Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Untitled
Journal of Viral Hepatitis, 2010, 17, 459–468
Efficacy and tolerability of peginterferon alfa-2a or alfa-2b plusribavirin in the daily routine treatment of patients with chronichepatitis C in Germany: The PRACTICE Study
T. Witthoeft,1 D. Hueppe,2 C. John,3 J. Goelz,4 R. Heyne,5 B. Moeller,5 G. Teuber,6 S. Wollschlaeger,7 A. Baumgarten,8 K.-G. Simon,9 G. Moog,10 N. Dikopoulos11 and S. Mauss121Private Gastroenterological Practice, Stade; 2Centre of Gastroenterology, Herne; 3Centre of Gastroenterology, Berlin; 4Practice Centre Kaiserdamm,
Berlin; 5Centre of Gastroenterology and Hepatology, Berlin; 6Johann Wolfgang Goethe University, Frankfurt/Mai; 7Hospital Dresden Friedrichstadt,
Dresden; 8General Practice, Berlin; 9Centre of Gastroenterology, Leverkusen; 10Centre of Gastroenterology, Kassel; 11Department for Internal Medicine I,
University of Ulm, Ulm; and 12Centre for HIV and Hepatogastroenterology, Dusseldorf, Germany
Received October 2009; accepted for publication November 2009
SUMMARY. In randomized clinical trials, treatment with
59.9% of patients in Group A and 55.9% in Group B
peginterferon plus ribavirin (RBV) results in a sustained
achieved an SVR (P £ 0.051). In genotype 1-infected pa-
virological response (SVR) in around half of hepatitis C virus
tients matched by baseline parameters and cumulative RBV
genotype 1-infected and 80% of genotype 2/3-infected
dose, SVR rates were 49.6% and 43.7% for Group A and
individuals. This study aimed to evaluate efficacy and tol-
Group B, respectively (P £ 0.047); when matched by base-
erability of peginterferon alfa-2a plus RBV compared with
line parameters and RBV starting dose, SVR rates were
peginterferon alfa-2b plus RBV for the treatment of chronic
49.9% and 44.6%, respectively (P = 0.068). Overall, 21.8%
hepatitis C in routine clinical practice. The intent-to-treat
of group A and 29.6% of group B patients discontinued
cohort consisted of 3414 patients treated with either
treatment (P £ 0.0001). The efficacy and tolerability of
peginterferon alfa-2a plus RBV (Group A) or peginterferon
peginterferon plus RBV in this large cohort of patients
alfa-2b plus RBV (Group B) in 23 centres participating in the
treated in routine daily practice was similar to that in
large, multicentre, observational PRACTICE study. Collected
randomized clinical trials. In matched pairs analyses,
data included baseline characteristics, treatment regimen,
more patients achieved an SVR with peginterferon alfa-2a
RBV dose and outcome. Rates of early virological response,
compared with peginterferon alfa-2b.
end of treatment response and SVR were 76.6%, 75.7% and52.9% in Group A, and 70.2%, 65.6% and 50.5% in Group
Keywords: chronic hepatitis, HCV, PCR, pegylated interferon,
B, respectively. In patients matched by baseline parameters,
ribavirin, sustained virological response, viral load.
Hepatitis C virus (HCV) infection is a major public health
numbers of intravenous drug users and immigration from
problem, with around 170 million individuals infected
endemic areas have led to an increase in the incidence of
worldwide [1]. Up to 85% of infected individuals go on to
HCV infection in Europe over recent years [2,3]. Peginter-
develop chronic HCV (CHC) infection, with an associated risk
feron plus ribavirin (RBV) represents the gold standard
of progression to cirrhosis, end-stage liver disease and
treatment for CHC. The primary measure of treatment suc-
hepatocellular carcinoma. Despite improvements in blood
cess is sustained virological response (SVR), i.e. negative
transfusion safety and healthcare conditions, the increase in
HCV RNA 6 months after the cessation of therapy, which isassociated with a >99% chance of being virus-free 5 yearslater [4]. In large randomized controlled trials (RCTs), SVR
Abbreviations: BMI, body mass index; CHC, chronic HCV; EOT, end
was achieved by almost half of genotype 1-infected and
of treatment; EVR, early virological response; HVL, high viral load;
IDEAL, Individualized Dosing Efficacy vs. flat dosing to Assess
around 80% of genotype 2/3-infected individuals [5–7].
optimaL pegylated interferon therapy; ITT, intent to treat; LVL, low
Results from such trials form the basis of national and
viral load; RBV, ribavirin; SVR, sustained virological response.
international guidelines that provide recommendations ondosing, treatment duration and patient management [8–12].
Correspondence: Priv.-Doz. Dr. Thomas Wittho¨ft, Private Gastroen-
terological Practice Stade, Wallstrasse 38, 21682 Stade, Germany.
However patients included in RCTs are necessarily subject to
strict inclusion and exclusion criteria that may not reflect
the more complex clinical picture seen in patients in the
clinical setting compared to that seen in clinical trials. We
Ôreal-lifeÕ setting. In addition, the clinical trial situation pro-
also aimed to assess response and tolerability in patients
vides a high level of medical and support care that tends to
matched in terms of baseline characteristics and RBV dose to
maximize patient compliance. This, together with controlled
directly compare the effects of the two peginterferons.
management of side effects and dose reductions, potentiallycontributes to improved compliance that is known to influ-
ence the success of treatment [13,14]. Given these factors, itis possible that results may vary between RCT results and
PRACTICE is a retrospective study of patients with CHC
managed at 23 German gastroenterological centres with high
Two forms of peginterferon, peginterferon alfa-2a (40KD)
treatment rates (‡20 patients/year) between 2000 and 2007.
and peginterferon alfa-2b (12KD), are commercially avail-
This study investigated patients from the total PRACTICE data
able, which differ in terms of their pharmacokinetic, viral
set who had undergone treatment with either peginterferon
kinetic and tolerability profiles [15,16]. Evaluation of any
alfa-2a (40KD) (PEGASYSÒ; Roche, Welwyn Garden City, UK)
differences in efficacy between the two compounds is difficult
plus RBV (CopegusÒ; Roche, Grenzach-Wyhlen, Germany) or
because of the lack of direct comparability between clinical
peginterferon alfa-2b (12KD) (PegIntronÒ; Schering-Plough,
trials and issues around trial design in direct comparison
Bruxelles, Belgium) plus RBV (RebetolÒ; Schering-Plough). As
studies. A range of factors are known to affect response to
this study was retrospective, dosing and treatment duration
peginterferon plus RBV, including baseline characteristics
were not controlled but reflected the clinical practice of the
such as HCV genotype, viral load, age and degree of fibrosis
physician and/or treatment centre at the time the patient was
[17]. In addition, RBV dose has also been shown to affect
treated. Patient selection for submission to the database was
entirely at the clinicianÕs discretion; no restrictive parameters
[6,14,18–20]. RBV dose can be a confounding factor in
were set other than diagnosis of CHC. Data collection was
comparative trials. In the Individualized Dosing Efficacy vs.
performed via an online e-CRF. Baseline parameters included
flat dosing to Assess optimaL pegylated interferon therapy
sex, age, weight/body mass index (BMI), duration of infection,
(IDEAL) trial [21], for example, differences in RBV starting
histology at baseline, concomitant diseases, drug abuse and
dose and dose reduction regimens introduce bias that pre-
concomitant medication; virological parameters included
vents direct comparison between the two peginterferons.
HCV genotype, viral load, early virological response (EVR [‡2-
Recommended combination treatment regimens for each
log10 drop in HCV RNA and/or HCV RNA £50 IU/mL and/or
peginterferon use different RBV dosing [22,23], and there-
HCV RNA qualitatively undetectable at week 12]), end of
fore studies that use recommended regimens cannot provide
treatment response (EOT) and SVR (HCV RNA £50 IU/mL
a direct, head-to-head comparison, although they do offer
and/or HCV RNA undetectable after 24 weeks of follow-up).
comparisons between the specific combination regimens. Toovercome the bias introduced by RBV dosing regimen, a
recent Italian study gave all patients treated with eitherpeginterferon the same RBV dose based on body weight, with
The statistical analysis was descriptive to reflect the clinical
RBV dose reduction being managed identically in both
routine as intended by the clinicians. Summary statistics
groups of patients [24]. However, if the two peginterferons
(mean, median, standard deviation, 25th percentile, 75th
are to be directly compared, baseline and treatment-related
percentile, minimum, maximum, number of values) or fre-
factors must be taken into account [25].
quencies and proportions were assessed for all collected
The Pegylated Interferons and RBV: Analysis of CHC
parameters. A matched pairs population was created to
Treatment In Centres of Excellence (PRACTICE) study is a
control the variability of baseline characteristics that influ-
German nationwide retrospective, observational study anal-
ence response. A second matched pairs population was
ysing the response to hepatitis C treatment in routine clinical
created to control for baseline characteristics and RBV dose.
practice. PRACTICE includes patients treated between 2000
Analyses were calculated with SPSS for Windows Release
and 2007 in 23 gastroenterological centres with excellent
12.0.2 (Chicago, IL, USA), Testimate Version 6.4.27
treatment expertise (at least 20 CHC patients treated per year).
(Institute for Data Analysis and Study Planning, Gauting/
This retrospective study provides an important source of
Munich, Germany) and Matched Version 1.1 (Institute for
information regarding a cross section of HCV patients treated
Medical Statistics and Documentation, Erlangen, Germany).
under real-life conditions. Such patients are likely to beexposed to factors that may potentially influence outcome
which are not experienced by patients participating in highlycontrolled clinical trials. Using data from the PRACTICE
Patients were matched in pairs, one from each treatment
cohort, we aimed to evaluate the efficacy and tolerability of
group: Group A included those patients treated with
peginterferon alfa-2a plus RBV and peginterferon alfa-2b
peginterferon alfa-2a and Group B those treated with
plus RBV for the treatment of CHC patients in a Ôreal-worldÕ
Peginterferon plus RBV in routine practice
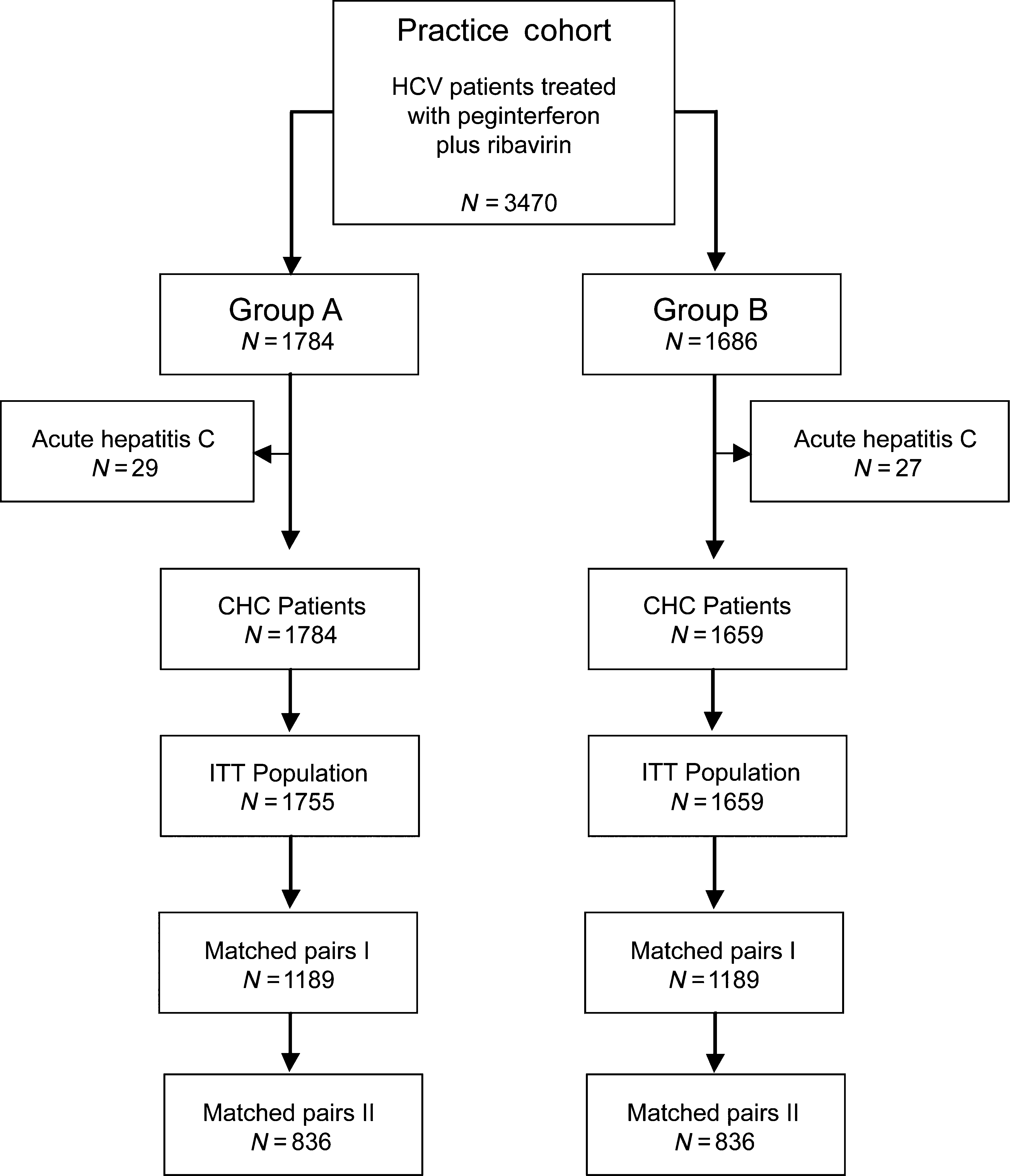
56 patients subsequently diagnosed with acute hepatitis C
To account for variations in response to peginterferon that
and not chronic hepatitis C were excluded from the analysis.
may result from baseline characteristics, patients were
The intent-to-treat population therefore consisted of 3414
matched according to the following criteria: age difference
patients: 1755 in Group A and 1659 in Group B. Patients
£3 years; HCV genotype (based on predominant infecting
were then assigned to matched pairs based on the criteria
genotype); category of viral load (low viral load or high viral
given earlier. Those patients who could not be allocated to a
load; cut-off: £400.000 IU/mL); BMI (difference £2 kg/m2);
pair were excluded from the analysis. The resulting Matched
Pairs I dataset consisted of 2378 patients (1189 from Group
RBV-combination therapy, peginterferon-RBV-combination
A and 1189 from Group B); of these 1672 (836 from each
Group) were included in the Matched Pairs II analysis.
treatment); presence of drug substitution treatment and
Groups A and B were well matched in terms baseline and
demographic data (Table 1) and in terms of concomitantmedication (Table 2). The majority of patients were treatment
naive [89.0%, intent to treat (ITT)]; 5.8% had relapsed, 4.9%
To account for the effects of variations as a result of RBV
were nonresponders and 0.3% had been both relapsers and
dose, a further analysis was performed. In addition to the
nonresponders (‡2 previous treatments). The most common
criteria of Matched Pairs I, patients were matched according
known sources of HCV infection were intravenous drug use
(35.7%, ITT analysis) and transfusion (18.0%, ITT analysis).
>100%), where 100% dose was based on that given by the
The source of infection was unknown in 33.0% of the patients.
specific RBV prescribing recommendation [22,23].
The mean duration of therapy is shown in Table 3. The
percentage of patients who received £80% cumulative doseof peginterferon and of RBV (based recommended dosing
B = 1686) included in the PRACTICE cohort who had
Virological responses to treatment in the various groups are
undergone treatment with peginterferon plus RBV were
shown in Table 5. In the ITT analysis, the rate of EVR, EOT
identified. Patient disposition is shown in Fig. 1. Among all,
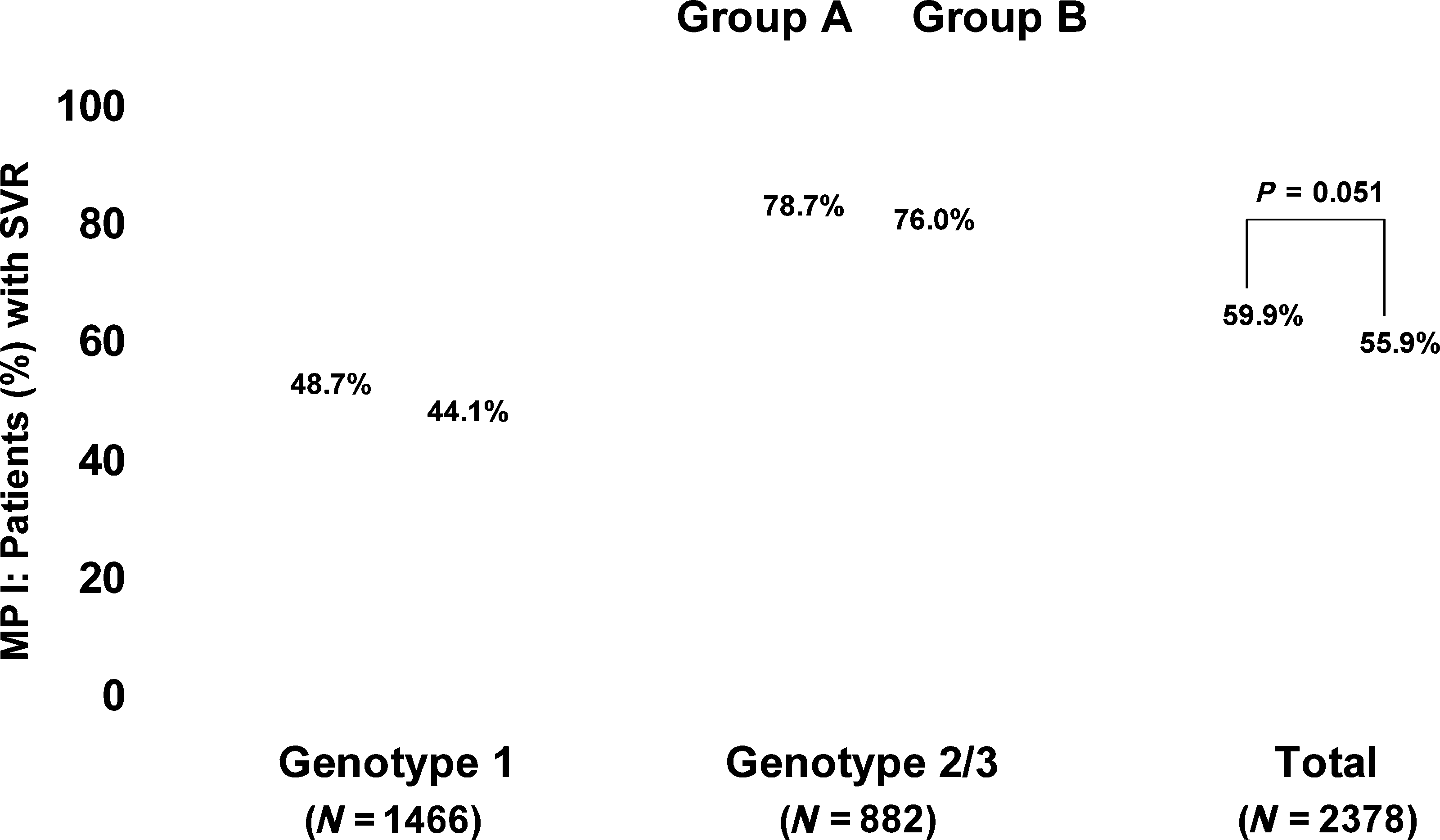
response and SVR was higher in patients in Group A com-pared with group B, although this did not reach statisticalsignificance for any measure. In the Matched Pairs I anal-ysis, the overall SVR was lower in Group B patients (55.9%)than in Group A patients (59.9%), and this differenceshowed
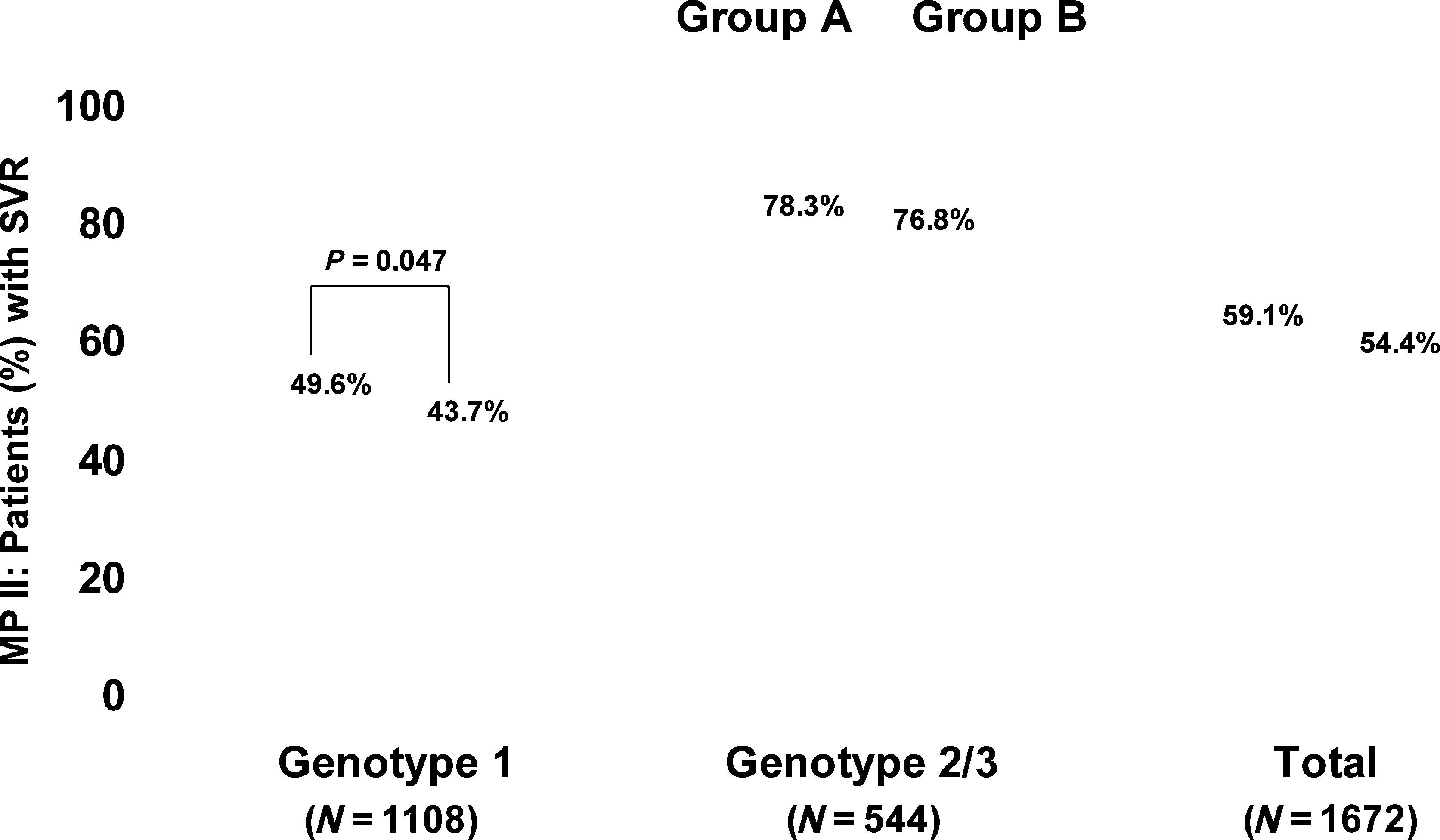
(P = 0.051; Fig. 2). There was no significant difference inSVR between Group A and Group B when analysed bygenotype (Table 5; Fig. 1). In the Matched Pairs II analysis,the overall SVR was again higher in Group A patientscompared with Group B patients (59.1% vs 54.4%, respec-tively; P = 0.054). For genotype 1-infected patients, thepercentage of patients with an SVR in Group A was signifi-cantly higher than for Group B (49.6% vs 43.7%, respec-tively; P = 0.047) (Fig. 3). There was no significantdifference for genotype 2/3-infected patients.
Rates of EVR, EOT and SVR response were lower in
patients co-infected with HIV (n = 148) compared withthose with HCV infection only. In the ITT population,29.4%, 47.4% and 34.7% of genotype 1 co-infected patientswith HIV achieved EVR, EOT response and SVR, respectively. For genotype 2/3 co-infected patients, EVR, EOT responseand SVR rates were 85.7%, 79.2% and 58.5%, respectively. SVR rates were higher in patients in Group A compared withGroup B (36.7% vs 31.6%, respectively, for genotype-1co-infected patients, and 63.0% vs 53.9%, respectively, for
ITT, intent to treat; MP, matched pairs; BMI, body mass index; HVL, high viral load (>400 000 IU/mL); LVL, low viral load(£400 000 IU/mL). *Present in >5% of overall population.
prescribing information, significantly more genotype 1-in-
Treatment discontinuations (ITT analysis)
fected patients in Group A achieved an SVR compared with
Overall, significantly fewer patients discontinued therapy
Group B. However, as the prescribed RBV starting dose and
before the EOT in Group A compared with Group B (21.8%
dose reduction regimens are different for the two different RBV
vs 29.6%; P £ 0.0001). The main reasons for withdrawal
preparations [22,23], this method may not have resulted in
were (multiple reasons were possible for each patient) viro-
matching in terms of absolute RBV dose. We therefore per-
logical nonresponse (Group A 12.7%; Group B 19.3%); poor
formed an additional analysis of genotype 1-infected patients
tolerability (Group A 4.0%; Group B 4.3%); patient request
matched by the criteria of Matched Pairs I plus initial RBV
(Group A 2.2%; Group B 3.1%) and noncompliance (Group
dose, which included the evaluation of any dose reductions
and dose reduction strategy (i.e. amount of reduction). Thepotential effect of body weight on RBV starting dose wascontrolled as patients were matched for BMI deviation
Ribavirin dose and dose adjustment – Matched Pairs III
<2 kg/m2 as per Matched Pair I criteria. In all, 579 matched
In the Matched Pair II analysis, where patients were
pairs were included in this analysis (Matched Pairs III).
matched according to cumulative RBV dose as defined by
Starting dose of RBV was 600 mg in 0.2%, 800 mg in
Peginterferon plus RBV in routine practice
ITT, intent to treat; MP, matched pairs. *In >1% of cohort.
26.4%, 1000 mg in 54.7% and 1200 mg in 18.6% of
resulted in a cure (SVR) in over half of all patients, a figure
patients in each Group. The majority of patients (90.2% in
similar to that reported in pivotal clinical trials [5–7]. Good
Group A and 87.2% in Group B) did not require RBV dose
SVR rates were achieved despite the fact the study included
reduction; 20 (3.5%) and 19 (3.3%) patients in Group A and
patients such as HIV infected patients and intravenous drug
Group B, respectively, received RBV dose reductions of
abusers who are generally considered to be less easy to treat
‡400 mg, and 31 (5.4%) and 52 (9.0%), respectively,
and would have been excluded from clinical trials. The
received RBV dose reductions of 200 mg (P = 0.1148 for
overall rates of EVR, EOT and SVR were higher in those
difference in dose reduction between groups). Average time
patients treated with peginterferon alfa-2a plus RBV com-
to first dose reduction was similar between both groups
pared with peginterferon alfa-2b plus RBV. In patients
(92.1 days in Group A and 94.5 days in Group B). In the
matched by baseline characteristics, treatment with peg-
Matched Pairs III analysis, a higher proportion of genotype
interferon alfa-2a plus RBV was associated with a higher
1-infected patients achieved SVR in Group A compared with
rate of SVR than peginterferon alfa-2b plus RBV. In addition,
Group B when matched by RBV starting dose, although this
when patients were matched in terms of RBV dose, both
did not reach statistical significance (49.9% vs 44.6%,
by starting dose and as a proportion of cumulative dose
based on prescribing information, more genotype 1-infectedpatients achieved SVR with peginterferon alfa-2a plus RBVcompared with peginterferon alfa-2b plus RBV.
Data from randomized clinical trials form the basis of
In this large open-label cohort study of patients with chronic
treatment guidelines and inform clinicians and healthcare
hepatitis C treated in clinical community settings over a
workers on individual patient management. However, clini-
period of 7 years, treatment with peginterferon plus RBV
cal trial populations by necessity are defined and restricted,and the trial process itself involves the use of clear protocols,for example, concerning dose reductions or treatment. The
support and monitoring a patient receives during a clinicaltrial is also more likely to improve compliance with treat-
ment, which is an important contributor to a successful
outcome. As such, the clinical trial situation may not fully
reflect real-life clinical practice with its more diverse, complex
patient population, variability in access and support mech-
anisms, and possibly less well-defined protocols in routine
practice. Cohort studies such as the current study aretherefore important to assess how well clinical trial data
transfer to routine practice. In the current study, 57.9%
Table 4 Patients (%) who received £80% cumulative dose of peginterferon or ribavirin (RBV) dose
of patients overall achieved an SVR: 46.5% of genotype
The current study also suggests that treatment with
1-infected patients and 77.3% of genotype 2/3-infected. This
peginterferon alfa-2a may result in a higher rate of SVR in
compares favourably with pivotal clinical trials that reported
patients treated under routine clinical conditions. For a valid
rates of 42–46% in genotype 1-infected patients and 76–82%
comparison of peginterferon regimes to be made, it is
in genotype 2/3-infected patients [5–7,26,27]. The findings
important to match patient groups not only according to
of this study are also in line with those from other retro-
baseline factors but also according to RBV dose. Genotype
spective analyses of HCV-infected patients treated in routine
and viral load are the most significant factors associated with
clinical practice where overall SVR rates of 49–66% have
SVR, but other baseline factors such as CHC treatment
been reported, with rates of 37–61% in genotype 1-infected
history, co-infection with HIV, BMI and age have also been
and around 70% of genotype 2-infected patients [28–32].
shown to influence response [17,31,35,36]. RBV dose is also
The SVR rates achieved by HIV/HCV co-infected patients in
important both to early viral decline and EVR, and to the
the current study not only were lower than those in HCV
prevention of relapse and so SVR [35]. There is evidence that
monoinfected patients as would be expected, but also
RBV dose at the start of and early in the course of treatment
compared favourably to those achieved in clinical trials
is predictive of SVR [19,20] and that maintenance of RBV
dose during therapy is also an important factor in attaining
Treatment with peginterferon plus RBV was well tolerated
SVR, particularly in genotype 1-infected patients [14,37].
in the current study. Rates of discontinuation of therapy
Interestingly, RBV has also been shown to be important to
were similar to that reported in pivotal clinical trials
SVR in recent studies of triple antiviral regimens [38] – the
(14–21%) [5–7] and were within the range reported by
so-called specifically targeted antiviral therapy for hepatitis C
other cohort studies of peginterferon plus RBV in clinical
or STAT-C – further underlining its importance in inter-
practice (11–33%) [28,31,32]. This current study therefore
feron-based treatment regimens. We found that EVR, EOT
adds to the growing volume of data demonstrating that the
and SVR rates were all higher for peginterferon alfa-2a
efficacy and tolerability of peginterferon plus RBV can be
compared with peginterferon alfa-2b, although this did not
similar in everyday clinical practice as that reported in
reach significance in the ITT analysis. Where patients were
matched by potentially confounding baseline characteristics,
EVR, early virological response; EOT, end of treatment; SVR, sustained virologicalresponse; ITT, Intent to treat; MP, Matched pairs; P values for A vs. B. Underlined P values reflect 5% level of significance: *P = 0.051; P = 0.054;àP = 0.047.
Peginterferon plus RBV in routine practice
side-effect profiles may affect adherence and so SVR. Therewas a significantly higher discontinuation rate with pegin-terferon alfa-2b compared with peginterferon alfa-2a in thecurrent study, predominantly as a result of higher virologicalnonresponse, although the rate of Ôpoor tolerabilityÕ wassimilar between groups. Consensus Guidelines for the treat-ment of CHC with peginterferon plus RBV have been avail-able since 2002 [8,9,11,12], with German guidelines beingpublished in 2004 [10]. The findings from this study suggestthat, overall, clinicians who took part in PRACTICE werelargely following guidelines in terms of treatment duration,with a mean duration of therapy of around 24 weeks for
Fig. 2 Sustained virological response in Matched Pair Ianalysis (matched by baseline factors).
genotype 2/3 patients and 40 weeks for genotype 1 patients,although the mean duration of therapy in genotype 1patients was shorter in the peginterferon alfa-2b group. Inaddition, the number of genotype 1 patients who received£80% cumulative interferon dose was higher at over 50% inthe peginterferon alfa-2b group, which may also havecontributed to poorer outcome.
Several recent trials have also reported higher SVR rates
with peginterferon alfa-2a plus RBV compared with pegin-terferon alfa-2b plus RBV. A prospective, randomized,independent Italian study, in which a standard initial doseof RBV and consistent strategies for dose reduction wereused for both peginterferons, found that more patientstreated with peginterferon alfa-2a plus RBV significantlyachieved SVR compared with those treated with peginter-
Fig. 3 Sustained virological response in Matched Pair II
feron alfa-2b plus RBV (68.7% vs 54.4%, respectively;
analysis (matched by baseline factors and cumulative
P = 0.008) [24]. The randomized open-label Milan Safety
Tolerability study also reported significantly higher SVRrates with peginterferon alfa-2a plus RBV compared with
more patients achieved an SVR with peginterferon alfa-2a
peginterferon alfa-2b plus RBV (66% vs 54%, respectively;
plus RBV compared to peginterferon alfa-2b plus RBV in a
P = 0.02) [39]. However, in the IDEAL study, SVR rates in
real-life setting, and this difference approached significance.
genotype 1-infected patients were reported to be similar
When matched by cumulative RBV dose, significantly more
between the two different peginterferons plus RBV [40]. The
genotype 1-infected patients treated with peginterferon alfa-
study reported higher EOT response with peginterferon alfa-
2a achieved an SVR. Similar results were also seen when
2a plus RBV, as was also seen in the current study, but this
patients were matched in terms of baseline characteristics
was offset by a greater relapse rate in IDEAL that resulted in
and RBV starting dose, although this did not reach signifi-
the similar rate of SVR. In a subanalysis of African Ameri-
cance, possibly as a result of the lower patient numbers in
can patients, a particularly difficult to treat population,
the Matched Pairs III analysis. As the majority of patients did
included in the IDEAL trial, although SVR rates were simi-
not require on-treatment dose reductions, and as reduction
lar, treatment with peginterferon alfa-2a plus RBV resulted
strategies appeared to be similar in those that did, it is
in higher rates of rapid virological response, EVR and EOT
unlikely that differences in RBV dose affected our findings.
response [41]. Given the importance of RBV to both early
Interestingly, in line with results from the APRICOT and
and SVR, particularly in genotype 1 patients, this effect may
RIBAVIC studies [33,34], we found a higher rate of response
be explained by the different RBV dosing and side-effect
rate in HCV/HIV co-infected patients treated with peginter-
management strategies that were used in the different
feron alfa-2a compared with those treated with peginterfer-
treatment arms of IDEAL, where RBV dose reductions of
on alfa-2b in the ITT population of this Ôreal-lifeÕ study.
200–400 mg/day were used for those patients treated with
Unfortunately, because of the small number of patients in
peginterferon alfa-2b, whereas those patients treated with
the Matched Pairs groups, it is not possible to interpret this
peginterferon alfa-2a received an RBV dose reduction of
finding further. The reasons behind the different responses
600 mg/day (as recommended in the prescribing guide-
obtained using the different peginterferons is unclear. Dif-
lines). Such differences make direct comparisons between
ferences in pharmacokinetics and viral kinetics may impact
the individual peginterferons alone impossible to make with
on virological response [15,16], while differences in
confidence from this study. In our study, initial RBV dose
and dose reduction management were at the discretion of
regimens used in daily practice in patients matched for
the treating clinician and presumably reflected current
possibly confounding baseline parameters.
treatment guidelines. However, it is interesting to note that,
In this large, multicentre study of patients treated with
in genotype 1-infected patients matched for initial RBV dose
peginterferon plus RBV over 7 years in Ôreal-worldÕ clinical
and for BMI, RBV dose reductions on-treatment were very
conditions, efficacy and tolerability were similar to that
similar between patient groups treated with peginterferon
described in industry-sponsored registration trials, despite
alfa-2a or peginterferon alfa-2b. The majority of patients
the high selection and support provided to patients enrolled
received dose reductions of 200 mg, independent of the
in such trials. When patients in this study were matched in
prescribing information that recommends reduction of
terms of baseline characteristics and according to RBV dose,
600 mg. These findings therefore suggest that differences in
both of which are known to affect the outcome of pegin-
RBV dose reduction did not contribute to the differences
terferon therapy, data suggest that more patients treated
seen in SVR and also that a more conservative RBV dose
with peginterferon alfa-2a in routine daily practice achieve
reduction strategy is employed in routine practice than is
SVR compared with peginterferon alfa-2b.
recommended in prescribing recommendations. Overall,therefore, data from our study support those of studies
which suggest that patients treated with peginterferon alfa-2a may be more likely to achieve an SVR compared with
We express our gratitude to all investigators who partici-
those who receive peginterferon alfa-2b. Further evaluation
is required to investigate possible reasons for the apparentdifferences in treatment success in the current study.
Although retrospective studies are subject to a range of
limitations compared with prospective studies, they do
Dietrich Hueppe has served as a speaker, a consultant and
provide an important source of descriptive information
an advisory board member for Roche, Essex, Gilead, Bristol-
pertaining to treatment under Ôreal-lifeÕ conditions and over
Myers Squibb and Novartis. Christine John has received an
longer time periods. In particular, they provide the oppor-
honorarium and expenses from Roche for the current study
tunity to assess whether success rates (in this case SVR)
and has received travel grants from Roche, Gilead and
obtained in clinical trials can also be obtained under real-life
Bristol-Myers Squibb. Joerg Goelz has served as a speaker for
conditions where patients are exposed to factors not
Essex, Roche, Tibotec, Gilead, Bristol-Myers Squibb, GSK,
encountered in clinical trials. The major strengths of this
Pfizer and Boehringer Ingelheim and has participated in
study include its large size and the long time period over
advisory boards for Gilead, BMS and Pfizer. Gerlinde Teuber
which data had been collected. Unlike the controlled clinical
has received speakerÕs fees from Bristol-Myers Squibb, Gilead
trial population, this study examined an unselected cross
and Essex. Sven Wollschlaeger has received speakerÕs fees
section of CHC patients treated under routine Ôreal-lifeÕ
from Roche, MSD, Schering-Plough, Bristol-Myers Squibb
conditions and therefore is more reflective of clinical prac-
and Novartis. Axel Baumgarten has served as a speaker, a
tice. The use of matched pairs of patients allows for more
consultant and an advisory board member for Roche, Tibo-
comparability between treatment groups by accounting for
tec, Bristol-Myers Squibb, GSK, Pfizer, Essex, Gilead and MSD
variation in baseline factors and RBV dose that may impact
and has research funding from Roche, Tibotec, GSK, Pfizer,
on outcome. Limitations of the study include the fact that is
Essex and Abbott for clinical study projects. Karl-Georg
not possible to completely rule out potential selection bias in
Simon has received speakerÕs fees from Roche, Astra, Essex,
different centres when assessing suitability for treatment and
Ferring and Bristol-Myers Squibb. Nektarios Dikopoulos has
in selecting treatment regimens, although the use of mat-
served as a speaker for Roche AG and has received speakerÕs
ched pairs of patients should help overcome the latter.
fees from Roche AG. Stefan Mauss has served as a speaker
Clinicians were free to decide which patients they selected for
and an advisory board member for Roche, Schering-Plough,
inclusion in the study, and data regarding any patients not
Gilead, Bristol-Myers Squibb, Novartis, GSK and Tibotec
selected for inclusion and the reasons for any such nonin-
and has received grants from Roche and Abbott. All other
clusion are not available. As with all retrospective studies,
authors have no conflicts of interest to declare.
another potential bias may be caused by missing data, as
This study was funded by Roche AG. The authors had
only data that were documented by the clinicians in the
complete access to the data that support this article. Funding
patient records were available for inclusion in the study.
for editorial support was also provided by Roche AG.
However, substantial data for the evaluation of the HCVtherapy were available for most baseline characteristics, and
the majority of patients had EVR and EOT as well as SVRdata. With regard to differences between the two treatment
1 World Health Authority. Hepatitis C Fact Sheet. 2000.
regimens, this is not a controlled head-to-head study
Available from http://www.who.int/mediacentre/factsheets/
but offers comparisons between the specific combination
fs164/en/. Accessed February 3, 2009.
Peginterferon plus RBV in routine practice
2 Esteban JI, Sauleda S, Quer J. The changing epidemiology of
18 Ferenci P, Fried MW, Shiffman ML et al. Predicting sus-
hepatitis C virus infection in Europe. J Hepatol 2008; 48:
tained virological responses in chronic hepatitis C patients
3 Rantala M, van de Laar MJ. Surveillance and epidemiology
of hepatitis B and C in Europe – a review. Euro Surveill
19 Loustaud-Ratti V, Alain S, Rousseau A et al. Ribavirin
exposure after the first dose is predictive of sustained viro-
4 Swain M, Lai M, Shiffman ML et al. Sustained virologic
logical response in chronic hepatitis C. Hepatology 2008; 47:
response resulting from treatment with peginterferon alfa-
2a alone or in combination with ribavirin is durable and
20 Maynard M, Gagnieu MC, Pradat P, Souvignet C, Trepo C.
constitutes a cure: an ongoing 5-year follow-up. Gastroen-
Prediction of sustained virological response by ribavirin
plasma concentration at week 4 during pegylated-inter-
5 Fried MW, Shiffman ML, Reddy KR et al. Peginterferon alfa-
feron/ribavirin combination therapy in HCV patients.
2a plus ribavirin for chronic hepatitis C virus infection. N
21 McHutchison J, Sulkowski M. Scientific rationale and study
6 Hadziyannis SJ, Sette Jr H, Morgan TR et al. Peginterferon-
design of the individualized dosing efficacy vs flat dosing to
alpha2a and ribavirin combination therapy in chronic
assess optimal pegylated interferon therapy (IDEAL) trial:
hepatitis C: a randomized study of treatment duration and
determining optimal dosing in patients with genotype 1
ribavirin dose. Ann Intern Med 2004; 140: 346–355.
chronic hepatitis C. J Viral Hepat 2008; 15: 475–481.
7 Manns MP, McHutchison JG, Gordon SC et al. Peginterferon
22 Rebetol (ribavirin) Summary of Product Characteristics.
alfa-2b plus ribavirin compared with interferon alfa-2b plus
Available from http://emc.medicines.org.uk/emc/assets/c/
ribavirin for initial treatment of chronic hepatitis C: a
html/DisplayDoc.asp?DocumentID=3237. Accessed Janu-
randomised trial. Lancet 2001; 358: 958–965.
8 National Institutes of Health Consensus Development Con-
23 Copegus (ribavirin) Summary of Product Characteristics.
ference Statement. Management of hepatitis C. NIH Consens
Available from http://emc.medicines.org.uk/emc/assets/c/
html/DisplayDoc.asp?DocumentID=11755. Accessed Janu-
9 Strader DB, Wright T, Thomas DL, Seeff LB. American
Association for the Study of Liver Diseases. Diagnosis,
24 Ascione A, Tartaqlione MT, Lampasi F et al. Peginterferon
management, and treatment of hepatitis C. Hepatology
Alpha-2a plus ribavirin versus peginterferon alpha-2b plus
ribavirin in naı¨ve patients with chronic hepatitis C virus
10 Zeuzem S. Standardtherapie der akuten und chronischen-
infection: results of a prospective randomised trial. J Hepatol
25 Hofmann WP, Bock H, Weber C et al. Effectiveness of an-
www.kompetenznetz-hepatitis.de/aerzteforum/standard-
tiviral therapy in patients with chronic hepatitis C treated
therapie_hep_c_zeuzem.pdf. Accessed November 30, 2008.
by private practice gastroenterologists. Z Gastroenterol 2006;
11 Yee HS, Currie SL, Darling JM, Wright TL. Management and
treatment of hepatitis C viral infection: recommendations
26 Zeuzem S, Feinman SV, Rasenack J et al. Peginterferon alfa-
from the Department of Veterans Affairs Hepatitis C
2a in patients with chronic hepatitis C. N Engl J Med 2000;
Resource Center program and the National Hepatitis C
Program office. Am J Gastroenterol 2006; 101: 2360–2378.
27 Pockros PJ, Carithers R, Desmond P et al. Efficacy and safety
12 Farrell GC. New hepatitis C guidelines for the Asia-Pacific
of two-dose regimens of peginterferon alpha-2a compared
region: APASL consensus statements on the diagnosis,
with interferon alpha-2a in chronic hepatitis C: a multi-
management and treatment of hepatitis C virus infection.
center, randomized controlled trial. Am J Gastroenterol
J Gastroenterol Hepatol 2000; 22: 607–610.
13 McHutchison JG, Manns M, Patel K et al. Adherence to
28 Wittho¨ft T, Mo¨ller B, Wiedmann KH et al. Safety, tolerability
combination therapy enhances sustained response in
and efficacy of peginterferon alpha-2a and ribavirin in
genotype1–infected patients with chronic hepatitis C. Gas-
chronic hepatitis C in clinical practice: the German Open
troenterology 2002; 123: 1061–1069.
Safety Trial. J Viral Hepat 2007; 14: 788–796.
14 Shiffman ML, Ghany MG, Morgan TR et al. Impact of
29 Gheorghe L, Iacob S, Sporea I et al. Efficacy, tolerability and
reducing peginterferon alfa–2a and ribavirin dose during
predictive factors for early and sustained virologic response
retreatment in patients with chronic hepatitis C. Gastroen-
in patients treated with weight-based dosing regimen of
PegIFN alpha-2b ribavirin in real-life healthcare setting.
15 Zeuzem S, Welsch C, Herrmann E. Pharmacokinetics of
J Gastrointestin Liver Dis 2007; 16: 23–29.
peginterferons. Semin Liver Dis 2003; 23(Suppl. 1): 23–28.
30 Sagir A, Heintges T, Akyazi Z et al. Therapy outcome in
16 Bruno R, Sacchi P, Ciappina V et al. Viral dynamics and
patients with chronic hepatitis C: role of therapy supervision
pharmacokinetics of peginterferon alpha-2a and peginter-
by expert hepatologists. J Viral Hepat 2007; 14: 633–638.
feron alpha-2b in naive patients with chronic hepatitis C: a
31 Thomson BJ, Kwong G, Ratib S et al. Response rates to
randomized, controlled study. Antivir Ther 2004; 9: 491–497.
combination therapy for chronic HCV infection in a clinical
17 Ferenci P. Predictors of response to therapy for chronic
setting and derivation of probability tables for individual
hepatitis C. Semin Liver Dis 2004; 24(Suppl. 2): 25–31.
patient management. J Viral Hepat 2008; 15: 271–278.
32 De Kaita K, Wong S, Renner E, Minuk GY. Treatment out-
genotype 1 infection treated with peginterferon alpha-2a
comes in a centralized specialty clinic for hepatitis C virus
plus ribavirin. Aliment Pharmacol Ther 2008; 28: 43–50.
are comparable with those from clinical trials. Can J Gas-
38 He´zode C, Forestier N, Dusheiko G et al. Telaprevir and
peginterferon with or without ribavirin for chronic HCV
33 Torriani FJ, Rodriguez-Torres M, Rockstroh JK et al. Pegin-
infection. N Engl J Med 2009; 360: 1839–1850.
terferon Alfa-2a plus ribavirin for chronic hepatitis C virus
39 Rumi MG, Aghemo A, Prati GM et al. Randomized study
infection in HIV-infected patients. N Engl J Med 2004; 351:
Peginterferon-alfa2b plus Ribavirin in naı¨ve patients with
34 Carrat F, Bani-Sadr F, Pol S et al. Pegylated interferon alfa-
chronic hepatitis C: final results of the Milan Safety Tol-
2b vs standard interferon alfa-2b, plus ribavirin, for chronic
erability (MIST) study. Hepatology 2008; 48: Abstract
hepatitis C in HIV-infected patients: a randomized controlled
40 McHutchison JG, Lawitz EJ, Shiffman ML et al. Peginterferon
35 Zeuzem S. Heterogeneous virologic response rates to inter-
alfa-2b or alfa-2a with ribavirin for treatment of hepatitis C
feron-based therapy in patients with chronic hepatitis C: who
infection. N Engl J Med 2009; 361: 580–593.
responds less well? Ann Intern Med 2004; 140: 370–381.
41 McCone J, Hu K, McHutchison JG et al. Sustained Virologic
36 Kau A, Vermehren J, Sarrazin C. Treatment predictors of a
Response (SVR) and Predictors of Response in African
sustained virologic response in hepatitis B and C. J Hepatol
American (AA) Patients in the IDEAL (Individualized Dosing
Efficacy Versus Flat Dosing to Assess OptimaL Pegylated
37 Bain VG, Lee SS, Peltekian K et al. Clinical trial: exposure to
Interferon Therapy) Phase 3b Study. Hepatology 2008; 48:
ribavirin predicts EVR and SVR in patients with HCV
Banco Santander Uruguay Casa central: Julio Herrera 1365, Montevideo, Uruguay CARTILLA de TARJETA DE DÉBITO Características del producto Herramienta que permite la realización de transacciones a través de los cajeros automáticos (ATM), operando sobre las cuentas que tiene el cliente en el Banco pudiendo realizar retiros, depósitos en efectivo y cheques, transferencias ent
MAGYAR NYELV ÉS IRODALOM MESTERKÉPZÉS A Miskolci Egyetem Bölcsészettudományi Kara (ME BTK) magyar szakos képzéseinek megtervezésekor alapvetően két tényezőt vettünk figyelembe: a hagyományos magyar szakos képzés jellegének megtartását, illetve az újabban jelentkező regionális és országos foglalkoztatási igényeket. A bölcsészek elhelyezkedési lehetőségeiről, esély
 Peginterferon plus RBV in routine practice
56 patients subsequently diagnosed with acute hepatitis C
To account for variations in response to peginterferon that
and not chronic hepatitis C were excluded from the analysis.
Peginterferon plus RBV in routine practice
56 patients subsequently diagnosed with acute hepatitis C
To account for variations in response to peginterferon that
and not chronic hepatitis C were excluded from the analysis.
 Peginterferon plus RBV in routine practice
side-effect profiles may affect adherence and so SVR. Therewas a significantly higher discontinuation rate with pegin-terferon alfa-2b compared with peginterferon alfa-2a in thecurrent study, predominantly as a result of higher virologicalnonresponse, although the rate of Ôpoor tolerabilityÕ wassimilar between groups. Consensus Guidelines for the treat-ment of CHC with peginterferon plus RBV have been avail-able since 2002 [8,9,11,12], with German guidelines beingpublished in 2004 [10]. The findings from this study suggestthat, overall, clinicians who took part in PRACTICE werelargely following guidelines in terms of treatment duration,with a mean duration of therapy of around 24 weeks for
Fig. 2 Sustained virological response in Matched Pair Ianalysis (matched by baseline factors).
Peginterferon plus RBV in routine practice
side-effect profiles may affect adherence and so SVR. Therewas a significantly higher discontinuation rate with pegin-terferon alfa-2b compared with peginterferon alfa-2a in thecurrent study, predominantly as a result of higher virologicalnonresponse, although the rate of Ôpoor tolerabilityÕ wassimilar between groups. Consensus Guidelines for the treat-ment of CHC with peginterferon plus RBV have been avail-able since 2002 [8,9,11,12], with German guidelines beingpublished in 2004 [10]. The findings from this study suggestthat, overall, clinicians who took part in PRACTICE werelargely following guidelines in terms of treatment duration,with a mean duration of therapy of around 24 weeks for
Fig. 2 Sustained virological response in Matched Pair Ianalysis (matched by baseline factors).