Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Dickibus.co.uk
CASE REPORT Omental Transplantation for Temporal Lobe Epilepsy : Report of Two Cases H. Rafael, R. Mego, P. Moromizato,* W. Garcia*
Universidad Nacional Autonoma de Mexico (UNAM)
Departments of General Surgery and Anesthesiology*
Instituto Mexicano Del Seguro Social (IMSS)
The authors present two patients, with poorly controlled temporal lobe epilepsy, who received transplants of omental tissue on the anterior perforated space and left temporal lobe. At present, 26 months after the operation, the first patient has improved about 85 percent; whereas the second patient has complete control of seizures nine months after the operation. These clinical results indicate that epileptic seizures can be reduced or aborted with this new surgical modality (reconstructive technique). Key words : Complex partial seizures, Epileptogenic zone, Omental transplantation. Introduction
controlled epileptic seizures and treated by transplantsof omental tissue on the epileptogenic zone are
The epilepsy surgery began in 1886, when Victor
Horsley treated three patients with refractory seizuresby surgical ablation of the epileptogenic zone.1 Since
Case Report
then and upto now, three essential procedures are usedat many neurosurgical centers2-4 : i) surgical ablation,
Case 1 : A 33 year old right handed woman, had a 21
ii) disconnection procedures and iii) vagus nerve
year history of medically refractory epilepsy. During
these years, she had been treated with severalantiepileptic drugs. Since 1995, she had received
However, since May 6, 1988 the authors have used a
clonazepam 5 mg/day and oxcarbazepine 1200 to
new surgical technique for patients with ischemic
1500 mg/day. During the last 3 years she had three
infarct and epilepsy.5,6 Two patients with poorly
spontaneous abortions between 6 to 13 weeks ofpregnancy.
Correspondence to : Dr. H. Rafael, Belgica 411-BIS, ColoniaPortales, 03300 Mexico City, Mexico.
During seizures she had tonic flexion of her right
hand, palpitation, motor dysphasia and paleness,
Omental Transplantation in Intractable Epilepsy
associated with partial impairment of consciousnessfor several seconds, and with a frequency of about 20episodes per month. She also had 2-3 generalizedtonic-clonic seizures per month, especially during themenstrual period. Postictally, she had moderate globaldysphasia, memory impairment and headache for 30to 60 minutes. In the interictal period, she hadepisodes of headache, irritability, motor dysphasia,sleep disorders and impairment of recent memory.
Neurological examination revealed normal motor andsensory functions. Neuropsychological testingshowed essentially recent memory impairment, slightmotor dysphasia,
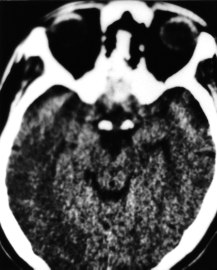
Extracranial interictal electroencephalogram showedwell localized epileptiform discharges in the lefttemporal region and, occasionally, generalizedatypical spikes. A preoperative computerizedtomography (CT) scan showed severe atrophy in bothtemporal lobes, especially in the left medial temporallobe and probable heterotopia or sclerosis in a smallarea of the left temporo-occipital cortex. The clinicalpre and postoperative picture was recorded on videotape, and the surgery was performed on April 18,1998
Fig. 1 : Preoperative CT scan without contrast showing
moderate atrophy in the anteromedial surface of the lefttemporal lobe. Case 2 : A 33 year old right handed man was admittedto hospital epileptic seizures, sleep disorders and
clonic seizures,7 due to a principal lesion in the medial
progressive impairment of recent memory. During the
temporal lobe, omental tissue (free omental flap with
last 28 years, he had been treated with many anti-
vascular microanastomosis) was transplanted on the
epileptic medicaments. Since 1997, he had received
anterior perforated space (APS) and left temporal
clonazepam 5 mg/day and sodium valproate 520
lobe.8,9 An omental segment was placed on the APS
mg/day. He had olfactory hallucinations, palpitations,
(posterior and lateral zone) and medial surface of the
paleness, stuttering and partial impairment of
left temporal lobe and another omental segment on the
consciousness for few seconds, with a frequency of
inferior and lateral surface of the same temporal lobe.
about 12 episodes per month. He had 0-2 generalizedtonic-clonic seizures per month. Postictally, he had
moderate global dysphasia, memory impairment,headache and sickness for about two hours. In the
In both patients, recent memory and sleep disorders
interictal period, he had episodes of headache,
improvement occurred on the third day after surgery.
stuttering, sleep disorders and lately, impairment of
By June 2000, the first patient was having between
0-4 preictal seizures per month (earlier 20 months)and only five generalized tonic-clonic seizures during
Neuropsychological testing revealed frequent
these 26 months postoperative (earlier 2-3 months).
stuttering, agitation, anxiety and recent memory
She is on clonazepam 3 mg in the night and
impairment. An interictal electroencephalogram
oxcarbazepine 600 mg/day. During this postoperative
revealed epileptiform discharges, most pronounced at
course, the seizure occurred more frequently in the
the left temporal lobe. A preoperative CT scan showed
first few months; the severity and duration of epileptic
moderate atrophy in both the temporal lobes,
attacks still being less than that before surgery.
especially in the anteromedial portion of the left
Moreover, in the intervening period, she had a
temporal lobe (Fig. 1). Surgery was carried out on
pregnancy and normal delivery. Her postoperative CT
scans (June 1,1999) showed the omental tissue on themedial and lateral surface of the left temporal lobe, as
Surgical Procedure : With the diagnosis of complex
well as revascularization of the underlying cerebral
partial seizures with or without generalized tonic-
Thus, the functional recovery of neurons and axons inthe epileptic foci (residual nervous tissue)5,6 inischemic and ischemic penumbra region can improve,if the blood flow is increased or reinstituted throughthe omentum. Therefore, interictal hypoperfusion13,14and hypometabolism15 of the epileptic foci arenormalized and likewise, extracellular concentrationof glutamate and aspartate,16 and the neuronalhyperexcitability are reduced.13,17
Although pre and postoperatively regional cerebralblood flow was not measured by positron emissiontomography (PET) or single photon emissioncomputed tomography (SPECT) in the present twopatients, the neurological improvement previouslyobtained after omental transplantation on the APS inpatients with essential arterial hypertension,18,19Alzheimer’s disease,20 and late sequelae of the basalganglia, the internal capsule and the thalamus8,9,12demonstrate the efficacy of the transplanted omentum.
In the author’s opinion, the success of the pregnancyin the first patient was also due to a functional
Fig. 2 : Postoperative CT scan with contrast obtained 5 days
recovery of the neuronal hyper-excitability21-23 in the
after surgery, showing the omentum on the anteromedial and
medial temporal lobe and its efferent projections via
lateral surface as well as revascularization into the underlying
the fornix towards the neuroendocrine cells within the
hypothalamus23,24 and subcommissural region.20,24
The second patient, 9 months postoperative, had 80%improvement in stuttering. He was getting only
Conclusion
clonazepam 2 mg at night. His postoperative CT scans(September 12, 1999) showed the omentum on the
The present two patients demonstrate that interictal
medial and lateral surface of the left temporal lobe as
focus must be revascularized in order to revert to the
well as revascularization of the underlying brain
progressive hypoperfusion and hypometabolism,
(Fig. 2). During the nine months after the operation,
which produces increased epileptogenicity. Likewise,
this surgical technique led to a complete control of
the authors believe that by means of this surgical
procedure (reconstructive technique), the neuronalloss and the astrocytic gliosis can be stopped.
Discussion References
These results demonstrate that placing omental tissuedirectly upon the epileptic focus (medial temporal
Horsley V : Brain surgery. BMJ 1886; 2 : 670-675.
lobe structures) and neighbouring areas (posterior
Penfield W : The radical treatment of traumatic epilepsy and
hypothalamus, subcommissural region and extreme
its rationale. Can Med Assoc 1930; 23 : 189-197.
superior of mesencephalic reticular nucleus), can
3. The vagus nerve stimulation study group. A randomized
reduce or abort complex partial seizures and confirm
controlled trial of the chronic vagus nerve stimulation for
our previous clinical experiences5,6 as well as of other
treatment of medically intractable seizures. Neurology 1995; 45 : 224-230.
authors.10 The omentum11,12 is used because it is the
Queenan JV, Germano IM : Advances in the neurosurgical
best tissue to provoke the neoformation of blood
management of adult epilepsy. Contemp Neurosurg 1997;
vessels (revascularization) and through these vessels,
the underlying and adjacent brain receives an increase
Rafael H : Commentary on human hippocampal structures.
in blood flow, oxygen, omental neurotransmitters
J Chil Neurol 1998; 13 : 146-147.
(dopamine, noradrenaline and acetylcholine) and
Rafael H : Surgical and neurological complications in a
neurotrophic factors (nerve growth factor and
series of 708 epilepsy surgical procedures. Neurosurgery
1998; 42 : 675-676.
Omental Transplantation in Intractable Epilepsy
7. Commission on classification and terminology of the
17. Lopez E, Parra L, Bravo J et al : Cambios en la excitabilidad
International League Against Epilepsy. Proposal for revised
neuronal y alteraciones en la densidad neuronal del
clinical and electroencephalographic classification of
hipocampo inducidos por isquemia local. Arch Neuroscien
epileptic seizures. Epilepsia 1981; 22 : 489-501.
(Mex) 1997; 2 : 61-66.
8. Rafael H : Transsylvian and transinsular approach. Turk
18. Rafael H : Microvascular decompression of the left lateral
Neurosurg 1995; 5 : 53-56.
medulla oblongata for severe refractory neurogenic
Rafael H, Moromizato P, del Angel J et al : Trasplante de
hypertension. Neurosurgery 1999; 44 : 691-692.
epiplon para infarto isquemico del cerebro. Cir Ciruj (Mex)
Rafael H : Hipertension arterial esencial : Un analisis
1998; 66 : 155-158.
neurologico sobre su etiologia. Hipertension (Mex) 2000; 20
10. May CH, Vogel Is : Epilepsia partialis continua successfully
treated by transplantation of omentum : Case report.
20. Rafael H, Mego R, Moromizato P et al : Omental
Presented at the First International Congress of Omentum in
transplantation for Alzheimer’s disease : case report. Neurol
India 2000; 48 : 319-321.
11. Goldsmith HS : The omentum : research and clinical
21. Logothetis J, Harner R : Electrocortical activitation by
applications. Springer-Verlag, New York. 1990; 5-245.
estrogens. Arch Neurol 1960; 3 : 290-297.
12. Rafael H : El epiplon : Trasplante al sistema nervioso.
22. Laplante P, Saint-Hilaire JM, Bouvier G : Headache as an
Mexico, DF : Editorial Prado 1996; 1-171.
epileptic manifestation. Neurology 1983; 33 : 1493-1495.
Weinand ME, Carter LP, El-Saadany WF et al : Cerebral
23. Woolley CS : Structural and electrophysiological effects of
blood flow and temporal lobe epileptogenicity. J Neurosurg
estradiol may increase the likelihood of seizures. Epilepsia
1997; 86 : 226-232.
1998; 39 (Suppl 6) : 210-211.
14. Rougier A, Lurton D, EI Bahh B et al : Bilateral decrease in
24. Pfaff DW, McEwen BS : Actions of estrogens and progestins
interictal hippocampal blood flow in unilateral mesiotemporal
on the nerve cells. Science 1983; 219 : 808-814.
epilepsy. J Neurosurg 1999; 90 : 282-288.
15. Blum DE, Ehsan T, Dungan D et al : Bilateral temporal
hypometabolism in epilepsy. Epilepsia 1998; 39 : 651-659.
16. Benbeniste H, Drejer J, Schousboe A et al : Elevation of the
extracellular concentration of glutamate and aspartate in rat hippocampus during transient cerebral ischemia monitored by intracerebral microdialysis. J Neurochem 1984; 43 : 1369-1374.
Accepted for publication : 9th August, 2001.
BUNDESJUNIORCUP 2012 Vorstieg: Österreichische Meisterschaft für Kinder und Jugend Klassen: Dornbirn 12./13. Mai 2012 Kinder weiblich Qualifikation 1/2 Finale Rg. Name Vorname Sektion/Land 1.Dg 1.Pk Rg.1 2.Dg 2.Pk Rg.2 Gp. RQ Fin Kl_Zeit 1 Winkler Julia 2 Kruckenhauser Lisa 3 Lettner Sandra ** 4 Lammer Laura 5 Wittauer Christina 6 Scho
RESEARCH PROGRAMME OVERVIEW Attempts to Identify New Therapeutic Targets for Triple-Negative Breast Cancer Targeted therapy is currently available for the majority of patients with newly diagnosed breast cancer. Thus, patients with estrogen receptor (ER)-positive and/or progesterone receptor (PR)-positive disease receive hormone therapy, while patients with HER2-postive disease may be treat
 Omental Transplantation in Intractable Epilepsy
associated with partial impairment of consciousnessfor several seconds, and with a frequency of about 20episodes per month. She also had 2-3 generalizedtonic-clonic seizures per month, especially during themenstrual period. Postictally, she had moderate globaldysphasia, memory impairment and headache for 30to 60 minutes. In the interictal period, she hadepisodes of headache, irritability, motor dysphasia,sleep disorders and impairment of recent memory.
Neurological examination revealed normal motor andsensory functions. Neuropsychological testingshowed essentially recent memory impairment, slightmotor dysphasia,
Extracranial interictal electroencephalogram showedwell localized epileptiform discharges in the lefttemporal region and, occasionally, generalizedatypical spikes. A preoperative computerizedtomography (CT) scan showed severe atrophy in bothtemporal lobes, especially in the left medial temporallobe and probable heterotopia or sclerosis in a smallarea of the left temporo-occipital cortex. The clinicalpre and postoperative picture was recorded on videotape, and the surgery was performed on April 18,1998
Fig. 1 : Preoperative CT scan without contrast showing
Omental Transplantation in Intractable Epilepsy
associated with partial impairment of consciousnessfor several seconds, and with a frequency of about 20episodes per month. She also had 2-3 generalizedtonic-clonic seizures per month, especially during themenstrual period. Postictally, she had moderate globaldysphasia, memory impairment and headache for 30to 60 minutes. In the interictal period, she hadepisodes of headache, irritability, motor dysphasia,sleep disorders and impairment of recent memory.
Neurological examination revealed normal motor andsensory functions. Neuropsychological testingshowed essentially recent memory impairment, slightmotor dysphasia,
Extracranial interictal electroencephalogram showedwell localized epileptiform discharges in the lefttemporal region and, occasionally, generalizedatypical spikes. A preoperative computerizedtomography (CT) scan showed severe atrophy in bothtemporal lobes, especially in the left medial temporallobe and probable heterotopia or sclerosis in a smallarea of the left temporo-occipital cortex. The clinicalpre and postoperative picture was recorded on videotape, and the surgery was performed on April 18,1998
Fig. 1 : Preoperative CT scan without contrast showing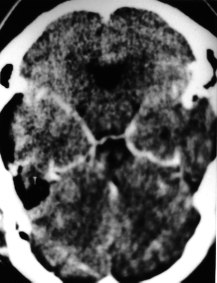 Thus, the functional recovery of neurons and axons inthe epileptic foci (residual nervous tissue)5,6 inischemic and ischemic penumbra region can improve,if the blood flow is increased or reinstituted throughthe omentum. Therefore, interictal hypoperfusion13,14and hypometabolism15 of the epileptic foci arenormalized and likewise, extracellular concentrationof glutamate and aspartate,16 and the neuronalhyperexcitability are reduced.13,17
Although pre and postoperatively regional cerebralblood flow was not measured by positron emissiontomography (PET) or single photon emissioncomputed tomography (SPECT) in the present twopatients, the neurological improvement previouslyobtained after omental transplantation on the APS inpatients with essential arterial hypertension,18,19Alzheimer’s disease,20 and late sequelae of the basalganglia, the internal capsule and the thalamus8,9,12demonstrate the efficacy of the transplanted omentum.
Thus, the functional recovery of neurons and axons inthe epileptic foci (residual nervous tissue)5,6 inischemic and ischemic penumbra region can improve,if the blood flow is increased or reinstituted throughthe omentum. Therefore, interictal hypoperfusion13,14and hypometabolism15 of the epileptic foci arenormalized and likewise, extracellular concentrationof glutamate and aspartate,16 and the neuronalhyperexcitability are reduced.13,17
Although pre and postoperatively regional cerebralblood flow was not measured by positron emissiontomography (PET) or single photon emissioncomputed tomography (SPECT) in the present twopatients, the neurological improvement previouslyobtained after omental transplantation on the APS inpatients with essential arterial hypertension,18,19Alzheimer’s disease,20 and late sequelae of the basalganglia, the internal capsule and the thalamus8,9,12demonstrate the efficacy of the transplanted omentum.