Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Bjpcn-cardiovascular.com
TherapeuticsReview Optimising treatment of type 2 diabetes with metformin There is good evidence that tight glycaemic control significantly improves outcomes in patients with type 2 diabetes. All practice nurses will be looking to achieve the new General Medical Services contract (GMS2) targets for HbA reduction in diabetes (see box). Practices will be developing prescribing strategies to achieve this reduction, in accordance with good clinical practice. Metformin offers an important first-line therapy for type 2 diabetes. The introduction of a new, sustained-release Dr Mike Mead formulation – Glucophage SR – should improve patient compliance with General Practitioner, Forest House Medical Centre, Leicester metformin and so improve glycaemic control. Starting therapy with metformin 26% lower risk of a diabetes-related end renal impairment. Check a patient’s renal When initiating therapy for patients with point. Metformin was also associated with function before starting metformin and type 2 diabetes, the first drug to consider a 29% lower risk of all-cause mortality don’t use the drug if their creatinine is is metformin – for four good reasons: compared with sulphonylureas or insulin. No significant effect on diabetes-related HbA targets in GMS2 1. Metformin increases insulin sensitivity mortality was found with sulphonylureas and targeting insulin resistance reduces or insulin. Cardiovascular disease cardiovascular risk in patients with type 2 accounted for 62% of deaths in the dietary diabetes. Insulin resistance encompasses arm of this trial and compared with diet, dyslipidaemia (raised triglycerides, low metformin gave a 39% reduction in HDL–cholesterol, raised small dense myocardial infarction. Metformin has, LDL–cholesterol) and hypertension, as well therefore, clearly proven benefits in as the hyperglycaemic component of reducing mortality and cardiovascular type 2 diabetes. disease in patients with type 2 diabetes. >130 mmol/L. Metformin needs to be 2. The United Kingdom Prospective 3. NICE guidance has recommended that stopped 48 hours before use of iodine- Diabetes Study (UKPDS) showed that metformin should be used as the first-line containing X-ray contrast media and metformin was at least as effective as glucose-lowering therapy in patients 48 hours before surgery requiring general sulphonylureas or insulin in controlling whose blood glucose is inadequately anaesthesia. blood glucose and was associated with a controlled with lifestyle intervention. More precisely, it recommended Potential problems with standard metformin for those with a BMI metformin therapy >25 kg/m2 with a ‘consideration’ There are two main problems with for patients who are not standard metformin therapy. First, the overweight – this is conservative dosing schedule, which requires a twice- as metformin works as well in daily or three times daily regimen, patients with normal weight and potentially making good compliance is a perfectly valid option in such difficult for patients. Second, the side- patients. effects that can occur with metformin. The main side-effects that may limit 4. Compared with sulphonylureas, compliance are gastrointestinal, including metformin has less potential for diarrhoea, vomiting, nausea, anorexia, weight gain and has a much lower abdominal pain and a metallic taste. risk of hypoglycaemia. This message is getting through, Non-adherence to metformin therapy is a as currently nearly three-quarters serious problem in practice and one that of all newly diagnosed patients we need to address in order to achieve with type 2 diabetes receive good glycaemic control and reach our metformin as first-line therapy. targets. One trial – the DART study – found adequate adherence in only one-third Precautions when starting (34%) of patients prescribed metformin. metformin
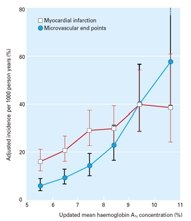
Incidence of myocardial infarction (heart attack) and microvascular
There are well-known Introduction of Glucophage SR
complications (eg eye problems) by updated mean haemoglobin A1c
contraindications before starting A new sustained-release formulation of
concentration, for white men aged 50–54 years at diagnosis and with meanduration of diabetes of 10 years. UKPDS Group. metformin, including severe heart metformin – Glucophage SR – is given failure, hepatic impairment and once-daily in the evening, with food to delay gastric emptying. Previous research has shown that a once-daily regimen of an extended-release oral hypoglycaemic can Optimising glycaemic give better compliance (and glycaemic control with metformin information control) than a twice-daily immediate- release version of the same drug. Glucophage SR has comparable efficacy in lowering HbA to standard metformin and is as effective as metformin twice or three times daily. Apart from the convenience of
34). Lancet 1998; 352: 854–865. a once-daily dose, Glucophage SR has a much lower incidence of gastrointestinal
NICE Inherited Clinical Guideline G. side-effects (including 50% lower incidence of diarrhoea) than standard metformin, potentially encouraging compliance with the drug and allowing us to titrate to a higher dose without the patient discontinuing their therapy. This means that patients who are inadequately controlled due to poor tolerability of metformin (including those only managing to take the lower doses) can be switched
diabetes: a retrospective cohort study. to the new modified-release preparation to Diabetic Medicine 2002; 19: 279–284. restore and improve their HbA control. Conclusion Metformin is now central to the therapy of patients with type 2 diabetes and every effort should be made to improve compliance with the drug, particularly if
release formulation. Clin Ther 2003;
we are to reach the targets for HbA 25: 515–529. new GMS contract.
Meaning of p-value in Medical Research Corresponding Author: Dr. Brijesh Sathian, Assistant Professor & Managing and Chief Editor NJE, Community Medicine, Manipal College of Medical Sciences, Department of Community Medicine, Manipal College of Medical Sciences, 155 - Nepal Submitting Author: Dr. Brijesh Sathian, Assistant Professor & Managing and Chief Editor NJE, Community
Thalassemia and Pulmonary Hypertension individuals, it is important that patients undergo annual screening If I have PAH, what should I do to improve my overall health? There are several things you can do to improve your health if youhave PAH. These include:Keep your weight at a healthy level. Adopt a healthy diet that is high in fruits and vegetables and What is pulmonary hypertension?

 TherapeuticsReview
TherapeuticsReview