Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
A randomized trial comparing fluconazole with clotrimazole troches for the prevention of fungal infections in patients with advanced human immunodeficiency virus infection
A RANDOMIZED TRIAL COMPARING FLUCONAZOLE WITH CLOTRIMAZOLE TROCHES FOR THE PREVENTION OF FUNGAL INFECTIONS IN PATIENTS WITH ADVANCED HUMAN IMMUNODEFICIENCY VIRUS INFECTION
WILLIAM G. POWDERLY, M.D., DIANNE M. FINKELSTEIN, PH.D., JUDITH FEINBERG, M.D., PETER FRAME, M.D.,
WEILI HE, M.S., CHARLES VAN DER HORST, M.D., SUSAN L. KOLETAR, M.D., M. ELAINE EYSTER, M.D.,
JOHN CAREY, M.D., HETTY WASKIN, M.D., THOMAS M. HOOTON, M.D., NEWTON HYSLOP, M.D.,
STEPHEN A. SPECTOR, M.D., AND SAMUEL A. BOZZETTE, M.D., PH.D.,
FOR THE NIAID AIDS CLINICAL TRIALS GROUP*
Abstract
azole group and 15 in the clotrimazole group; adjusted
other serious fungal infections are common complications
relative hazard, 8.5; 95 percent confidence interval, 1.9 to
in patients infected with the human immunodeficiency vi-
37.6). The benefit of fluconazole was greater for the pa-
rus (HIV). Fluconazole is effective for long-term suppres-
tients with 50 or fewer CD4ϩ cells per cubic millimeter
sion of many fungal infections, but its effectiveness as pri-
than for the patients with higher counts. Fluconazole was
mary prophylaxis had not been adequately evaluated.
also effective in preventing esophageal candidiasis (ad-
justed relative hazard, 5.8; 95 percent confidence interval,
trial that compared fluconazole (200 mg per day) with clo-
1.7 to 20.0; Pϭ0.004) and confirmed and presumed oro-
trimazole troches (10 mg taken five times daily) in patients
pharyngeal candidiasis (5.7 and 38.1 cases per 100 per-
who were also participating in a randomized trial of pri-
son-years of follow-up in the fluconazole and clotrimazole
mary prophylaxis for Pneumocystis carinii pneumonia.
groups, respectively; PϽ0.001). Survival was similar in
After a median follow-up of 35 months, inva-
sive fungal infections had developed in 4.1 percent of the
patients in the fluconazole group (9 of 217) and in 10.9
duces the frequency of cryptococcosis, esophageal can-
percent of those in the clotrimazole group (23 of 211; rel-
didiasis, and superficial fungal infections in HIV-infected
ative hazard, as adjusted for the CD4ϩ count, 3.3; 95 per-
patients, especially those with 50 or fewer CD4ϩ lympho-
cent confidence interval, 1.5 to 7.6). Of the 32 invasive
cytes per cubic millimeter, but the drug does not reduce
fungal infections, 17 were cryptococcosis (2 in the flucon-
overall mortality. (N Engl J Med 1995;332:700-5.)
PROPHYLAXIS against opportunistic infections is gested that this agent is also effective in preventing a
a major part of the care of patients with advanced
recurrence of oropharyngeal candidiasis.9,10 Until re-
human immunodeficiency virus (HIV) infection. Pro-
cently, the true incidence of fungal infections was un-
phylactic treatment of Pneumocystis carinii pneumonia
clear, however, and there was no reported experience
has been clearly shown to prevent initial episodes, as
with primary prophylaxis against serious fungal infec-
well as relapse, and to prolong survival.1-4 The effec-
tion. The effectiveness of fluconazole was also un-
tiveness of preventive therapy for Mycobacterium avium
known, and there was concern about its long-term tox-
infection has also been demonstrated.5 Invasive fungal
ic effects (especially hepatotoxicity), the possibility of
infections, especially with Cryptococcus neoformans, occur
drug interactions, the cost of the drug, and the poten-
in 5 to 10 percent of patients with the acquired immu-
tial for antifungal resistance to develop over time. The
nodeficiency syndrome (AIDS).6,7 In addition, mucocu-
AIDS Clinical Trials Group (ACTG) conducted a ran-
taneous candidiasis is almost ubiquitous in patients
domized, prospective clinical trial (ACTG 981) to eval-
with advanced HIV disease, and recurrent infection
uate the use of fluconazole as prophylactic therapy
against fungal infections in patients with advanced
Fluconazole is an orally active triazole antifungal
agent that is effective in preventing a relapse of cryp-tococcal meningitis.8 Several small studies have sug-
Study Design
From Washington University School of Medicine, St. Louis (W.G.P.); the Sta-
ACTG 981 compared fluconazole (200 mg per day) with clotrima-
tistical and Data Analysis Center, Harvard School of Public Health, Boston
zole troches (10 mg five times daily) for the prevention of invasive
(D.M.F., W.H.); the National Institute of Allergy and Infectious Diseases(NIAID), Bethesda, Md., and Johns Hopkins University, Baltimore (J.F.); the
fungal infections in patients with advanced HIV infection. Clotrima-
University of Cincinnati, Cincinnati (P.F.); the University of North Carolina,
zole was chosen for the control group rather than placebo in order to
Chapel Hill (C.H.); Ohio State University, Columbus (S.L.K.); Pennsylvania State
provide patients with effective local therapy for oropharyngeal can-
University College of Medicine, Hershey (M.E.E.); Case Western Reserve Uni-
didiasis and thus allow an examination of the safety and effectiveness
versity School of Medicine, Cleveland (J.C.); Duke University, Durham, N.C.
of the long-term use of fluconazole in preventing invasive fungal dis-
(H.W.); the University of Washington, Seattle (T.M.H.); Tulane University, New
ease. Eligible participants were already enrolled in ACTG 081.11
Orleans (N.H.); the University of California, San Diego, La Jolla (S.A.S., S.A.B.);
Patients were excluded from participation in ACTG 981 if they
the San Diego Veterans Affairs Medical Center, San Diego (S.A.B.); and RAND,
had a history of systemic fungal infection or allergy or intolerance to
Santa Monica, Calif. (S.A.B.). Address reprint requests to Dr. Bozzette at the SanDiego Veterans Affairs Medical Center, Mail Code 111N-1, 3350 La Jolla Village
imidazoles or azoles, if they had serum aminotransferase levels high-
er than five times the upper limit of normal or a positive serum cryp-
Supported by grants from the NIAID, the National Center for Research Re-
tococcal antigen titer at any dilution during screening, or if they were
sources, and Pfizer Central Research. Dr. Bozzette is a senior research associate
receiving maintenance therapy with systemic antifungal agents or re-
of the Department of Veterans Affairs.
quired multiagent therapy for mycobacterial infection. Patients with
*The institutions and investigators participating in the NIAID AIDS Clinical
a history of oropharyngeal, vaginal, or cutaneous candidiasis were el-
Trials Group are listed in the Appendix.
igible to participate. Patients were ineligible if they had active muco-
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on June 24, 2011. For personal use only. No other uses without permission.
Copyright 1995 Massachusetts Medical Society. All rights reserved.
FLUCONAZOLE VS. CLOTRIMAZOLE FOR FUNGAL INFECTIONS IN HIV INFECTION
sal fungal infection at the time of enrollment; however, those with
percent (10 percent vs. 2.5 percent), with a one-sided alpha level of
mucosal candida infection could receive treatment with topical anti-
0.05, in the 18-month rate of invasive fungal infections. Enrollment
fungal agents and be eligible for enrollment once they were in clinical
was later expanded so that the trial would have sufficient power to
remission. Patients with dermatophyte infections (e.g., tinea pedis)
detect a treatment difference of at least 4.5 percent (6 percent vs. 1.5
were eligible, provided cultures for candida were negative. The study
percent) in the 18-month rate of cryptococcosis. Measures were com-
design was approved by the institutional review board at each partic-
pared by a chi-square test, Fisher’s exact test, the Wilcoxon–Mann–
ipating institution; all patients gave written informed consent before
Whitney test, or Student’s t-test, as appropriate. The end points
(time to the occurrence of a fungal infection, a first episode of grade
Patients were randomly assigned to treatment with fluconazole or
3 or higher toxic effects [according to the standard ACTG grading
clotrimazole troches in a 1:1 ratio within strata defined according to
system3], treatment discontinuation, and death) were summarized as
the study center and treatment assignment in ACTG 081. Study par-
Kaplan–Meier curves and compared by a log-rank test stratified with
ticipants underwent clinical and laboratory evaluations at base line,
the use of prerandomization criteria. Multivariate regression models
every two weeks for the first month, and monthly thereafter. Cultures
were fit with the proportional-hazards model to adjust for covariates
of normally sterile body fluids and tissues, histopathological studies,
such as the CD4ϩ lymphocyte count and to derive hazard ratios with
and cryptococcal-antigen measurements were used to evaluate all ep-
isodes that suggested possible fungal infection. Prophylaxis was to becontinued until an invasive fungal infection developed, the patient
withdrew from the trial or the parent study, or the patient died. Fol-low-up evaluations were performed one month after the discontinua-
Study Population
tion of prophylaxis for patients who had invasive infection or with-drew from the study. Adherence to the study regimen was assessed
A total of 428 patients were enrolled at 29 sites from
by calculating the proportion of doses reportedly missed each month
September 1989 through September 1992; only 7 pa-
and using that value to estimate the number of days each week that
tients were enrolled after December 31, 1991. The fol-
low-up period ended on June 30, 1993. The median fol-
Patients in whom superficial mucocutaneous fungal infections de-
low-up for the entire cohort was 35 months. A total
veloped (including oral thrush but not esophageal candidiasis) wereinitially given local therapy. Nystatin suspension (10 ml of a suspen-
of 78 patients were lost to follow-up. The treatment
sion of 100,000 U per milliliter) was given four times daily for the ini-
groups were balanced with regard to the numbers of
tial treatment of thrush. For vaginal and cutaneous candidiasis, local
therapy of the investigator’s choice was used. If local therapy failed
Of the 428 patients enrolled in the study, 217 were
after a 7-day trial, patients could be treated systemically for up to30 days.
assigned to receive fluconazole and 211 to receive clo-trimazole troches. All patients are included in the anal-
End Points
ysis. The treatment groups were similar with respect to
The primary end point of the study was the time to the develop-
demographic variables and base-line laboratory values,
ment of an invasive fungal infection. Secondary end points included
with the exception of the median CD4ϩ cell count,
survival, the time to the development of a serious fungal infection
which was lower, although not significantly so, in the
(invasive fungal infections and esophageal candidiasis), and the time
fluconazole group than in the clotrimazole group (90
to the development of a superficial fungal infection. Invasive infec-
vs. 114 cells per cubic millimeter) (Table 1).
tions included cryptococcosis; the endemic mycoses, including histo-plasmosis and coccidioidomycosis; and other fungal infections withevidence of systemic invasion. Cryptococcosis was diagnosed on the
Clinical End Points
basis of a positive culture for C. neoformans or biopsy results consis-
Invasive fungal infections developed in 9 patients as-
tent with cryptococcosis and a positive titer of serum cryptococcal
signed to fluconazole and in 23 assigned to clotrima-
antigen. A diagnosis of presumed cryptococcal infection required acompatible clinical syndrome, with a positive titer of cryptococcal
zole (relative hazard, 2.6; 95 percent confidence inter-
antigen from either serum or cerebrospinal fluid. A diagnosis of
val, 1.2 to 5.6; Pϭ0.02) (Table 2). Of the 32 invasive
other invasive fungal disease was established either by culture or by
fungal infections, 17 were cryptococcosis (2 in the flu-
Candida esophagitis was diagnosed by the demonstration of tissue
invasion by candida. A presumptive diagnosis was based on the
Table 1. Base-Line Characteristics of 428 Patients with HIV In-
presence of oropharyngeal thrush and esophageal symptoms with
fection Assigned to Prophylaxis with Fluconazole or
abnormal findings on endoscopy or barium swallow, a response to
appropriate therapy, or both. Mucocutaneous candida infection wasdiagnosed on the basis of a compatible clinical syndrome and micro-
scopical evidence of candida infection (positive potassium hydroxide
preparation). A presumptive diagnosis required a compatible clinicalsyndrome and a response to specific antifungal therapy.
All end points were confirmed at each study center and subse-
quently reviewed by the protocol chairs without knowledge of specific
treatment assignments; the single disagreement was resolved by the
vote of a third member of the protocol team. Statistical Analysis P. carinii prophylaxis — no. of patients (%)
The data were analyzed on the basis of the treatment to which the
patients were randomly assigned, regardless of whether the treat-
ment was modified or discontinued during the follow-up period (in-
tention-to-treat principle). Although the study was designed to eval-
uate the one-sided null hypothesis that fluconazole was no better
than clotrimazole, more conservative two-sided P values are report-
CD4ϩ count р50 cells/mm3 — % of patients
ed. The initial target sample size of 240 was chosen to ensure that
CD4ϩ count Ͼ150 cells/mm3 — % of patients
there would be at least 80 percent power to detect a difference of 7.5
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on June 24, 2011. For personal use only. No other uses without permission.
Copyright 1995 Massachusetts Medical Society. All rights reserved.
conazole group and 15 in the clotrimazole group; rela-
tive hazard, 7.4; 95 percent confidence interval, 1.7 to
32.2; Pϭ0.004). The other invasive fungal infections
included eight cases of histoplasmosis (three in the
fluconazole group and five in the clotrimazole group),
four cases of aspergillosis (three in the fluconazole
group and one in the clotrimazole group), and one case
each of coccidioidomycosis (in the clotrimazole group),
fusarium infection (in the fluconazole group), and au-
reobasidium fungemia (in the clotrimazole group). The
estimated two-year risk of invasive fungal infection was
2.8 percent in the fluconazole group and 9.1 percent in
the clotrimazole group (difference in risk, 6.3 percent;
Pϭ0.02). After adjustment for the base-line CD4ϩ
lymphocyte count, the estimated relative hazard for in-vasive fungal infection was 3.3 (95 percent confidence
Figure 1. Relation between CD4ϩ Lymphocyte Count and the
interval, 1.5 to 7.6) and the estimated relative hazard
The top and bottom lines of the boxes represent the 75th and
for cryptococcosis was 8.5 (95 percent confidence inter-
25th percentiles, respectively, and the horizontal lines within the
val, 1.9 to 37.6) among the patients randomly assigned
boxes represent the 50th percentiles (medians); the bars above
and below the boxes represent the range of outlying values, if
The differences in treatment efficacy were most pro-
any, and the two diamonds at the top represent the two extreme
nounced among the patients with lower base-line
CD4ϩ lymphocyte counts. In the clotrimazole group,the adjusted relative hazard for invasive fungal infec-
actually occurred after the CD4ϩ count had become
tions in patients with base-line counts of 50 or fewer
CD4ϩ cells per cubic millimeter was 4.1 (95 percent
There were 20 cases of esophageal candidiasis (3 in
confidence interval, 1.3 to 13.0; Pϭ0.02), whereas the
the fluconazole group and 17 in the clotrimazole group;
adjusted relative hazard for patients with base-line
relative hazard, as adjusted for the CD4ϩ count, 5.8;
counts higher than 50 cells per cubic millimeter was 2.6
95 percent confidence interval, 1.7 to 20.0; Pϭ0.004).
(95 percent confidence interval, 0.8 to 8.1; Pϭ0.10).
Thus, there were 12 cases of serious fungal infection
Similarly, the estimated two-year cumulative risk of
(invasive disease plus esophageal candidiasis) among
cryptococcosis for patients with base-line CD4ϩ lym-
the patients assigned to fluconazole, as compared with
phocyte counts of 50 or fewer cells per cubic millimeter
40 among those assigned to clotrimazole (adjusted rel-
was 1.6 percent in the fluconazole group and 9.9 per-
ative hazard, 4.7; 95 percent confidence interval, 2.3 to
cent in the clotrimazole group (difference in risk, 8.3
percent; Pϭ0.02), as compared with 0.8 percent and
There were 46 confirmed cases of superficial fungal
4.3 percent, respectively, for patients with higher base-
infection (10 in the fluconazole group and 36 in the clo-
line counts (difference in risk, 3.5 percent; Pϭ0.04).
trimazole group) and 87 presumed cases (23 in the flu-
In addition, most patients had profound immunosup-
conazole group and 64 in the clotrimazole group) (rel-
pression by the time invasive fungal infections actually
ative hazard of a confirmed or presumed infection, 3.1;
developed; 78 percent of such infections occurred in
95 percent confidence interval, 2.2 to 4.4; PϽ0.001).
patients whose most recent CD4ϩ lymphocyte count
Oropharyngeal candidiasis accounted for most of these
was 50 or fewer cells per cubic millimeter. The base-
superficial infections. The number of episodes of con-
line CD4ϩ lymphocyte counts in patients with sub-
firmed or presumed oropharyngeal candidiasis per 100
sequent cryptococcal infection were only slightly lower
patient-years of follow-up was 5.7 for patients assigned
than the base-line counts in those who remained free
to fluconazole and 38.1 for those assigned to clotrima-
of such infection, but almost all cases of cryptococcosis
zole (PϽ0.001). An insufficient number of women were
enrolled in this study to assess theeffect of fluconazole on vaginal can-
Table 2. Relative Hazard of Fungal Infection or Death among Patients Assigned to
Fluconazole, as Compared with Those Assigned to Clotrimazole.*
Survival
assigned to fluconazole and 89 ran-domly assigned to clotrimazole died
percent confidence interval, 0.6 to1.1). After adjustment for the base-
*All analyses are stratified according to treatment assignment in ACTG 081 (i.e., according to type of prophylaxis against
P. carinii pneumonia). Values in parentheses are 95 percent confidence intervals.
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on June 24, 2011. For personal use only. No other uses without permission.
Copyright 1995 Massachusetts Medical Society. All rights reserved.
FLUCONAZOLE VS. CLOTRIMAZOLE FOR FUNGAL INFECTIONS IN HIV INFECTION
the use of a Cox proportional-hazards model, the rela-
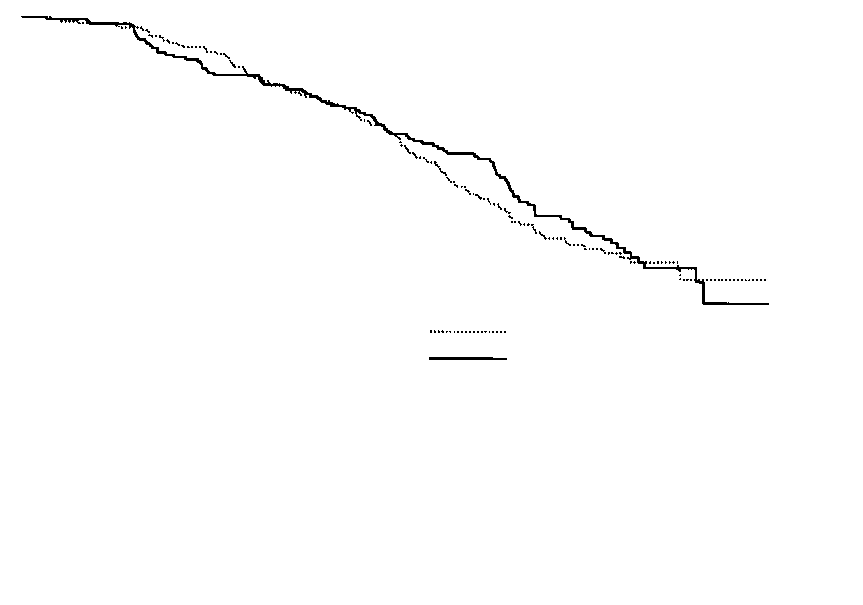
tive risk of death in the fluconazole group was 0.9 (95percent confidence interval, 0.7 to 1.3; Pϭ0.7). A total
of 102 patients in the fluconazole group and 96 in theclotrimazole group either had an invasive fungal infec-
tion or died (Pϭ0.57 by stratified log-rank test) (Fig. 2). Five patients in each group died within one month
after the diagnosis of invasive fungal infection; three of
the deaths in the fluconazole group and four of those in
the clotrimazole group were attributed to the fungal in-
fection by the site investigators. Seven of the 10 pa-
tients were infected with C. neoformans.Interaction with P. carinii Prophylaxis
Figure 2. Kaplan–Meier Estimates of the Cumulative Risk of
Fluconazole was more effective than clotrimazole in
Death or Invasive Fungal Infection among Patients Assigned to
preventing superficial fungal infections in patients as-
Receive Fluconazole or Clotrimazole Troches.
signed to trimethoprim–sulfamethoxazole, dapsone, oraerosolized pentamidine according to the protocol for
fluconazole (Pϭ0.03). In the fluconazole group, pa-
ACTG 081. The number of patients in each subgroup
tients reported adhering to the regimen for at least six
was too small to detect statistically significant differ-
days per week during 95 percent of the patient-months
ences between fluconazole and clotrimazole in the pre-
of follow-up, whereas adherence to clotrimazole for at
vention of invasive fungal disease, although there was
least six days per week occurred during only 50 percent
a consistent trend in favor of fluconazole. The observed
of patient-months (PϽ0.001). Ten patients assigned to
differences in mortality between the fluconazole and
clotrimazole (4.7 percent) reported taking systemic an-
clotrimazole groups were more pronounced among the
tifungal agents for three or more months during the
patients receiving aerosolized pentamidine (Pϭ0.17)
than among those receiving dapsone (Pϭ0.82) or tri-methoprim–sulfamethoxazole (Pϭ0.5). DISCUSSION
Invasive fungal infection is an important cause of
Toxic Effects
morbidity and mortality in patients with advanced HIV
The two treatment groups were similar with respect
disease. Disseminated cryptococcosis occurs in 5 to 10
to the rate of occurrence of most symptoms and abnor-
percent of patients with AIDS in the United States and
malities in laboratory measurements (Table 3). Site in-
is associated with a mortality rate of 10 to 20 percent.6,7
vestigators discontinued treatment in 19 patients (13 in
Histoplasmosis and coccidioidomycosis are common in
the fluconazole group and 6 in the clotrimazole group,
the endemic areas and are seen sporadically elsewhere.
Pϭ0.11) because of probable or possible drug-related
All require intensive initial therapy, typically with par-
side effects. Therapy was discontinued in three patients
enteral amphotericin B and lifelong suppressive treat-
because of rashes attributed to fluconazole. Concern
about hepatotoxicity resulted in the discontinuation of
This study clearly shows that many such infections
treatment in eight patients (six in the fluconazole group
can be prevented with 200 mg of fluconazole daily. The
and two in the clotrimazole group, Pϭ0.6); however,
estimated two-year rate of invasive fungal infections
the overall incidence of severe (grade 3 or higher) ab-normalities in the results of liver-function tests was
Table 3. Rate of Severe Abnormalities in Laboratory Measure-
Because common side effects of systemic prophylaxis
against P. carinii pneumonia could potentially obscure
the toxic effects of antifungal therapy, toxic effectswere analyzed in the subgroup of patients receiving
aerosolized pentamidine. More of the patients assigned
to fluconazole required transfusions (7.4 percent, vs.
2.8 percent in the clotrimazole group; Pϭ0.03) and
had at least one episode of severe nausea (14.1 percent,
vs. 3.9 percent in the clotrimazole group; Pϭ0.03) or
abdominal pain (18.0 percent, vs. 6.5 percent in the clo-
trimazole group; Pϭ0.03). The incidence of severe ab-
normalities in the results of liver-function tests did not
Treatment Compliance
*Severe abnormalities were those classified as grade 3 or higher on the ACTG toxicity scale.
Patients receiving clotrimazole discontinued antifun-
†Number of events per 100 person-years of follow-up.
gal medication significantly earlier than those receiving
‡ULN denotes upper limit of normal.
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on June 24, 2011. For personal use only. No other uses without permission.
Copyright 1995 Massachusetts Medical Society. All rights reserved.
was 2.8 percent in the fluconazole group and 9.1 per-
counts of 50 or fewer cells per cubic millimeter, and the
cent in the clotrimazole group. The benefit seen with
prevention of one case of invasive fungal infection
fluconazole was almost entirely due to the reduction in
required less than one third as many doses of flucona-
the risk of cryptococcosis. The incidence of other inva-
zole in this group as in the group with higher CD4ϩ
sive fungal infections was too low to determine whether
fluconazole provided effective prophylaxis against them.
In summary, fluconazole was safe, effective, and well
However, fluconazole has been found to be ineffective
tolerated as prophylaxis against superficial, serious,
against aspergillosis and may be inadequate (at the
and invasive fungal infections, especially those caused
doses used in this study) against histoplasmosis.15,16
by candida and C. neoformans. Further studies are need-
The benefit of antifungal prophylaxis was greater in pa-
ed to determine the net benefit of preventing these in-
tients with base-line CD4ϩ lymphocyte counts of 50 or
fections, the population at highest risk for them, the po-
fewer cells per cubic millimeter. The incidence of inva-
tential for the development of resistance to antifungal
sive fungal infections in the fluconazole group was quite
azoles, and the cost effectiveness of prophylaxis with
low regardless of the initial CD4ϩ count, whereas in
fluconazole as compared with careful monitoring. For
the clotrimazole group, such infections were uncom-
now, it is reasonable to consider primary prophylaxis
mon only among patients with initial counts that were
with fluconazole in patients with advanced HIV infec-
higher than 50 cells per cubic millimeter.
tion, particularly those at higher risk of fungal infec-
Superficial fungal infection due to candida species is
tion, such as patients with CD4ϩ lymphocyte counts of
ubiquitous in patients with HIV disease and causes con-
50 or fewer cells per cubic millimeter.
siderable morbidity. Our data also show that flucona-
We are indebted to Lucinda Phillips for her meticulous attention
zole is effective in the prevention of candida infections
to data management and to the many volunteers who participated in
in patients with advanced HIV disease; however, 10.6
the trial, without whom it could not have been completed.
percent of the patients assigned to fluconazole still had
at least one episode of proved or presumed candidiasis
during the study. These breakthrough infections raise
The following institutions and investigators participated in the tri-
the possibility of the development of a resistance to flu-
al: University of Cincinnati School of Medicine — J. Leonard, P. Daniel,M. White, and W. Cotton; Washington University School of Medicine —
conazole, a phenomenon that is increasingly recog-
M. Klebert, J. Voorhees, and T. Bailey; University of California, San Di-
nized in patients with advanced HIV infection and that
ego — R. Haubrich, D.D. Richman, and J. Coffman; Ohio State Uni-
has been linked to the use of fluconazole.17,18 Unfortu-
versity — R.J. Fass, M.F. Para, and C. Jackson; Johns Hopkins Univer-
nately, data on resistance are not available from this
sity School of Medicine — R.L. Becker, L. Grue III, and D.A. Wright;
Case Western Reserve University Medical School — M. Chance, M. Wal-lace, and V. Cargill; Pennsylvania State University College of Medicine —
Fluconazole was well tolerated by our patients. Seri-
M.C. Ehman and J. Zurlo; Duke University Medical Center — J.A. Bart-
ous adverse reactions were rare, and there was no seri-
lett and K. Shipp; Tulane University and Louisiana State University —
ous hepatotoxicity attributable to the drug. Gastroin-
J.A. Zachary and D. Mushett; University of Washington — A.C. Collier
testinal symptoms appear to be the most common side
and L. Corey; Harvard Medical School — C.S. Crumpacker, J.D. Allan, and D.E. Craven; Northwestern University Medical School —
effects of fluconazole. Although the trial was not spe-
R. Murphy and R. Hirschtick; Rush–Presbyterian–St. Luke’s Medical
cifically designed to evaluate mortality, we could detect
Center — C. Benson and J. Pottage; State University of New York,
no survival advantage associated with fluconazole. The
Buffalo — R. Hewitt and N. Rzepkowski; State University of New York,
lack of an effect on survival, in spite of the clear-cut
Syracuse — D.C. Blair; University of Minnesota — R. Nelson, C. Jones,and F.S. Rhame;
prophylactic effectiveness of fluconazole, a finding con-
Mt. Sinai Medical Center — D. Mildvan, A. Fox, and
C. Sanders; University of North Carolina School of Medicine — R. Whit-
sistent with the results of many other trials of prophy-
ten and B. Longmire; Indiana University Medical School — J. Craft and
laxis in HIV-infected patients,3,5,12 reflects the relatively
L.J. Wheat; University of California, San Francisco — S. Safrin, R. Mah,
low rate of mortality directly attributable to fungal in-
and R. Coleman; St. Luke’s–Roosevelt Hospital Center — M. Grieco;
Stanford University — J. Fessel, T. Merigan, and S. Kirk; University ofCalifornia, Los Angeles — M.B. Goetz and B.P. Manchester; Albert Ein-
In this study, episodes of disease attributable to can-
stein College of Medicine — R. Soeiro, G. Krienik, and J. Shilozberg;
dida and C. neoformans were six to eight times less com-
University of Massachusetts — S.H. Cheeseman, C.A. Bova, and J. Ava-
mon among the patients assigned to fluconazole than
to; Memorial Sloan-Kettering Cancer Center — D. Armstrong and
among those assigned to clotrimazole. Since the overall
M. White; Frontier Science and Technology Research Foundation, Buffalo— L. Phillips;
incidence of serious fungal infections was low, however,
Division of AIDS, NIAID — R. Hafner, M. Power, and
B. Landry; and Pfizer Central Research, Groton, Conn. — P. Robinson.
the absolute differences in the risk of these infectionswere small, and the efficiency of prescribing flucona-
REFERENCES
zole for primary prophylaxis against serious fungal in-
1. Leoung GS, Feigal DW, Montgomery AB, et al. Aerosolized pentamidine for
fection is uncertain. In fact, we estimate that 11,756
prophylaxis against Pneumocystis carinii pneumonia: the San Francisco
doses of fluconazole were given to prevent each case
community prophylaxis trial. N Engl J Med 1990;323:769-75.
2. Schneider MME, Hoepelman AIM, Eeftinck Schattenkerk JK, et al. A con-
of invasive fungal infection in the study population.
trolled trial of aerosolized pentamidine or trimethoprim–sulfamethoxazole
However, this calculation does not consider the bene-
as primary prophylaxis against Pneumocystis carinii pneumonia in patients
fit of preventing superficial fungal infections or the
with human immunodeficiency virus infection. N Engl J Med 1992;327:1836-41.
possibility of reserving therapy for subgroups at par-
3. Hardy WD, Feinberg J, Finkelstein DM, et al. A controlled trial of trimeth-
ticularly high risk. For example, the absolute and dif-
oprim–sulfamethoxazole or aerosolized pentamidine for secondary pro-
ferential risk for all fungal infections was much higher
phylaxis of Pneumocystis carinii pneumonia in patients with the acquiredimmunodeficiency syndrome: AIDS Clinical Trials Group protocol 021.
among the patients with initial CD4ϩ lymphocyte
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on June 24, 2011. For personal use only. No other uses without permission.
Copyright 1995 Massachusetts Medical Society. All rights reserved.
FLUCONAZOLE VS. CLOTRIMAZOLE FOR FUNGAL INFECTIONS IN HIV INFECTION
4. Osmond D, Charlebois E, Lang W, Shiboski S, Moss A. Changes in AIDS
12. Powderly WG, Saag MS, Cloud GA, et al. A controlled trial of fluconazole
survival time in two San Francisco cohorts of homosexual men: 1983 to
or amphotericin B to prevent relapse of cryptococcal meningitis in patients
with the acquired immunodeficiency syndrome. N Engl J Med 1992;326:
5. Nightingale SD, Cameron DW, Gordin FM, et al. Two controlled trials of
rifabutin prophylaxis against Mycobacterium avium complex infection in
13. Wheat J, Hafner RE, Wulfsohn M, et al. Prevention of relapse of histoplas-
mosis with itraconazole in patients with the acquired immunodeficiency syn-
6. Dismukes WE. Cryptococcal meningitis in patients with AIDS. J Infect Dis
drome. Ann Intern Med 1993;118:610-6.
14. Galgiani JN, Ampel NM. Coccidioidomycosis in human immunodeficiency
7. Chuck SL, Sande MA. Infections with Cryptococcus neoformans in the ac-
virus-infected patients. J Infect Dis 1990;162:1165-9.
quired immunodeficiency syndrome. N Engl J Med 1989;321:794-9.
15. Kobayashi GS, Travis SJ, Rinaldi MG, Medoff G. In vitro and in vivo activ-
8. Bozzette SA, Larsen RA, Chiu J, et al. A placebo-controlled trial of main-
ities of Sch 39304, fluconazole, and amphotericin B against Histoplasma
tenance therapy with fluconazole after treatment of cryptococcal meningitis
capsulatum. Antimicrob Agents Chemother 1990;34:524-8.
in the acquired immunodeficiency syndrome. N Engl J Med 1991;324:580-
16. Wheat LJ, Mawhinney S, Hafner R, et al. Fluconazole treatment for histo-
plasmosis in AIDS: prospective multicenter noncomparative trial. In: Pro-
9. Stevens DA, Greene SI, Lang OS. Thrush can be prevented in patients with
gram and abstracts of the 34th Interscience Conference on Antimicrobial
acquired immunodeficiency syndrome and the acquired immunodeficiency
Agents and Chemotherapy, Orlando, Fla., Oct. 4–7, 1994. Washington,
syndrome-related complex: randomized, double-blind, placebo-controlled
D.C.: American Society for Microbiology, 1994:214. abstract.
study of 100-mg oral fluconazole daily. Arch Intern Med 1991;151:2458-64.
17. Powderly WG. Resistant candidiasis. AIDS Res Hum Retroviruses 1994;10:
10. Just-Nubling G, Gentschew G, Meissner K, et al. Fluconazole prophylaxis
of recurrent oral candidiasis in HIV-positive patients. Eur J Clin Microbiol
18. Cameron ML, Schell WA, Bruch S, Bartlett JA, Waskin HA, Perfect JR.
Correlation of in vitro fluconazole resistance of Candida isolates in rela-
11. Bozzette SA, Finkelstein DM, Spector SA, et al. A randomized trial of three
tion to therapy and symptoms of individuals seropositive for human im-
antipneumocystis agents in patients with advanced human immunodeficien-
munodeficiency virus type 1. Antimicrob Agents Chemother 1993;37:
cy virus infection. N Engl J Med 1995;332:693-9.
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on June 24, 2011. For personal use only. No other uses without permission.
Copyright 1995 Massachusetts Medical Society. All rights reserved.
HBI Company Data Kft. 1911 Budapest, Corvin krt. 15. Tel: (1) 425-7433, Fax: (1) 425-7434 http://www.partnercontrol .hu/ Negatív események listája - 2010/07 Felszámolási eljárás megindítása cégadatok felszámoló 0109671038 - 24 x 36 STÚDIÓ Kft., 1029 Budapest Kútföldi u. 3. A CONT(Ó)-ROLL Kft., 1023 Budapest Árpád fejedelem útja 40-41. 0109880055 - 4dimension
IPL/Photofacial Pre-Treatment Precautions 2-4 Weeks Prior: Avoid sun exposure and/or use a sunscreen with an SPF of at least 30 and completely avoid sun exposure for 48 hrs prior to your tx. For those with darker complexions or prone to hyperpigmentation, consult with Dr Stolley regarding the use of hydroquinone prior to tx. 1 Week Prior: Stop Retin A (Tretinoin) and other vitamin A
 FLUCONAZOLE VS. CLOTRIMAZOLE FOR FUNGAL INFECTIONS IN HIV INFECTION
the use of a Cox proportional-hazards model, the rela-
tive risk of death in the fluconazole group was 0.9 (95percent confidence interval, 0.7 to 1.3; Pϭ0.7). A total
of 102 patients in the fluconazole group and 96 in theclotrimazole group either had an invasive fungal infec-
tion or died (Pϭ0.57 by stratified log-rank test) (Fig.
FLUCONAZOLE VS. CLOTRIMAZOLE FOR FUNGAL INFECTIONS IN HIV INFECTION
the use of a Cox proportional-hazards model, the rela-
tive risk of death in the fluconazole group was 0.9 (95percent confidence interval, 0.7 to 1.3; Pϭ0.7). A total
of 102 patients in the fluconazole group and 96 in theclotrimazole group either had an invasive fungal infec-
tion or died (Pϭ0.57 by stratified log-rank test) (Fig.