Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Home SVCCArea:English - Español - Português Expanding Access to Safe and Effective Tobacco Dependence Treatments-Lessons from the USA and Beyond Saul Shiffman*, PhD; Joe Gitchell**, MD *Psychology, Psychiatry and Pharmaceutical Science, University of Pittsburgh & Pinney Associates, Pittsburgh, PA, USA
**Pinney Associates, Bethesda, MD, USA The authors provide consulting services to Glaxo Smith Kline, marketers of stop smoking medications INTRODUCTION The single largest challenge in health promotion and disease prevention for the next 50 years will be stimulating dramatic increases in the numbers of cigarette smokers who quit smoking.
This is the primary strategy available to reduce tobacco-caused death and disease over this term, and unfortunately, we have a long way to go to achieve the level of quitting that would be necessary to improve health radically.
There are two mechanisms to increase the number of cigarette smokers who successfully quit: 1) Increase the total number of smokers who make an attempt to quit, and 2) Increase the likelihood of success for each individual smoker.
Fortunately, policies that are major components of a comprehensive tobacco control policy, such as increased cigarette taxes and restrictions on where smokers can smoke, appear to promote quitting behavior. Further, there have been advances in the development and dissemination of effective treatments for tobacco dependence that enhance success rates.(1)
Although these treatments (both behavioral and pharmacologic) produce modest success rates, this improvement over unaided quitting can still lead to accelerations in population quitting behavior if they can be made available and accessible to wider populations of smokers.
This lecture will rely primarily on a published article to describe how reducing regulatory barriers to the access of pharmacotherapy offers promise for increasing its use and should contribute to population benefits in terms of increased quitting, based on data from the USA. The lecture will conclude with a poster presented at the 2000 11th World Conference on Tobacco OR Health that suggests that similar effects occur in countries outside of the US.
PUBLIC HEALTH IMPACT OF OVER-THE-COUNTER NICOTINE MEDICATIONS. (2) This was the first paper that characterized the benefit of reducing the regulatory barrier of requiring a physician's prescription in terms of expanding access. It relied on fairly short-term utilization data, but it indicated that utilization of nicotine medications greatly increased with their availability without a prescription. (copies of this article are available by request to the second author of this lecture ) USE OF FDA-APPROVED PHARMACOLOGIC TREATMENTS FOR TOBACCO DEPENDENCE Of the estimated 48 million adult smokers in the United States, approximately 16 million attempt to stop smoking cigarettes for at least 24 hours annually; another 2-3 million attempt to stop but cannot abstain for 24 hours (1). However, 1.2 million (2.5%) persons stop smoking each year (2). Although behavioral and pharmacologic methods
increase abstinence rates (3), most cessation attempts are undertaken without the benefit of treatment (4). In 1984, the Food and Drug Administration (FDA) approved the first pharmacologic aid for smoking cessation, nicotine gum. Since then, other treatments have become available. This study estimates the number of quit attempts using FDA approved pharmacologic aids during 1984-1998. The study results indicate that product use has changed over this period and that the availability of over-the-counter (OTC) products and the introduction of new products have increased pharmacologically assisted quit attempts.
Information about the sales of prescription smoking-cessation products was obtained from the National Data Corporation* (NDC) by the Source Prescription Audit (SPA). By 1991, the pharmacy sample included approximately 25,000 pharmacies and 75 million prescriptions filled nationally each month; by 1998, sales data included 34,000 pharmacies and 150 million prescriptions covering approximately 66% of the total number of prescriptions in the United States. The total number of prescriptions was obtained through an agreement with PCS Health Systems, Inc., which provides electronic claims services for almost every retail pharmacy.
Information about the sale of OTC products was based on data gathered by ACNielsen, a marketing research organization, that tallied purchases using an electronic Universal Product Code (UPC) scanner.
Scanner data were collected from a sample of 10,000 outlets located primarily in the top 50 U.S. markets.
Purchases from retail outlets without scanner technology were estimated from a sample of those stores.
The combined sample was weighted to estimate total purchases from all outlets. Purchase data from a representative panel of 40,000 households were used to estimate the proportion of unit sales of OTC nicotine replacement therapy (NRT) products representing new uses or quit attempts. The panel of households used a UPC scanner placed in their home to scan purchases after shopping. A new use or quit attempt was counted when an OTC product appeared for the first time in a household's data during a particular calendar year.
ACNielsen retail volume estimates were adjusted to project the total number of new OTC uses based on these data.
In 1992, the availability of prescription nicotine patches increased the estimated number of pharmacologically assisted quit attempts per year from 1-2 million to approximately 7 million (Figure 1).
The estimated number of quit attempts then decreased, ranging from 2 million to 3 million during 1993 -1995, but increased to approximately 6 million in 1996, coinciding with the availability of nicotine gum and the nicotine patch as OTC products. The estimated number of pharmacologically assisted quit attempts increased in 1997 and remained at that level in 1998. By 1998, the nicotine patch ac-counted for 49% of the pharmacologically assisted quit attempts, nicotine gum, 28%; Zyban, 21%; and nicotine inhaler and nasal spray, <3%. To examine the relation of use to medication availability, data were aggregated into periods marked by the introduction of new treatments and changes in the regulatory status of treatments.
In general, use has increased over time as availability improved, and to a lesser extent as new products were introduced. For example, the number of average monthly estimated quit attempts was 642,000 during May 1996-May 1997 when nicotine gum and patches became avail-able OTC, compared with 259,000 during January 1993-April 1996. The introduction of Zyban increased average monthly estimated quit attempts to 708,000.
*Use of trade names and commercial sources is for identification only and does not constitute endorsement by CDC or the U.S. Department of Health and Human Services.(3)
This paper provides an even broader perspective by showing trends of pharmacotherapy use since the availability of nicotine gum in 1984. It shows how the availability of the nicotine patch as a prescription-only product led to a brief period of high utilization in 1992, but that this was not sustained. This contrasts with the sustainability of the utilization with a mix of non-prescription and prescription products, with the large majority of pharmacotherapy being used via the non-prescription channel.
EXPANDED ACCESS AND PROMOTION OF PHARMACOLOGIC TREATMENT OF TOBACCO DEPENDENCE: FOUR NOVEL EXAMPLES Introduction Quitting among adult smokers is the primary method to reduce tobacco-related death and disease in the near term.
Despite that fact that pharmacotherapy is a widely recommended method to increase success rates among quitters, the majority of smokers attempt to quit by willpower alone.
Evidence from the U.S. and Australia has shown that in those countries, increased utilization of pharmacotherapy has resulted from: - Expansion of access (through regulatory changes) - ncreased product promotion and advertising (through regulatory and commercial changes).
Purpose: To assess the effects of increased product accessibility and promotion on pharmacotherapy utilization in 4 additional countries: Belgium, Brazil, France, and Mexico.
Methods Product advertising expenditures and utilization were tracked preceding and subsequent to marketplace changes in Belgium, Brazil, France, and Mexico.
Marketplace changes consisted of: - Policy changes in regulation (over-the-counter approval of NRT) - Increased product advertising (new product entry into open market).
Treatment utilization was measured by unit sales standardized into treatment weeks of each pharmacotherapy (package count divided by proscribed weekly dosing).
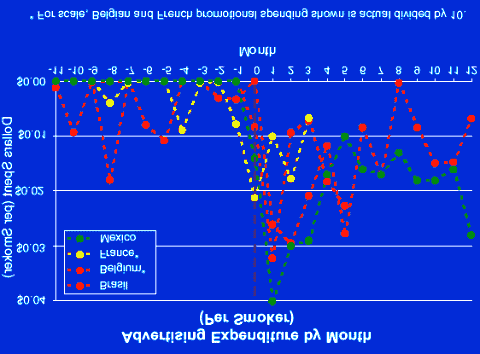
Per smoker advertising expenditure was generated by taking overall product advertising spending and dividing by smoking population within each country: - Belgium -Estimated 2.2 million smokers
- Brazil -Estimated 35.7 million smokers - France -Estimated 15.4 million smokers - Mexico -Estimated 15.6 million smokers.
Correlations between advertising expenditure and treatment utilization were calculated using Pearson correlation coefficients.
Results Both advertising expenditure (per smoker) and treatment utilization increased dramatically following the regulatory changes and/or the new product introductions in all markets (Fig. 2 and 3).
Within each country, increases in product advertising expenditure (per smoker) were significantly related to increased unit sales and, consequently, increased treatment weeks (all r >0.56; p <0.005).
Conclusions Enhanced availability and/or increased advertising and promotion of pharmacotherapy results in increased utilization across a variety of countries.
These data cannot indicate whether the increase in product utilization is coming from those who would have tried to quit anyway (but who would have quit without assistance) or from new quitters.
Given that these treatments have been consistently shown to significantly increase quit rates, it is reasonable to conclude that this increase in product utilization should result in more successful quits and thus public health gains.
Barriers to marketing investment in the treatment market for proven safe and efficacious products should be minimized to increase the number of quit attempts utilizing pharmacotherapy.
Limitations "Treatment weeks" is a variable used as a surrogate of quitting behavior; actual increases in quitting behavior can only be assessed using population surveys.
This paper provides promising evidence that realizing the benefits of increased access and promotion of treatment for tobacco dependence is not unique to the USA. The examples from four different countries (Belgium, Brazil, France, and Mexico) all point to the ability for reducing barriers to access and increasing promotion to increase the utilization of effective treatments.
DISCUSSION There remain other barriers to lower to further increase access and use of effective treatments. Many smokers have concerns that the pharmacologic treatments are not safe to use to quit smoking, and thus they either do not use them at all, or they use them for too short a period.
Another barrier is the cost of these treatments, especially since they are not generally offered in the same "daily supply" packages that cigarettes are. Most pharmacotherapy can only be purchased in one-week or longer supplies, so that even if the "per day" cost is similar to that of cigarettes, the initial expenditure is much greater.
While this presentation suggests that progress has been made in the effort to increase quitting, it is clear that much more needs to be done to achieve the goal of maximally reducing cigarette smoking as quickly as possible. A significant opportunity that can complement the broader access of available pharmacotherapies is increased training for health care professionals so that they are more comfortable and able to intervene with their patients who smoke. Health care professionals can fulfill an important role by encouraging their patients who smoke to quit and by directing them to treatments that will increase their chances of success.
REFERENCES
1. Fiore MC, Bailey WC, Cohen SJ, et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, MD:
U.S. Department of Health and Human Services. Public Health Service. June 2000.
2. Shiffman S, Gitchell J, Pinney J, Burton SL, Kemper KE, Lara EA. Public health impact of over-the-counter nicotine medications. Tobacco Control 1997; 6: 306-310.
3. Centers of Disease Control and Prevention. Use of FDA-approved pharmacologic treatments for tobacco dependence.
Morbidity and Mortality Weekly Report 2000; 49: 665-668
Your questions, contributions and commentaries will be answered
by the lecturer or experts on the subject in the Prevention and Epidemiology list.
Please fill in the form (in Spanish, Portuguese or English) and press the "Send" button.
Send Erase 2nd Virtual Congress of Cardiology Dr. Florencio Garófalo Dr. Raúl Bretal Dr. Armando Pacher fgaro@fac.org.ar rbretal@fac.org.ar apacher@fac.org.ar fgaro@satlink.com rbretal@netverk.com.ar apacher@satlink.com
Copyright 1999-2001 Argentine Federation of Cardiology
This company contributed to the Congress:
First Aid Kit Requirements Each backpacker MUST have a first aid kit that is fully supplied and maintained in a ready state. This kit must be carried by each backpacker and cannot be shared to save weight. In overview, the kit contents must include an assortment of different types of bandages for wound management, materials for blister management, gauze and tape, antibiotic ointment, antiba
ANDREW B. SILVA, MD VIRGINIA HEAD AND NECK SURGEONS P.C. HERE’S WHAT TO DO IF A NOSE BLEED STARTS: Sit down or lay down with your head propped up on 2 or 3 pillows. Keep calm and remember many nose bleeds will stop all by themselves if you just rest for a few minutes. If you are driving or operating heavy or dangerous equipment stop. Put an ice pack on your nose . Get a thin washclot
 Home SVCC Area: English - Español - Português
Home SVCC Area: English - Español - Português 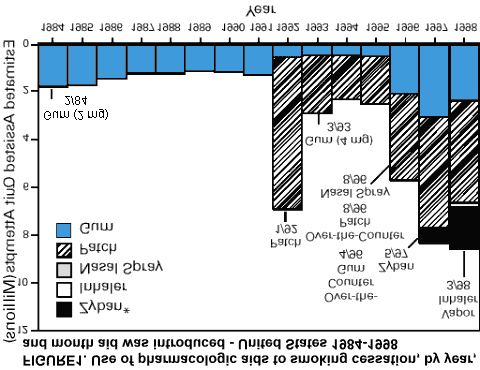 increase abstinence rates (3), most cessation attempts are undertaken without the benefit of treatment (4). In 1984, the Food and Drug Administration (FDA) approved the first pharmacologic aid for smoking cessation, nicotine gum. Since then, other treatments have become available. This study estimates the number of quit attempts using FDA approved pharmacologic aids during 1984-1998. The study results indicate that product use has changed over this period and that the availability of over-the-counter (OTC) products and the introduction of new products have increased pharmacologically assisted quit attempts.
Information about the sales of prescription smoking-cessation products was obtained from the National Data Corporation* (NDC) by the Source Prescription Audit (SPA). By 1991, the pharmacy sample included approximately 25,000 pharmacies and 75 million prescriptions filled nationally each month; by 1998, sales data included 34,000 pharmacies and 150 million prescriptions covering approximately 66% of the total number of prescriptions in the United States. The total number of prescriptions was obtained through an agreement with PCS Health Systems, Inc., which provides electronic claims services for almost every retail pharmacy.
Information about the sale of OTC products was based on data gathered by ACNielsen, a marketing research organization, that tallied purchases using an electronic Universal Product Code (UPC) scanner.
Scanner data were collected from a sample of 10,000 outlets located primarily in the top 50 U.S. markets.
Purchases from retail outlets without scanner technology were estimated from a sample of those stores.
The combined sample was weighted to estimate total purchases from all outlets. Purchase data from a representative panel of 40,000 households were used to estimate the proportion of unit sales of OTC nicotine replacement therapy (NRT) products representing new uses or quit attempts. The panel of households used a UPC scanner placed in their home to scan purchases after shopping. A new use or quit attempt was counted when an OTC product appeared for the first time in a household's data during a particular calendar year.
ACNielsen retail volume estimates were adjusted to project the total number of new OTC uses based on these data.
In 1992, the availability of prescription nicotine patches increased the estimated number of pharmacologically assisted quit attempts per year from 1-2 million to approximately 7 million (Figure 1).
The estimated number of quit attempts then decreased, ranging from 2 million to 3 million during 1993 -1995, but increased to approximately 6 million in 1996, coinciding with the availability of nicotine gum and the nicotine patch as OTC products. The estimated number of pharmacologically assisted quit attempts increased in 1997 and remained at that level in 1998. By 1998, the nicotine patch ac-counted for 49% of the pharmacologically assisted quit attempts, nicotine gum, 28%; Zyban, 21%; and nicotine inhaler and nasal spray, <3%. To examine the relation of use to medication availability, data were aggregated into periods marked by the introduction of new treatments and changes in the regulatory status of treatments.
In general, use has increased over time as availability improved, and to a lesser extent as new products were introduced. For example, the number of average monthly estimated quit attempts was 642,000 during May 1996-May 1997 when nicotine gum and patches became avail-able OTC, compared with 259,000 during January 1993-April 1996. The introduction of Zyban increased average monthly estimated quit attempts to 708,000.
*Use of trade names and commercial sources is for identification only and does not constitute endorsement by CDC or the U.S. Department of Health and Human Services.(3)
This paper provides an even broader perspective by showing trends of pharmacotherapy use since the availability of nicotine gum in 1984. It shows how the availability of the nicotine patch as a prescription-only product led to a brief period of high utilization in 1992, but that this was not sustained. This contrasts with the sustainability of the utilization with a mix of non-prescription and prescription products, with the large majority of pharmacotherapy being used via the non-prescription channel.
EXPANDED ACCESS AND PROMOTION OF PHARMACOLOGIC TREATMENT OF TOBACCO DEPENDENCE: FOUR
increase abstinence rates (3), most cessation attempts are undertaken without the benefit of treatment (4). In 1984, the Food and Drug Administration (FDA) approved the first pharmacologic aid for smoking cessation, nicotine gum. Since then, other treatments have become available. This study estimates the number of quit attempts using FDA approved pharmacologic aids during 1984-1998. The study results indicate that product use has changed over this period and that the availability of over-the-counter (OTC) products and the introduction of new products have increased pharmacologically assisted quit attempts.
Information about the sales of prescription smoking-cessation products was obtained from the National Data Corporation* (NDC) by the Source Prescription Audit (SPA). By 1991, the pharmacy sample included approximately 25,000 pharmacies and 75 million prescriptions filled nationally each month; by 1998, sales data included 34,000 pharmacies and 150 million prescriptions covering approximately 66% of the total number of prescriptions in the United States. The total number of prescriptions was obtained through an agreement with PCS Health Systems, Inc., which provides electronic claims services for almost every retail pharmacy.
Information about the sale of OTC products was based on data gathered by ACNielsen, a marketing research organization, that tallied purchases using an electronic Universal Product Code (UPC) scanner.
Scanner data were collected from a sample of 10,000 outlets located primarily in the top 50 U.S. markets.
Purchases from retail outlets without scanner technology were estimated from a sample of those stores.
The combined sample was weighted to estimate total purchases from all outlets. Purchase data from a representative panel of 40,000 households were used to estimate the proportion of unit sales of OTC nicotine replacement therapy (NRT) products representing new uses or quit attempts. The panel of households used a UPC scanner placed in their home to scan purchases after shopping. A new use or quit attempt was counted when an OTC product appeared for the first time in a household's data during a particular calendar year.
ACNielsen retail volume estimates were adjusted to project the total number of new OTC uses based on these data.
In 1992, the availability of prescription nicotine patches increased the estimated number of pharmacologically assisted quit attempts per year from 1-2 million to approximately 7 million (Figure 1).
The estimated number of quit attempts then decreased, ranging from 2 million to 3 million during 1993 -1995, but increased to approximately 6 million in 1996, coinciding with the availability of nicotine gum and the nicotine patch as OTC products. The estimated number of pharmacologically assisted quit attempts increased in 1997 and remained at that level in 1998. By 1998, the nicotine patch ac-counted for 49% of the pharmacologically assisted quit attempts, nicotine gum, 28%; Zyban, 21%; and nicotine inhaler and nasal spray, <3%. To examine the relation of use to medication availability, data were aggregated into periods marked by the introduction of new treatments and changes in the regulatory status of treatments.
In general, use has increased over time as availability improved, and to a lesser extent as new products were introduced. For example, the number of average monthly estimated quit attempts was 642,000 during May 1996-May 1997 when nicotine gum and patches became avail-able OTC, compared with 259,000 during January 1993-April 1996. The introduction of Zyban increased average monthly estimated quit attempts to 708,000.
*Use of trade names and commercial sources is for identification only and does not constitute endorsement by CDC or the U.S. Department of Health and Human Services.(3)
This paper provides an even broader perspective by showing trends of pharmacotherapy use since the availability of nicotine gum in 1984. It shows how the availability of the nicotine patch as a prescription-only product led to a brief period of high utilization in 1992, but that this was not sustained. This contrasts with the sustainability of the utilization with a mix of non-prescription and prescription products, with the large majority of pharmacotherapy being used via the non-prescription channel.
EXPANDED ACCESS AND PROMOTION OF PHARMACOLOGIC TREATMENT OF TOBACCO DEPENDENCE: FOUR 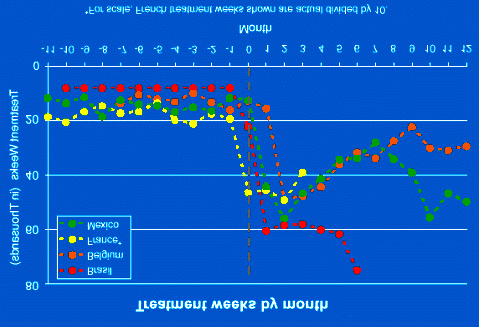
 - Brazil -Estimated 35.7 million smokers - France -Estimated 15.4 million smokers - Mexico -Estimated 15.6 million smokers.
Correlations between advertising expenditure and treatment utilization were calculated using Pearson correlation coefficients.
Results
- Brazil -Estimated 35.7 million smokers - France -Estimated 15.4 million smokers - Mexico -Estimated 15.6 million smokers.
Correlations between advertising expenditure and treatment utilization were calculated using Pearson correlation coefficients.
Results  Your questions, contributions and commentaries will be answered
by the lecturer or experts on the subject in the Prevention and Epidemiology list.
Please fill in the form (in Spanish, Portuguese or English) and press the "Send" button.
Send Erase
Your questions, contributions and commentaries will be answered
by the lecturer or experts on the subject in the Prevention and Epidemiology list.
Please fill in the form (in Spanish, Portuguese or English) and press the "Send" button.
Send Erase