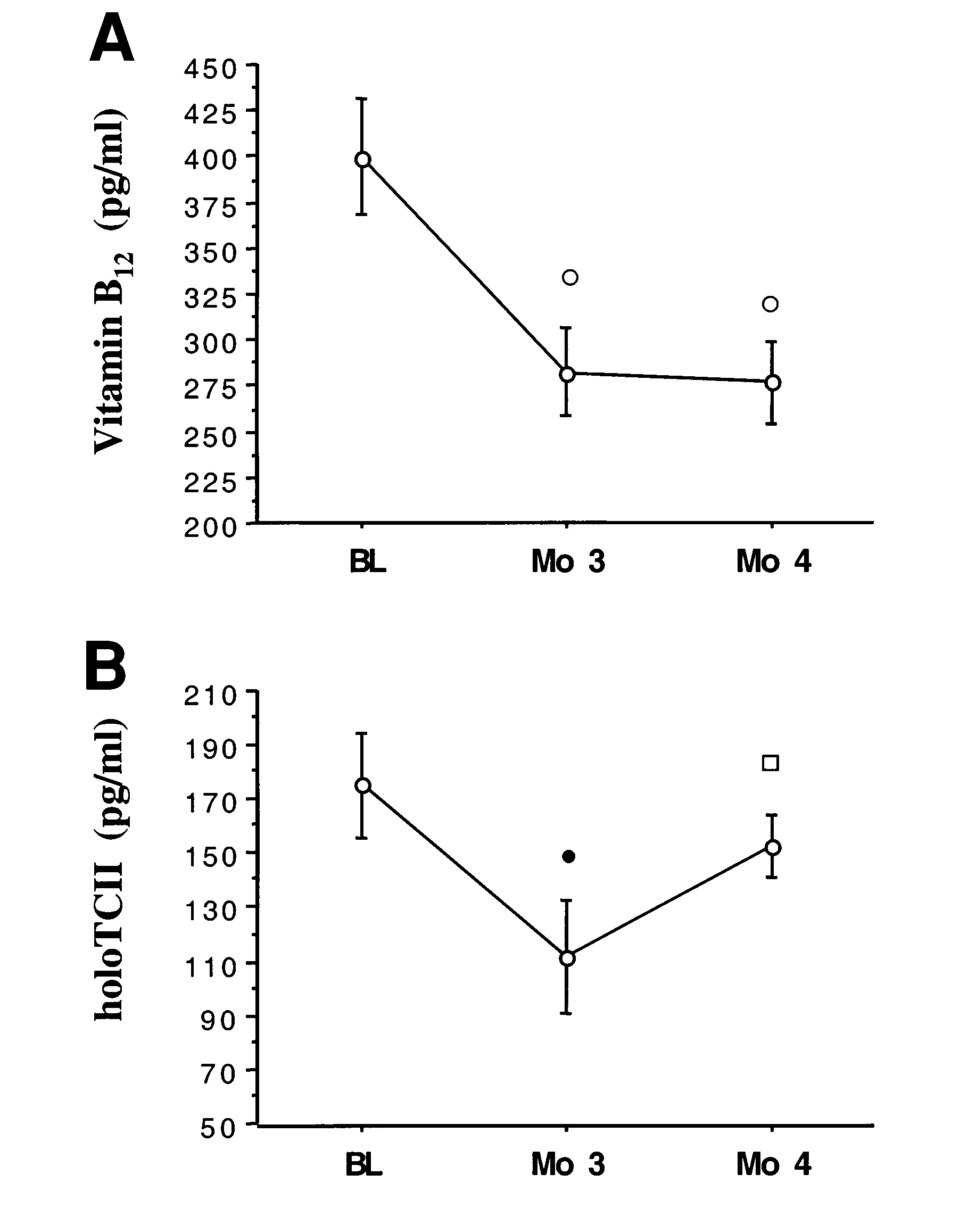
Metformin-treated subjects for serum total vitamin B (A) and serum holoTCII (B). ᭺, P
Ͻ 0.0005 between baseline and month 3 or month 4; ᭹, P Ͻ 0.01 between baseline and month 3; ᮀ,
P Ͻ 0.005 between month 3 and month 4. Vertical bars indicate SEM.
overnight fast, a baseline hydrogen breathtest was obtained before and after adminis-tration of 10 g lactulose in 100 ml water. Readings were taken every 10 min for 2 h.
chemistries (electrolytes, renal function,
increased early peak, was considered con-
and liver function tests), complete blood
sistent with small intestinal bacterial over-
count (CBC), serum folate, and lactate. A
taken to indicate slowed intestinal transit.
weekly intervals for the first month and at
Serum folate levels were determined by com-
months of metformin therapy, oral calcium
petitive inhibition radioassay using a com-
at 850 mg/day for 2 weeks. Almost all sub-
carbonate (1.2 g/day) was administered to
the metformin group alone for 1 month.
and lactate determinations were performed
during the initial treatment period. How-
on an automated Glucose-Lactate Analyzer II
ever, the dose of medication was titrated
(Yellow Springs Instruments, Yellow Springs,
states of small-bowel bacterial overgrowth.
clinical laboratory using high-performance
Serum lactate and glucose were drawn with
DIABETES CARE, VOLUME 23, NUMBER 9, SEPTEMBER 2000
Bauman and Associates Table 1—Subject characteristics
The dependent variables (serum total vita-min B and holoTCII) were analyzed for the
between-group comparisons (control vs. metformin) by using an unpaired t test and
a multiple regression analysis. A nonpara-
metric test (Mann-Whitney U test) was used
to determine the difference in the distribu-
groups for the percent change from baseline
Data are n or means ± SEM. Control subjects continued on sulfonylurea therapy.
to month 3 in the holoTCII levels. Theresults are reported as means ± SEM. Within
formin-treated group had lower serum total
the control and metformin groups, compar-
B (Ϫ61 ± 19 pg/ml, P Ͻ 0.005) than the
1.9 vs. 9.1 ± 2.0%, P Ͻ 0.05). In the con-
isons were performed using a repeated-mea-
control group. Significantly more subjects in
trol (sulfonylurea-treated) group, no sig-
nificant difference in HbA was found (8.7
significance of differences for the baseline,
jects in the control group (P Ͻ 0.05).
developed lactic acidosis that mandatedwithdrawal from the study. From baseline
in the control group (190 ± 45 vs. 187 ±
43 lb., NS) but significantly fell in the met-
committee as well as the subcommittees on
bonate (Tums, 1.2 g/day) in the metformin-
formin group (232 ± 31 vs. 222 ± 28 lb.,
decreased serum holoTCII levels. Theserum holoTCII increased from 111 ± 21 to
CONCLUSIONS — Because ileal vita-
153 ± 11 pg/ml—a 53 ± 15% increase after
process, in our study, patients with type 2
month 4 (P Ͻ 0.005; Fig. 1B)—but the
serum total vitamin B level did not change
chemistries (electrolytes, renal function,
metformin. A fall in serum total vitamin B12
and liver function tests), CBC, and serum
lactate were within normal limits for all
has a half-life of 6 min and, as such, is
No patient had evidence of bacterial over-
growth before or at the conclusion of the
(11,15,16). In the normal adult, ϳ80% of
were not significantly different between the
hydrogen breath tests. The concentrations
(formerly called transcobalamin [TC] I and
of the serum B analogs were variable. After
4 months of therapy, they were not signifi-
protein with a half-life of 2 weeks and with
Throughout the course of the study, no sig-
cantly different from baseline in either the
cell surface receptors only on reticuloen-
dothelial storage cells (15,16). We further
noted in the control group at baseline, 3
group: 142 ± 60 vs. 126 ± 101 pg/ml; con-
months, or 4 months (335 ± 45 vs. 364 ±
trol group: 188 ± 44 vs. 101 ± 78 pg/ml;
51 vs. 375 ± 90 pg/ml, NS). After 3 months
baseline vs. 4 month values, respectively),
supplementation. A potential limitation of
of metformin therapy, subjects in this group
also suggesting that bacterial overgrowth
this study was that the enrollment of sub-
serum total vitamin B (400 ± 32 vs. 282 ±
months, serum folate levels were not signifi-
24 pg/ml, P Ͻ 0.0005) (Fig. 1A) and
cantly different from baseline values (met-
holoTCII (175 ± 19 vs. 111 ± 21 pg/ml, P
formin group: 8.8 ± 3.3 vs. 7.8 ± 2.8 vs. 7.0
Ͻ 0.01) (Fig. 1B). Of the 14 subjects receiv- ± 1.8 pg/ml; control group: 8.7 ± 1.9 vs. 9.6 such as metformin, extends into the hydro-ing metformin, with the exception of 2 sub-
± 4.9 vs. 8.6 ± 1.3 pg/ml; baseline vs. 3-
jects who had a slight increase, 12 subjects
had a fall in serum total vitamin B levels;
were below the lower limit of normal in any
which acts to displace divalent cations (7).
the initial 3 months of treatment with met-
tials and affect divalent cation membrane
functions, such as those that are calcium
holoTCII value Ͻ40 pg/ml. Controlling for
dependent, and may act in general as a cal-
group was significantly lower at 6 months
DIABETES CARE, VOLUME 23, NUMBER 9, SEPTEMBER 2000
Metformin reduces vitamin B absorption 12 Table 2—Vitamin B and holoTCII values
min B stores (16,22). A state of severe B
12
deficiency, as a consequence of prolongedmetformin administration, may result in
peripheral nerve damage. This may be con-
fused with that of the peripheral neuropathy
of diabetes, a clinical scenario that could lead
allowed to progress, would be expected to
be followed by low serum total vitamin B12
levels and, presumably, eventual clinical
deficiency; this sequence of events was not
addressed in our study. Because the periph-
able from that of vitamin B deficiency, the
serum vitamin B is of great concern if not
recognized and treated appropriately. Ionic
plex to attach to ileal cell surface receptors,
with an oral calcium supplement. Patientswith type 2 diabetes treated with met-
Control subjects continued on sulfonylurea therapy.
formin, especially those who do not con-sume milk or milk products on a daily
affected by calcium. Specifically, the cell
the detection of negative vitamin B balance
basis or do not take supplemental calcium
surface TCII receptors on all DNA synthe-
and the clinical disorders caused by vitamin
B deficiency. However, in the past decade,
intake of calcium as well as be closely mon-
metformin may interfere with the delivery
it has been increasingly appreciated that nor-
of vitamin B to these cells (16). Calcium-
dependent processes in general may poten-
found in a significant proportion of patients
tially be altered by metformin, and whether
with varying clinical features of this vitamin
Acknowledgments— This work was sup-
such effects are significant physiologically
deficiency (9,11,12,16,20,21). Herzlich and
ported by Lipha Pharmaceuticals, Eastern Para-
has yet to be determined. However, in the
Herbert (11) were the first to report the
lyzed Veterans of America, the Veterans Affairs
study herein, there is no evidence that sup-
selective depletion of that portion of total
Medical Center (VAMC), and the Victor Herbert
plemental calcium has an adverse effect on
Research Fund at the VAMC, Bronx, New York.
metformin’s hypoglycemic effects. There is
reduction of holoTCII or TCII-B ) in early
Parts of this work have previously been pre-
negative vitamin B balance. This indicates
sented to the American Society of Hematology in
that the earliest serum marker of subnormal
1993 (W.B., S.S., E.J., and V.H.) and published as
an abstract in Blood 82 (Suppl. 1):432A, 1993.
(8,17,18). This finding is further supported
vitamin B absorption, and therefore of neg-
by our in vivo observation of a reversal of
References
1. Bailey CJ, Turner RC: Metformin. N Engl J
were affected similarly by metformin; how-
tute a significant percentage of total corri-
with oral calcium supplementation, just as
they do in elderly individuals given oral vit-
on long-term metformin therapy. Br Med J
of change in serum analogs or that of serum
folate in our study suggests that bacterial
exhibited overt clinical hematological or
3. Tomkin GH: Malabsorption of vitamin B12
overgrowth was not a significant factor in
formin: a comparison with metformin. Br
ciency because it takes over a year of nega-
4. Caspary WF, Creutzfeldt W: Analysis of the
inhibitory effect of biguanides on glucose
once considered to be a sensitive index for
in the elimination of nerve and blood vita-
absorption. Diabetologia 7:379–385, 1971
DIABETES CARE, VOLUME 23, NUMBER 9, SEPTEMBER 2000
Bauman and Associates
11. Herzlich B, Herbert V: Depletion of serum
ences Institute Press, 1996, p. 191–205
17. Herbert V: Mechanism of intrinsic factor
negative vitamin B balance. Lab Invest 58:
action in the isolated rat small intestine. J
absorption in diabetics on biguanides. Dia-
12. Miller JW, Green R, Herbert VD, Flynn MA:
18. Herbert V, Castle WB: Divalent cation and
Holotranscobalamin II is a reliable indicator
pH dependence of rat intrinsic factor action
Small intestinal transit in diabetics. Br Med
of rat small intestine. J Clin Invest 40:1978–
7. Schafer G: Some new aspects on the inter-
following oral B12 supplements (Abstract).
19. Brandt LJ, Bernstein LH, Wagle A: Produc-
biguanides with biological membranes.
13. Wickramasinghe SN, Fida S: Correlations
Biochem Pharmacol 25:2014–2024, 1976
between holo-transcobalamin II, holo-hap-
with small bowel bacterial overgrowth. Ann
8. Carmel R, Rosenberg AH, Lau KS, Streiff
from healthy subjects and patients. J Clin
20. Allen RH, Stabler SP, Savage DG, Linden-
baum J: Diagnosis of cobalamin deficiency.
enhancement by intrinsic factor. Gastroen-
14. Vu T, Amin J, Ramos M, Flener V, Vanyo L,
I. Usefulness of serum methylmalonic acid
and total homocysteine concentrations. Am
9. Kolhouse JF, Kondo H, Allen NC, Podell E,
Allen RH: Cobalamin analogues are present
21. Lindenbaum J, Savage DG, Stabler SP, Allen
patients. Am J Hematol 42:202–211, 1993
RH: Diagnosis of cobalamin deficiency. II.
15. Herbert V, Fong W, Gulle V, Stopler T: Low
Relative sensitivities of serum cobalamin,
dilution assays are not specific for true
holotranscobalamin II is the earliest serum
methylmalonic acid, and total homocysteine
cobalamin. N Engl J Med 299:785–792,
concentrations. Am J Hematol 34:99–107,
amin) absorption in patients with AIDS.
10. Lau KS, Gottlieb C, Wasserman LR, Herbert
22. Swain R: Stages of B12 deficiency. In Round
16. Herbert V: Vitamin B . In Present Knowl-Table Series 66: Vitamin B12 Deficiency. Her-
using radioisotope dilution and coated char-
edge in Nutrition. Ziegler EE, Filer LJ, Eds.
DIABETES CARE, VOLUME 23, NUMBER 9, SEPTEMBER 2000
Dott. Simone Piazza Curriculum Vitae Dati anagrafici Nato a simone.piazza@maggioreosp.novara.it – info@curepalliativepiazza.it Carriera Scolastica e Professionale Diploma di maturità scientifica conseguito presso l’istituto “Liceo Scientifico P. Gobetti” di Omegna nel luglio 1996 con il punteggio di 50/60. Diploma di laurea in Medicina e Chirurgia cons
Effects of rosiglitazone and sumatriptan on human isolated small and large coronary arteries Kathryn Bagot, Mozam Ali, Lee Dawson, Sandy Williams, Bob SheldrickAsterand UK Ltd, 2 Orchard Road, Royston, Hertfordshire, SG8 5HD, UK. Introduction Species differences in receptor type, expression level or coupling can lead to marked differences in responses between laboratory animals a
 Metformin reduces vitamin B absorption
Metformin reduces vitamin B absorption