Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Gastricpacer.it
See Corresponding Editorial by Hirsch and Mackintosh on pages 2– 4
Autonomic Nervous System Activity and the State and Development of Obesity in Japanese School Children Narumi Nagai,* Tamaki Matsumoto,† Hiroko Kita,‡ and Toshio Moritani*Abstract Results: The obese children demonstrated a significantly
lower TP (6.77 Ϯ 0.12 vs. 7.11 Ϯ 0.04 ln ms2, p Ͻ 0.05),
KITA, AND TOSHIO MORITANI. Autonomic nervous
LF power (6.16 Ϯ 0.12 vs. 6.42 Ϯ 0.05 ln ms2, p Ͻ 0.05),
system activity and the state and development of obesity in
and HF power (5.84 Ϯ 0.15 vs. 6.34 Ϯ 0.07 ln ms2, p Ͻ
Japanese school children. Obes Res. 2003;11:25–32.
0.01) compared with the non-obese children. A partial cor-
Objective: The autonomic nervous system (ANS) plays an
relation analysis revealed that the LF and HF powers among
important role in regulating energy expenditure and body
42 obese children were negatively associated with the du-
fat content; however, the extent to which the ANS con-
ration of obesity independent of age (LF: partial r ϭ Ϫ0.55,
tributes to pediatric obesity remains inconclusive. The aim
p Ͻ 0.001; HF: partial r ϭ Ϫ0.40, p Ͻ 0.01). The obese
of this study was to evaluate whether sympathetic and/or
children were further subdivided into two groups based on
the parasympathetic nerve activities were altered in an
the length of their obesity. All three spectral powers were
obese pediatric population. We further examined a physio-
significantly reduced in the obese group with obesity of
logical association between the duration of obesity and
Ͼ3 years (n ϭ 18) compared to the group with obesity
the sympatho-vagal activities to scrutinize the nature of
ANS alteration as a possible etiologic factor of childhood
Discussion: Our data indicate that obese children possess
reduced sympathetic as well as parasympathetic nerve ac-
Research Methods and Procedures: Forty-two obese and
tivities. Such autonomic depression, which is associated
42 non-obese healthy sedentary school children were care-
with the duration of obesity, could be a physiological factor
fully selected from 1080 participants initially recruited to
promoting the state and development of obesity. These
this study. The two groups were matched in age, gender, and
findings further imply that preventing and treating obesity
height. The clinical records of physical characteristics and
beginning in the childhood years could be an urgent andcrucial pediatric public health issue.
development of the obese children were retrospectivelyreviewed to investigate the onset and progression of obesity. Key words: childhood obesity, duration of obesity, sym-
The ANS activities were assessed during a resting condition
pathetic nervous system, parasympathetic nervous sys-
by means of heart rate variability power spectral analysis,
tem, heart rate variability
which enables us to identify separate frequency compo-nents, i.e., total power (TP), low-frequency (LF) power, andhigh-frequency (HF) power. The spectral powers were thenlogarithmically transformed for statistical testing. Introduction
An increase in obesity prevalence has been observed
internationally in children from preschool age to adoles-
cence (1). Alarming findings are now emerging from Asian
Accepted for publication in final form September 3, 2002.
countries that are rapidly westernizing their lifestyles, par-
*Laboratory of Applied Physiology, Graduate School of Human and Environmental Studies,Kyoto University, Kyoto, Japan; †International Buddhist University, Osaka, Japan; and
ticularly their behavioral and dietary habits. As for Japan,
‡Division of Environmental Health, Hyogo Prefecture Institute of Public Health, Hyogo,
the 2000 annual report of the health and physical develop-
ment of the pediatric population disclosed that the number
Address correspondence to Dr. Toshio Moritani, Laboratory of Applied Physiology, Grad-uate School of Human and Environmental Studies, Kyoto University, Sakyo-ku, Kyoto
of obese children ages 6 to 11 years has approximately
doubled over the last 20 years (2). Data from previous
E-mail: t.moritani@neuro.mbox.media.kyoto-u.ac.jpCopyright 2003 NAASO
studies provide strong evidence that a higher level of body
OBESITY RESEARCH Vol. 11 No. 1 January 2003
Autonomic Nervous System Activity, Nagai et al.
mass index (BMI)1 during childhood can predict overweight
spectral analysis have shown that obese young women
later in life (3,4). To make matters worse, obesity in chil-
possess significantly lower SNS activity against various
dren is associated with various adverse biochemical, phys-
thermogenic perturbations, such as cold exposure (23), cap-
iological, and psychological effects, many of which have
saicin-containing yellow curry diet (24), and mixed food
strong links with chronic disease risk factors in adulthood
intake (25). Unlike invasive measurements such as plasma
(4,5). Thus, finding etiologic factors of obesity, as well as
catecholamine concentration, catecholamine turnover, and
preventing the obesity epidemic beginning in the childhood
muscle sympathetic nerve activity, the HRV power spec-
years, is currently a critical issue in the pediatric public
tral analysis lightens the burden imposed on subjects during
an experiment and is a suitable and valuable approach to
Although many environmental and genetic factors are
evaluating ANS activity in large-scale pediatric obesity
intermingled, the development of obesity is ultimately
caused by a sequential alteration of energy balance, with
Accordingly, in this study, we evaluated resting ANS
energy intake exceeding energy expenditure (6). The stabil-
activity by means of the HRV power spectral analysis in
ity of a human’s internal environment depends largely on
healthy sedentary non-obese and obese school children who
the orchestrations of the autonomic nervous system (ANS).
were carefully selected to avoid the physiological heteroge-
Because the sympathetic branch of the system particularly
neity of obesity, and investigated whether the SNS and/or
contributes to coordinating energy homeostasis, the alter-
the PNS activities were altered in an obese pediatric popu-
ation of sympathetic nervous system (SNS) activity is
lation. We also retrospectively reviewed clinical records of
widely assumed to promote onset and development of obe-
physical characteristics and development within the obese
sity. The MONA LISA hypothesis, an acronym for Most
children, and examined a physiological association between
Obesities kNown Are Low In Sympathetic Activity (7), has
the history of obesity (the onset and progression of obesity)
been supported (8,9). However, disagreement still exists
and the sympathovagal activities in order to further scruti-
over the nature of the sympathetic abnormality within the
nize the nature of ANS alteration as a possible etiologic
adult obese population (10,11). Less research has been done
with children, and the findings regarding the physiologicalrole of the SNS on pediatric obesity have been thus farinconclusive (12–14). The discrepancy is thought to arise
Research Methods and Procedures
largely from the difficulty in controlling the array of vari-
Subjects
ables (including age, gender, the history of obesity, other
One thousand eighty obese and non-obese healthy Japa-
medical complications, dietary and behavioral habits,
nese children, ages 6 to 12 years, initially volunteered to
physical activity levels, and emotional stress) and in ade-
participate in this research. The study protocol was ap-
quately assessing SNS activity in human subjects of all age
proved by the Institutional Review Board of Kyoto Univer-
sity Graduate School. All children and their parents were
Heart rate variability (HRV) power spectral analysis is a
carefully instructed about the study and gave their written
well-accepted, useful, and noninvasive method, and has
informed consent to participate in the study. Before obtain-
provided a comprehensive quantitative and qualitative eval-
ing any data from the children, the parents completed a
uation of neuroautonomic function under various research
standardized health questionnaire regarding their children’s
and clinical settings (15–17). In general, power spectral
past medical history, current health condition, past records
analysis of HRV has shown at least two distinct regions of
of height and body weight for estimating the history of
periodicity in electrocardiogram (ECG) R-R intervals. The
obesity, diet, physical activity, and lifestyle.
high-frequency component (Ͼ0.15 Hz) is a major contrib-
After measuring height and body weight, percentage of
utor to reflecting parasympathetic nervous system (PNS)
body fat was determined by means of a bioelectrical imped-
activity, and the low-frequency component (Ͻ0.15 Hz) is
ance analyzer (Model TBF-534; Tanita Corp., Tokyo, Ja-
associated with both SNS and the PNS activities (18,19).
pan). The analyzer has been used in several pediatric inves-
Previous investigations have demonstrated that the percent-
tigations because it produces a reasonable estimate for body
age of body fat (20), changes in body weight and energy
fat content in children (26,27). BMI was also calculated as
storage (21), and glucose-induced thermogenesis (22) were
body weight divided by square height. “Obesity” was de-
correlated with differences in the power spectral compo-
fined based on the criterion previously used in pediatric
nents. A series of our recent studies with the HRV power
research (Ͼ120% of the standard body weight for Japanesechildren) (3).
The results of the health questionnaires and the body
1 Nonstandard abbreviations: BMI, body mass index; ANS, autonomic nervous system;
composition measurements were carefully examined. Then,
SNS, sympathetic nervous system; HRV, heart rate variability; ECG, electrocardiogram;
42 obese and 42 non-obese children were selected for
PNS, parasympathetic nervous system; TP, total power; LF, low frequency; HF, highfrequency; MSNA, muscle sympathetic nerve activity.
investigation of a physiological association of childhood
OBESITY RESEARCH Vol. 11 No. 1 January 2003
Autonomic Nervous System Activity, Nagai et al. R-R Spectral Analysis Procedure Table 1. Physical characteristics of children
Our R-R interval power spectral analysis procedures have
been fully described elsewhere (16,30,31). Briefly, analog
Non-obese
output of the ECG monitor (MEG-6100; Nihon Kohden,
(n ؍ 42) (n ؍ 42)
Tokyo, Japan) was digitized through a 13-bit analog-to-
digital converter (HTB 410; Trans Era, South Orem, UT) ata sampling rate of 1024 Hz. The digitized ECG signals were
differentiated, and the resultant ECG QRS spikes and the
intervals of the impulses (R-R intervals) were stored se-
quentially on a hard disk for later analyses.
Before R-R spectral analysis was performed, the stored
R-R interval data were displayed and aligned sequentially to
obtain equally spaced samples with an effective sampling
frequency of 2 Hz (32) and displayed on a computer screenfor visual inspection. Then, the direct current component
Values are expressed as means Ϯ SE.
and linear trend were completely eliminated by digital fil-
tering for the band-pass between 0.03 and 0.5 Hz. The rootmean square value of the R-R interval was calculated asrepresenting the average amplitude. After passing throughthe Hamming-type data window, power spectral analysis by
obesity and ANS activity. The two groups were matched in
means of a fast Fourier transform was performed on a
age, gender, and height. All children were in good health
consecutive 256-s time series of R-R interval data obtained
and had no personal or family history of hypertension,
cardiovascular disease, diabetes mellitus, or other endocrine
Based on our previous investigations (16,30,31,33), the
diseases. None of the children were taking any medications.
spectral powers in frequency domain were quantified by
According to the nutritional survey included in the health
integrating the areas under the curves for the following
questionnaire, daily energy intake and nutritional content of
respective band width: the low-frequency (LF: 0.03 and
food did not significantly differ between the two groups.
0.15 Hz), an indicator of both SNS and PNS activity; the
Concerning the physical activity level, none of the children
high-frequency (HF: 0.15 and 0.5 Hz), which solely reflects
in these groups regularly engaged in sports activities or
the PNS activity; and the total power (TP: 0.03 and 0.5 Hz),
aerobic exercises. The descriptive characteristics of the chil-
representing the overall ANS activity. Because basal spec-
tral absolute values differed greatly among individuals, thespectral powers were then logarithmically transformed for
Methods
The children came at 8:30 AM to the temporary laboratory
that was set up in the school infirmary. All experiments
Statistical Analyses
were performed in the morning, and the entire research
All data are expressed as mean Ϯ SE. Student’s unpaired
project lasted for 2 consecutive days in June. The room
t test was performed to assess statistical differences in
was temperature controlled (25 °C), quiet, and comfortable,
physical characteristics and the parameters of the ANS
with minimal arousal stimuli. After appropriate skin prep-
activity between the obese and non-obese groups. Partial
aration, the subjects were fitted with ECG electrodes and
correlation analysis was performed to examine the re-
then rested for at least 15 minutes before the start of the
lationships between the ANS parameters and the dura-
tion of obesity independently of a covariate, i.e., age. All p
After the resting period, the CM lead ECG signals were
values were two-sided. A p value of Ͻ0.05 was chosen as
continuously recorded for 4.5 minutes while each child
the level of significance. All statistical analyses were made
remained seated in a chair and breathed normally (28). It
on a personal computer with a commercial software
should be noted that, according to our preliminary experi-
package (SPSS version 10.0J for Windows; SPSS Inc.,
ment as well as accepted parameters of pediatric physiology
(29), children’s breathing frequency is generally higher than9 rates per minute (Ͼ0.15 Hz). Thus, we assumed that,without controlling the respiration rates during the ECG
measurements, respiratory-linked variations in heart rate did
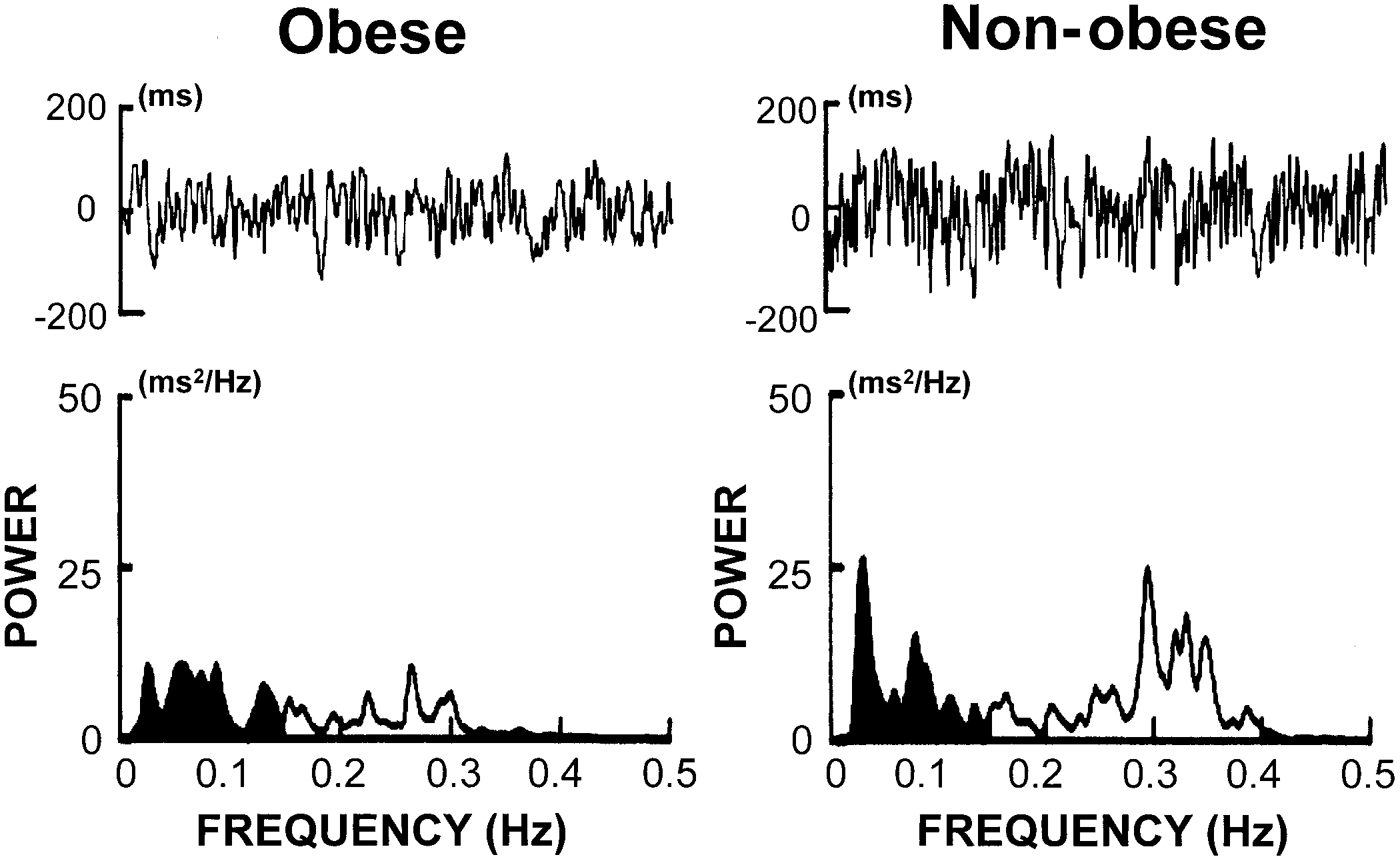
Figure 1 represents typical sets of raw R-R intervals and
not overlap with low-frequency heart rate fluctuations
the power spectral data obtained from an obese and a
non-obese child, respectively, during the resting condition.
OBESITY RESEARCH Vol. 11 No. 1 January 2003
Autonomic Nervous System Activity, Nagai et al. Figure 1: Examples of ECG R-R interval changes and the corresponding power spectra for an obese and a non-obese child at rest,respectively.
According to visual inspection, the obese child possessed
HF: partial r ϭ Ϫ0.40, p Ͻ 0.01). A statistical analysis
remarkably reduced ranges in R-R variability, as well as in
demonstrated that all three spectral powers were signifi-
both frequency components of the power spectrum, com-
cantly reduced in the group with obesity of Ͼ3 years
(n ϭ 18) compared to the group with obesity of Ͻ3 years
The statistical analysis revealed that there were signifi-
(n ϭ 24; TP: 6.35 Ϯ 0.15 vs. 7.33 Ϯ 0.09 ln ms2, p Ͻ 0.01;
cant differences in the R-R spectral parameters between the
LF: 5.78 Ϯ 0.15 vs. 6.67 Ϯ 0.12 ln ms2, p Ͻ 0.01; HF:
two groups. The obese group had a significantly higher
5.37 Ϯ 0.20 vs. 6.46 Ϯ 0.13 ln ms2, p Ͻ 0.01).
resting heart rate compared with the non-obese group(90.7 Ϯ 1.5 vs. 84.3 Ϯ 1.0 beats per minute, p Ͻ 0.001). AsFigure 2 demonstrates, all the spectral powers were signif-
Discussion
icantly lower in the obese group than in the non-obese group
This study provides valuable information regarding a
(TP: 6.77 Ϯ 0.12 vs. 7.11 Ϯ 0.04 ln ms2, p Ͻ 0.05; LF:
potential etiologic association between childhood obesity
6.16 Ϯ 0.12 vs. 6.42 Ϯ 0.05 ln ms2, p Ͻ 0.05; HF: 5.84 Ϯ
and ANS activity. The main findings are that healthy sed-
0.15 vs. 6.34 Ϯ 0.07 ln ms2, p Ͻ 0.01), indicating that both
entary obese school children possess much lower sympa-
SNS and PNS activity decrease in obese children.
thetic and parasympathetic nerve activities. In addition, a
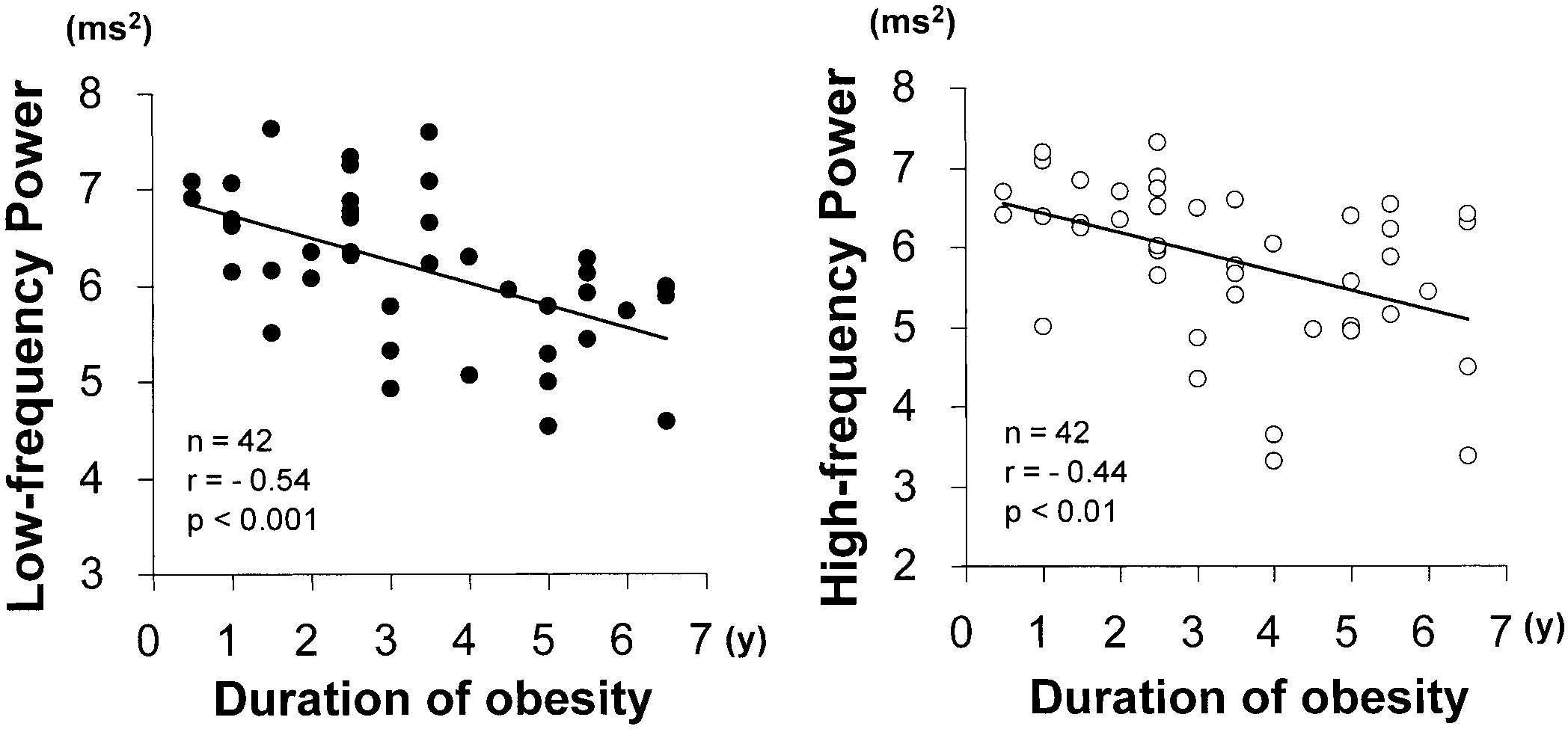
To further investigate an association between the HRV
degree of these autonomic reductions depends on the dura-
spectral powers and the history of obesity, the obese chil-
tion of obesity independent of a subject’s age.
dren were subdivided into two groups based on the length of
It is well known that the coordination of energy ho-
obesity. It has been shown that physiological factors such as
meostasis particularly relies on the normal functioning of
age influence HRV (34,35); thus, we performed the partial
the sympathoadrenal system. As the MONA LISA hypoth-
correlation analysis to examine the relationship after adjust-
esis indicates (7), it is reasonable to assume that reduced
ment for age. As Figure 3 shows, the LF and HF powers
SNS activity leads to a lower rate of thermogenesis, and
among 42 obese children were negatively correlated with
consequently, to a positive energy balance and obesity.
the duration of obesity (LF: partial r ϭ Ϫ0.55, p Ͻ 0.001,
Despite intensive research, physiological roles of SNS ac-
OBESITY RESEARCH Vol. 11 No. 1 January 2003
Autonomic Nervous System Activity, Nagai et al. Figure 2: Comparison of total, low-frequency, and high-frequency powers between the obese and the non-obese groups, respectively. Results are expressed as mean Ϯ SE for each group. *p Ͻ 0.05, **p Ͻ 0.01.
tivity on human obesity remain unclear. The different meth-
results over the nature of the SNS affected by obesity (36).
odologies used among investigators may have caused this
Technical developments have allowed direct intraneural re-
situation. For instance, plasma and urinary norepinephrine
cordings of sympathetic nerve traffic by microneurography,
estimates, both of which are commonly used as global
but the technique is limited to peripherally measuring SNS
indexes for sympathetic activity, have provided conflicting
activity in the skin and skeletal muscles (9,37). The muscle
Figure 3: Partial correlations between both the low-frequency and the high-frequency powers and the duration of obesity, independent ofa physiological effect of age among 42 obese children.
OBESITY RESEARCH Vol. 11 No. 1 January 2003
Autonomic Nervous System Activity, Nagai et al.
sympathetic nerve activity (MSNA) has been applied to
ues of spectral components to examine the ANS features of
obesity research, generally demonstrating a positive corre-
pediatric obesity, and provided the evidence that the TP, LF,
lation between the amount of body fat and MSNA (10,11).
and HF powers were all more substantially reduced in the
Because measuring MSNA requires the insertion of a fine
obese than in the non-obese children. It has been pointed out
tungsten microelectrode and because MSNA is mainly re-
that the frequency component of HRV spectral analysis,
lated to the control of blood pressure rather than energy
which reflects only the SNS activity, is difficult to single
metabolism, the methodology is not relevant to investigat-
out. The normalized units and the ratios, i.e., LF/HF, have
ing SNS activity, especially in a pediatric and epide-
been used as alternative indexes to evaluate SNS and PNS
activities (13,16,22). These indexes have been valuable
The spectral analysis of HRV has attracted considerable
and applicable to clinical settings as well as basic physio-
attention from investigators in various physiological fields,
logical research, but the results could overestimate or
including diabetes and obesity research both for adult (16,
underestimate the sympatho-vagal activity because the in-
20 –22, 31) and pediatric populations (13,14,38 – 41), and
dexes are relative values. As described above, neuro-
has become a reliable noninvasive measure to appraise
physiological contributions to the LF and HF powers have
ANS activity. As to an association of the ANS and energy
been clarified, and SNS activity, at least in part, does
homeostasis, Landsberg and Young (42) indicated that cat-
contribute to the LF power even in the resting condition
echolamine turnover within cardiac tissue could precisely
(23). We recognize that the LF power, like all other indi-
reflect autonomic events that affect energy metabolism else-
cators, has its limitations in precisely measuring SNS ac-
where in the body. We have conducted a pharmacological
tivity. Nevertheless, under the condition that the LF power
blockade experiment to confirm the validity of the HRV
together with the HF power and the TP all significantly
power spectral analysis for evaluating and quantifying the
decrease, which has appeared in presently healthy obese
sympathovagal activity. In short, after atropine, a parasym-
children, it is plausible to assume that both SNS and PNS
pathetic muscarinic antagonist, was intravenously injected,
R-R variability was markedly reduced and the HF compo-
Even during childhood, low levels of PNS activity are
nents were almost entirely abolished, whereas the LF com-
associated with cardiac autonomic neuropathy in diabetics
ponents were partly decreased. When propranolol, a -ad-
with poor metabolic control (39), duration of diabetes (40),
renoceptor antagonist, was additionally injected, heart rate
and elevated blood pressure (47). Taking the previous re-
fluctuations were almost entirely abolished, and the resting
sults into consideration, reduced PNS activity appearing in
energy expenditure was significantly reduced (23,25,31).
presently healthy obese children might be a conceivable
Previous clinical studies further demonstrated that noninsu-
early sign to predict cardiovascular and metabolic health. As
lin-dependent diabetes mellitus patients with neuropathy
to the SNS activity, our results suggest the possibility that
had markedly reduced R-R interval fluctuations and HRV
the MONA LISA hypothesis, indicating that obesity is
spectral power at rest compared with healthy individuals
associated with a relative or absolute reduction in the ther-
(16,30). These findings support the previous studies (18,19)
mogenic component of SNS activity, might, at least in part,
and indicate that 1) the HF power is associated solely with
contribute to our understanding of the pathophysiological
PNS activity, and the LF power is jointly mediated by PNS
features of pediatric obesity. Normal or increased levels of
and SNS activities, and 2) R-R interval variability and the
SNS activity and its blunted responsiveness seem to be
integrated values of all the components of power spectra
present in adult-established obesity (9,11,23–25). Taken
could reflect the overall ANS activity. Concerning the ex-
together, the nature of SNS alteration in human obesity
perimental setting, several studies have faced a difficulty in
might diversify depending on the time in which the obese
using HRV spectral analysis during nonresting conditions
state occurs, is promoted, or is established.
such as dynamic exercise, but the validity of spectral anal-
We have extensively reviewed the literature regarding
ysis of HRV under the resting condition, which we used in
pediatric obesity. To the best of our knowledge, however, a
this study, has been well documented (16,17,43). Therefore,
limited number of studies have been conducted to examine
the application of HRV spectral analysis in a childhood
the physiological role of ANS in human obesity during the
population has distinct advantages over the existing meth-
early stage of life. Martini et al. (13) and Riva et al. (14)
ods for autonomic function in that it is noninvasive, less
used time- and frequency-domain of HRV measured by
time consuming, and less upsetting for young participants
24-hour Holter recordings, and suggested that obese ado-
lescents with metabolic changes, such as hyperinsulinemia,
Although quantification and interpretation of HRV re-
euglycemia, or dislipidemia, may have a sympathovagal
main a complex issue (15,44), the efficacy and applicability
balance, characterized by a primary decrease in PNS activ-
of the technique used in the present investigation have been
ity with a relative prevalence of SNS activity. Yakinci et al.
shown in previous research (16,30,31,33,45,46). By apply-
(12) performed noninvasive autonomic tests, including or-
ing this analysis procedure, we measured the absolute val-
thostatic test, Valsalva maneuver, and deep breathing, and
OBESITY RESEARCH Vol. 11 No. 1 January 2003
Autonomic Nervous System Activity, Nagai et al.
indicated normal activity of SNS and hypoactivity of PNS
fare Center of Ako and Tatsuno in Hyogo Prefecture for
in obese children. According to the study of Wawryk et al.
their cooperation and assistance during the experiments.
(41), both LF and HF components were significantly re-duced, which suggests autonomic suppression, in children
References
with diabetes mellitus and greater body weight compared
1. World Health Organization. Obesity: Preventing and Man-
with the control group. Because of the disparity in the
aging the Global Epidemic. Report of a WHO consultation.
experimental conditions, i.e., subjects’ age and clinical
Geneva: World Health Organization; 1998.
2. The Division of Health Promotion and Welfare in the
characteristics, the number of participants, and analytical
Public Life Science Department of Hyogo Prefecture. The
procedures for the ANS activity, the outcomes of these
annual report of investigating health and physical develop-
investigations and our study were not always consistent. We
ment for preschool and school-aged children in 2000. 2000,
assume, however, that the autonomic alteration is evident
and might be an important etiologic factor of childhood
3. Kotani K, Nishida M, Yamashita S, et al. Two decades of
annual medical examinations in Japanese obese children: do
Other intriguing results obtained from this study were
obese children grow into obese adults? Int J Obes Relat Metab
that the LF and HF powers decreased with increasing du-
ration of obesity and that the depression of these powers
4. Whitaker RC, Wright JA, Pepe MS, Seidel KD, Dietz WH.
Predicting obesity in young adulthood from childhood and
was more apparent in the children with obesity of more than
parental obesity. N Engl J Med. 1997;337: 869 –73
3 years. Age has been reported to have a strong influence on
5. Mossberg H-O. 40-year follow-up of overweight children.
HRV (34,35). Thus, we performed a partial correlation
analysis, revealing that the reduction of the spectral powers
6. Bray GA. Autonomic and endocrine factors in the regulation
was not related to a physiological effect of age. Future
of energy balance. Fed Proc. 1986;45:1404 –10.
longitudinal research will be needed to confirm the changes
7. Bray GA. Obesity, a disorder of nutrient partitioning: the
of ANS activity and the development of obesity in the
MONA LISA hypothesis. J Nutr. 1991;121:1146 – 62.
childhood. Nonetheless, the present data indicate that an
8. Peterson HR, Rothschild M, Weinberg CR, Fell RD,
increasing duration of obesity could affect the global levels
McLeish KR, Pfeifer MA. Body fat and the activity of the autonomic nervous system. N Engl J Med. 1988;318:1077– 83.
and/or functions of SNS as well as PNS in simple obese
9. van Baak MA. The peripheral sympathetic nervous system in
human obesity. Obes Rev. 2001;2:3–14.
In summary, we investigated a potential physiological
10. Scherrer U, Randin D, Tappy L, Vollenweider P, Jequier
association of ANS activity and the state and development
E, Nicod P. Body fat and sympathetic nerve activity in healthy
of obesity in healthy sedentary school children. Causes and
subjects. Circulation. 1994;89:2634 – 40.
consequences of human obesity continue to elude. Our
11. Spraul M, Anderson EA, Bogardus C, Ravussin E. Muscle
findings, however, indicate that childhood obesity is closely
sympathetic nerve activity in response to glucose ingestion: im-
interrelated with the reduction of both SNS and PNS activ-
pact of plasma insulin and body fat. Diabetes. 1994;43:191– 6.
ities. Because the ANS is involved in nearly every important
12. Yakinci C, Mungen B, Karabiber H, Tayfun M, Everek- lioglu C. Autonomic nervous system functions in obese chil-
homeostatic process going on within the body, the suppres-
dren. Brain Dev. 2000;22:151–3.
sion of autonomic functioning can cause far-reaching ad-
13. Martini G, Riva P, Rabbia F, et al. Heart rate variability in
verse effects, including metabolic disorder and cardiovas-
childhood obesity. Clin Auton Res. 2001;11:87–91.
cular malfunction, and consequently, undermine children’s
14. Riva P, Martini G, Rabbia F, et al. Obesity and autonomic
health. In addition, the risk of obesity in adulthood is
function in adolescence. Clin Exp Hypertens. 2001;23:57– 67.
increased for obese children. Thus, this study further im-
15. Conny MA, Louis AA, Jeroen CW, Gerard BA, Herman P.
plies that preventing and treating obesity beginning in the
Heart rate variability. Ann Intern Med. 1993;118:436 – 47.
childhood years is an urgent and crucial pediatric public
16. Moritani T, Hayashi T, Shinohara M, Mimasa F, Masuda I, Nakao K. Sympatho-vagal activities of NIDDM patients during exercise as determined by heart rate spectral analysis. In: Kawamori R, Vranic M, Horton ES, Kubota M, eds. Acknowledgments Glucose Fluxes, Exercise and Diabetes. London, UK; Smith-
This study was supported in part by a Japanese Ministry
of Education, Science, Sports and Culture Grant-in-Aid for
17. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology.
Scientific Research (B)11480011. We are grateful to the
Heart rate variability. Standard of measurements, physiological
children of the Misaki and Ikaruga elementary schools and
interpretation and clinical use. Circulation. 1996;93:1043– 65.
their parents for their enthusiastic participation. We also
18. Akselrod S, Gordon D, Ubel FA, Shannon DC, Barger AC,
thank the teachers in the Misaki and Ikaruga elementary
Cohen RJ. Power spectrum analysis of heart rate fluctuation:
schools for their kind support and great efforts. Finally, we
a quantitative probe of beat-to-beat cardiovascular control.
appreciate the research staffs at the Public Health and Wel-
OBESITY RESEARCH Vol. 11 No. 1 January 2003
Autonomic Nervous System Activity, Nagai et al.
19. Pagani M, Lombardi F, Guzzetti S, et al. Power spectral
32. Rompelman O, Coenen AJR, Kitney RI. Measurement of
analysis of heart rate and arterial pressure variabilities as a
heart-rate variability: part 1— comparative study of heart-rate
marker of sympatho-vagal interaction in man and conscious
variability analysis methods. Med Biol Eng Comput. 1977;15:
dog. Circ Res. 1986;59:178 –93.
20. Petretta M, Bonaduce D, De Filippo E, et al. Assessment of
33. Amano M, Kanda T, Ue H, Moritani T. Exercise training
cardiac autonomic control by heart period variability in pa-
and autonomic nervous system in obese individuals. Med Sci
tients with early-onset familial obesity. Eur J Clin Invest. Sport Exer. 2001;33:1287–91.
34. Yeragani VK, Pohl R, Berger R, Balon R, Srinivasan K.
21. Hirsch J, Leibel RL, Mackintosh R, Aguirre A. Heart rate
Relationship between age and heart rate variability in supine
variability as a measure of autonomic function during weight
and standing postures: a study of spectral analysis of heart
change in humans. Am J Physiol. 1991;261:R1418 –R23.
rate. Pediatr Cardiol. 1994;15:14 –20.
22. Paolisso G, Manzella D, Ferrara N, et al. Glucose ingestion
35. Finley JP, Nugent ST. Heart rate variability in infants, chil-
affects cardiac ANS in healthy subjects with different amounts
dren and young adults. J Auton Nerv Syst. 1995;51:103– 8.
of body fat. Am J Physiol. 1997;273:E471–E8.
36. Young JB, Macdonald IA. Sympathoadrenal activity in hu-
23. Matsumoto T, Miyawaki T, Ue H, Kanda T, Zenji C,
man obesity: heterogeneity of findings since 1980. Int J ObesMoritani T. Autonomic responsiveness to acute cold expo- Relat Metab Disord. 1992;16:959 – 67.
sure in obese and non-obese young women. Int J Obes Relat
37. Snitker S. Macdonald I, Ravussin E, Astrup A. The sym- Metab Disord. 1999;23:793– 800.
pathetic nervous system and obesity: role in aetiology andtreatment. Obes Rev. 2000;1:5–15.
24. Matsumoto T, Miyawaki C, Ue H, Yuasa T, Miyatsuji A,
38. Gutin B, Owens S, Slavens G, Riggs S, Treiber F. Effect of Moritani T. Effects of capsaicin-containing yellow curry
physical training on heart-period variability in obese children.
sauce on sympathetic nervous system activity and diet-in-
J Pediatr. 1997;130:938 – 43.
duced thermogenesis in lean and obese young women. J Nutr
39. Akinci A, Celiker A, Baykal E, Tezic T. Heart rate variabil- Sci Vitaminol. 2000;46:309 –15.
ity in diabetic children: sensitivity of the time- and frequency-
25. Matsumoto T, Miyawaki C, Ue T, Kanda T, Yoshitake Y,
domain methods. Pediatr Cardiol. 1993;14:140 – 6. Moritani T. Comparison of thermogenic sympathetic re-
40. Rollins MD, Jenkins JG, Carson DJ, McClure BG, Mitch-
sponse to food intake between obese and non-obese young
ell RH, Imam SZ. Power spectral analysis of the electrocar-
women. Obes Res. 2001;9:78 – 85.
diogram in diabetic children. Diabetologia. 1992;35:452–5.
26. Battistini N, Brambilla P, Virgili F, et al. The prediction of
41. Wawryk AM, Bates DJ, Couper JJ. Power spectral analysis
total body water from body impedance in young obese sub-
of heart rate variability in children and adolescents with
jects. Int J Obes Relat Metab Disord. 1992;16:207–12.
IDDM. Diabetes Care. 1997;20:1416 –21.
27. Houtkooper LB, Going SB, Lohman TG, Roche AF, Van
42. Landsberg L, Young JB. Fasting, feeding and regulation of Loan M. Bioelectrical impedance estimation of fat-free body
the sympathetic nervous system. N Engl J Med. 1978;298:
mass in children and youth: a cross-validation study. J Appl
43. Rimoldi O, Furlan R, Pagani MR, et al. Analysis of neural
28. Gutin B, Owens S. Role of exercise intervention in improving
mechanisms accompanying different intensities of dynamic
body fat distribution and risk profile in children. Am J Human
exercise. Chest. 1992;101:226S–30S.
44. Eckberg DL. Sympathovagal balance: a critical appraisal.
29. Malina RM. and Bouchard C. Heart, blood, and lung Circulation. 1997;96:3224 –32.
changes during growth. In: Malina RM, Bouchard C, eds.
45. Hibino G, Moritani T, Kawada T, Fushiki T. Caffeine Growth, Maturation, and Physical Activity. Champaign, IL:
enhances modulation of parasympathetic nerve activity in
Human Kinetics Books; 1991, pp. 163– 4.
humans: quantification using power spectral analysis. J Nutr.
30. Moritani T, Hayashi T, Shinohara M, Mimasa F, Shibata M. Comparison of sympatho-vagal function among diabetic
46. Shihara N, Yasuda K, Moritani T, et al. The association
patients, normal controls and endurance athletes by heart rate
between Trp64Arg polymorphism of the beta3-adrenergic re-
spectral analysis. J Sports Med Sci. 1993;7:31–9.
ceptor and autonomic nervous system activity. J Clin Endo-
31. Hayashi T, Masuda I, Shinohara M, Moritani T, Nakao K. crinol Metab. 1999;84:1623–7.
Autonomic nerve activity during physical exercise and pos-
47. Javorka K, Buchanec J, Javorkova J, et al. Heart rate and
tural change: investigations by power spectral analysis of heart
its variability in juvenile hypertonics during respiratory ma-
rate variability. Jpn J Biochem Exerc. 1994;6:30 –7.
neuvers. Clin Exp Hypertens. 1988;10:391– 409.
OBESITY RESEARCH Vol. 11 No. 1 January 2003
11/07/2013 - BOLLETTINO UFFICIALE DELLA REGIONE LAZIO - N. 56 Tariffa Euro Descrizione PRESTAZIONI DI ASSISTENZA SPECIALISTICA AMBULATORIALE - NOMENCLATORE TARIFFARIO "Allegato A " IPERTERMIA PER IL TRATTAMENTO DI TUMORE Ipertermia [terapia aggiuntiva] indotta da microonde ultrasuoni, radiofrequenza a bassa energia, sonde intestinali, o altri mezzi per trattamento di tumoreTR
C Â M A R A M U N I C I PA L Acta da Reunião Pública da Câmara Municipal do Porto, realizada em 29 de Maio de 2001 PRESENTES: O Senhor Presidente, Eng.º Nuno Magalhães Car- doso, que presidiu, e os Senhores Vereadores Eng.º Orlando BarrosG a s p a r, Prof.ª Ernestina Miranda, Dr.ª Maria José Azevedo, Dr.ª MariaManuela Vieira, Prof. António Hernâni Gonçalves, Dr. José
 Autonomic Nervous System Activity, Nagai et al.
Autonomic Nervous System Activity, Nagai et al.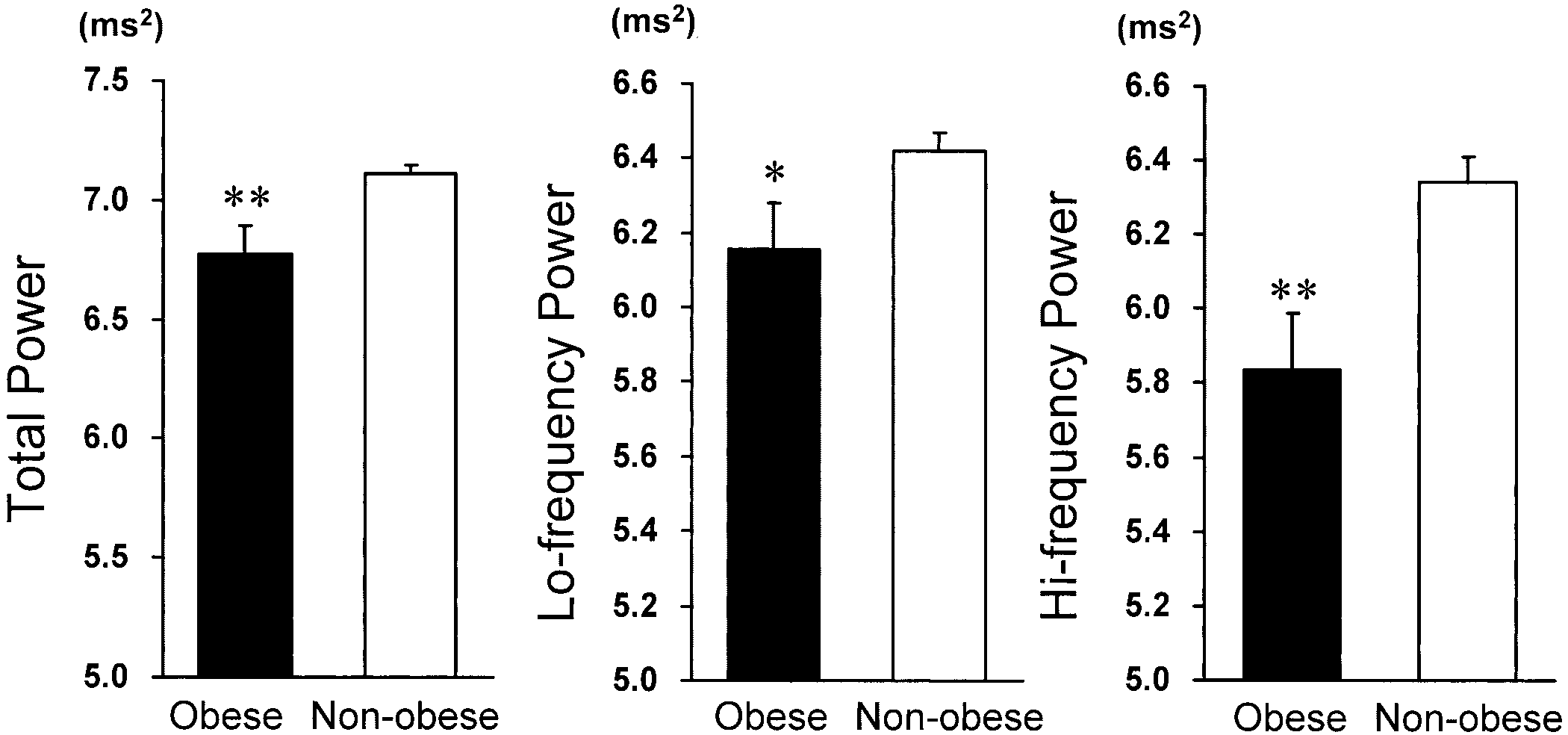
 Autonomic Nervous System Activity, Nagai et al.
Autonomic Nervous System Activity, Nagai et al.