Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
How to record uterine artery doppler in the first trimester
Ultrasound Obstet Gynecol 2013; 42: 478–479 Published online 8 May 2013 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.12366
How to . . . Practical advice on imaging-based techniques and investigations with
accompanying slides and videoclips online
How to record uterine artery Doppler in the first trimester *Department of Fetal Medicine, Institute for Women’s Health, University College London Hospitals, London, UK; †Harris BirthrightResearch Centre for Fetal Medicine, King’s College Hospital, London, UKBACKGROUND
Effective screening for pre-eclampsia can be achieved bymeasurement of the uterine artery pulsatility index (PI) at11–13 weeks’ gestation, used in combination with mater-nal history, blood pressure, serum pregnancy-associatedplasma protein-A and placental growth factor1. For afalse-positive rate of 5%, it has been estimated thatthe new combined method of screening can predict90% of cases of pre-eclampsia requiring delivery before34 weeks and 45% of cases of late-onset pre-eclampsia2,3. Early-onset, rather than late-onset, pre-eclampsia isassociated with an increased risk of perinatal morbidityand mortality, and both short-term and long-termmaternal complications. Early identification of women atrisk of developing pre-eclampsia and growth restrictionis likely to facilitate targeted antenatal surveillance and
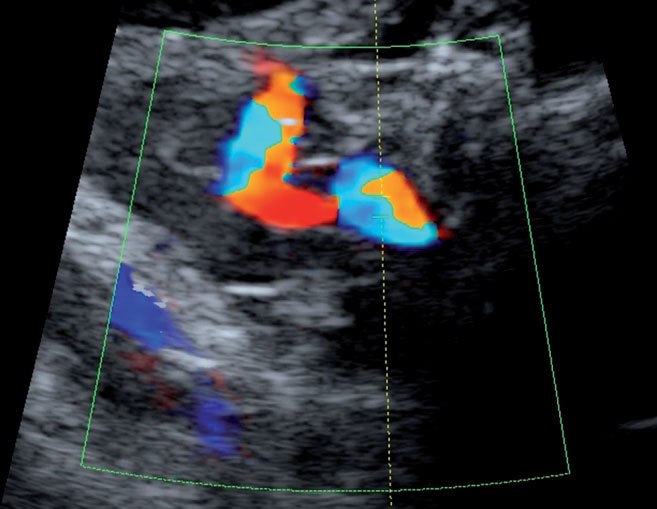
Figure 1 Parasagittal section of the uterus and cervix. Color flow
possibly intervention. It would also potentially avoid
mapping is used to identify the uterine arteries as aliasing vessels
the development of serious complications, through
coursing along the side of the cervix and uterus.
interventions such as administration of low-dose aspirinand antihypertensive medication, and early delivery4.
For uterine artery PI measurement, the gestational age
PRACTICAL POINTS
must be between 11 + 0 and 13 + 6 weeks. Transabdom-inal ultrasound should be used to obtain a midsagittalsection of the uterus and cervical canal. The internal
1. Obtain a sagittal section of the uterus and cervical
cervical os should be identified and the transducer tilted
canal. Zoom to the area of interest.
gently from side to side in each paracervical region, using
2. Identify the internal cervical os. Gently tilt the
color flow mapping, to identify the uterine arteries as
transducer from side to side using color flow mapping
aliasing vessels coursing along the side of the cervix and
to identify the uterine arteries. When you apply color
uterus (Figure 1). Pulsed wave Doppler should be used
Doppler, narrow the color box and adjust the velocity
to obtain flow velocity waveforms from the ascending
branch of the uterine artery at the point closest to the
3. Apply pulsed wave Doppler with the sampling gate
internal os. When three similar consecutive waveforms
set at 2 mm to cover the whole vessel. Ensure that the
are obtained, the PI should be measured and the mean PI
angle of insonation is < 30◦.
of the left and right arteries calculated5 (Figure 2).
4. Record at least three consecutive uniform waveforms. Correspondence to: Prof. K. H. Nicolaides, Harris Birthright Research Centre for Fetal Medicine, King’s College Hospital, Denmark Hill,London SE5 9RS, UK (e-mail: kypros@fetalmedicine.com)
Copyright 2013 ISUOG. Published by John Wiley & Sons Ltd. Figure 2 (a) The ascending branch of the uterine artery at its paracervical portion and at the point closest to the internal os is identified and pulsed wave Doppler is used to obtain flow velocity waveforms. (b) When three similar consecutive waveforms are obtained, the pulsatility index (PI) should be measured and the mean PI of the left and right arteries calculated. The PI is calculated as the difference between the peak systolic velocity (S) and the end-diastolic velocity (D), divided by the mean velocity (Vm): PI = (S−D)/Vm. REFERENCES
age at 11–13 weeks. Fetal Diagn Ther 2012 [Epub ahead ofprint].
4. Bujold E, Roberge S, Lacasse Y, Bureau M, Audibert F,
1. Nicolaides KH. Turning the pyramid of prenatal care. Fetal
Marcoux S, Forest JC, Gigu`ere Y. Prevention of pre-eclampsia
Diagn Ther 2011; 29:183–196.
and intrauterine growth restriction with aspirin started in
2. Akolekar R, Syngelaki A, Sarquis R, Zvanca M, Nicolaides
early pregnancy: a meta-analysis. Obstet Gynecol 2010; 116:
KH. Prediction of early, intermediate and late pre-eclampsia
from maternal factors, biophysical and biochemical markers at
5. Martin AM, Bindra R, Curcio P, Cicero S, Nicolaides KH.
11–13 weeks. Prenat Diagn 2011; 31: 66–74.
Screening for pre-eclampsia and fetal growth restriction by
3. Poon LC, Syngelaki A, Akolekar R, Lai J, Nicolaides KH.
uterine artery Doppler at 11–14 weeks of gestation. Ultrasound
Combined screening for preeclampsia and small for gestational
Obstet Gynecol 2001; 18: 583–586.
Slides summarizing practical points, withaccompanying illustrations and videoclips,are provided as supporting informationonline.
Copyright 2013 ISUOG. Published by John Wiley & Sons Ltd. Ultrasound Obstet Gynecol 2013; 42: 478–479.
Dictionary Adjuvant therapy (AD-joo-vant) — Any additional treatment that is given after a cancer is removed surgically. Adjuvant therapy may include chemotherapy, radiation therapy, or hormonal therapy. Areola (a-REE-o-la) — The area of dark-colored skin on the breast that surrounds the nipple. Aromatase Inhibitor — Medication given to post menopausal estrogen receptor-po
Advice to athletes on the use of supplements in sport POSITION STATEMENT of UK Sport, the British Olympic What is the difference between a medicine and a Association (BOA), the British Paralympic Association (BPA), supplement? National Sports Medicine Institute (NSMI), and the Home Country Sports Councils (HCSC) Athletes should be aware that any product that claims to restore,
 Ultrasound Obstet Gynecol 2013; 42: 478–479
Ultrasound Obstet Gynecol 2013; 42: 478–479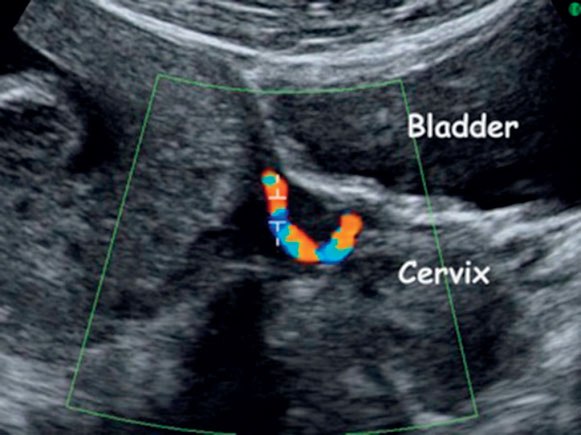
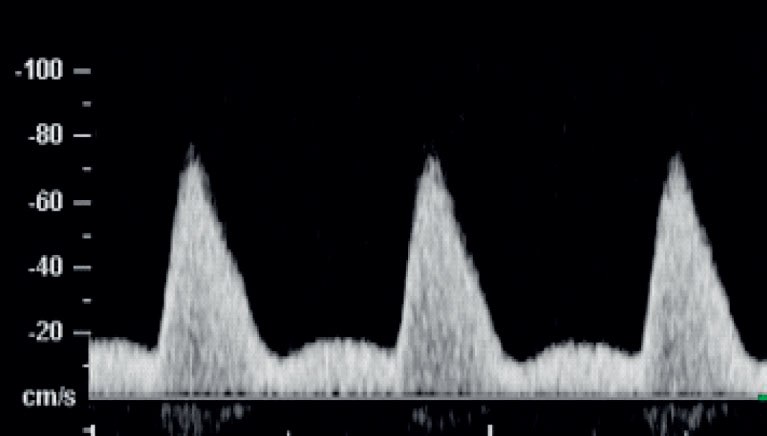
 Figure 2 (a) The ascending branch of the uterine artery at its paracervical portion and at the point closest to the internal os is identified and
Figure 2 (a) The ascending branch of the uterine artery at its paracervical portion and at the point closest to the internal os is identified and