Le sildénafil présent dans Kamagra exerce une inhibition réversible de la PDE5, modulant la cascade GMPc et favorisant une vasodilatation localisée. L’absorption digestive varie selon la forme utilisée, comprimés classiques ou gels oraux. La distribution tissulaire est large et la liaison protéique élevée, avoisinant 96 %. La métabolisation hépatique génère un métabolite actif contribuant à l’effet pharmacologique global. La demi-vie reste courte, avec disparition plasmatique en quelques heures. Les interactions significatives concernent surtout les nitrés organiques et inhibiteurs puissants du CYP3A4. Dans les publications techniques, kamagra en ligne est souvent cité dans le cadre d’analyses comparatives portant sur les différences de formulations et de cinétique d’absorption.
Untitled
Histomorphometric Evaluation of Extraction Sockets and Deficient Alveolar Ridges Treated with Allograft and Barrier Membrane: A Pilot Study Hyman Smukler, BDS, DMD, HDD*/Luca Landi, DDS**/Reza Setayesh, DMD, DMSc***
The aim of the study was to determine the fate of demineralized freeze-dried bone allograft (DFDBA)used in conjunction with a barrier membrane in the management of extraction sockets and deficientalveolar ridges, and to compare the amount of bone formed with that found in untreated sites. Tenbiopsies were obtained from 8 grafted patients. Five biopsies were harvested from untreated sites dur-ing routine implant placement and analyzed for comparison. In the socket management procedure,DFDBA was packed tightly into the socket and covered with an expanded polytetrafluoroethylene (e-PTFE) membrane. Primary closure was achieved in all cases. In the ridge regeneration procedure, corti-cal columns were placed in the ridge projecting outward approximately 3 mm to create and maintainspace for DFDBA particles packed between them; the columns were then covered by an e-PTFE mem-brane. Healing time ranged from 8 to 23 months. At the time of implant placement, bone cores (7 mmϫ 2 mm) were harvested, fixed in 10% formalin solution, and prepared for histologic examination. Atthe light microscopic level, no inflammation or fibrous encapsulation was observed. New bone forma-tion on and around DFDBA particles was widespread. Histomorphometric analysis of the grafted speci-mens and untreated sites was carried out using the trabecular bone volume (TBV) index. The TBV in themaxillary test specimens was 55.03%, as compared to 57.33% of control cores. Unaltered DFDBAmade up 8.7% of the test specimens. In the mandibular biopsies, the TBV was 56.6%, while for thecontrols it was 40.9%. The volume of DFDBA still present was 2.45%. The results tended to indicatethat treatment with DFDBA in conjunction with cell occlusive membranes will result in new bone for-mation, predominantly by the process of conduction, which appears to be similar in amount andnature to that found in cores harvested from healed nonfunctional edentulous areas. (INT J ORAL MAXILLOFAC IMPLANTS 1999;14:407–416)
Key words: deficient ridges, demineralized freeze-dried bone allograft, extraction sockets, guided bone regeneration, histomorphometry, osteoconduction
According to Amler et al,1 uncomplicated heal- events, beginning with clot formation and culmi-
ing of human extraction sockets takes place in
nating in a bone-filled socket with a connective tis-
approximately 40 days in an organized sequence of
sue and epithelial tissue covering. However, diseaseof periodontic and endodontic origin or surgicaltrauma can adversely affect this normal pattern andresult in extraction sites that have healed but have
***Professor, Boston University School of Dental Medicine,
Department of Periodontology and Oral Biology, Boston,
alveolar ridges that are quantitatively deficient.
These deformed alveolar ridges do not permit
***Periodontal Resident, Boston University School of Dental
appropriate pontic fabrication when conventional
Medicine, Department of Periodontology and Oral Biology,
fixed prostheses are contemplated; nor do they per-
Boston, Massachusetts; and Private Practice, Grosseto, Italy.
mit the placement of endosseous implants when
***Associate Professor, Boston University School of Dental
Medicine, Department of Periodontology and Oral Biology,
this form of tooth replacement is being considered.
Defective ridge formation can be prevented bygrafting the deficient or vulnerable sockets at the
Reprint requests: Dr Hyman Smukler, Boston University School
time of tooth loss to ensure the formation of alveo-
of Dental Medicine, Department of Periodontology and OralBiology, 100 East Newton Street, Boston, MA 02118.
lar bone within the sites,2,3 and deficient alveolar
ridges can be augmented or regenerated.4–7
COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTINGOF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
The International Journal of Oral & Maxillofacial Implants
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-
OUT WRITTEN PERMISSION FROM THE PUBLISHER. Smukler et al
Requirements for successful alveolar regenera-
There is a paucity of human histologic and his-
tion were first presented by Melcher and Dreyer in
tomorphometric data pertaining to the amounts of
1962.8 Later, Nyman and coworkers9 proposed
new bone formed in extraction sockets and on
guidelines for guided tissue regeneration in the
deficient alveolar ridges augmented with DFDBA
repair of defects associated with teeth and edentu-
particles and barrier membranes. This study was
lous ridges.10 These included creation and mainte-
undertaken to evaluate the potential of this type of
nance of space; protection of the blood clot
treatment to produce new bone in these situations.
formed; trephining of cortical plates to enhance the
An additional aim was to compare the amounts of
ingress of vascular, cellular, and molecular elements
newly formed bone with that found in untreated
needed in the regenerative process; and the use of a
cell occlusive barrier membrane to prevent inva-sion of the site by tissues that could impede regen-
Materials and Methods
eration. These criteria have since been successfullyapplied in endeavors to generate bone in extraction
Patient Selection. Six patients, all requiring
sockets2,3 and to regenerate alveolar bone in defec-
extraction of 1 or more teeth for traumatic or
tive ridges.4,5,6,11 Human demineralized freeze-
endodontic reasons (these were to be replaced by
dried bone allografts (DFDBA) have been used in
endosseous implants), were included in the socket
conjunction with the principles of guided bone
treatment portion of the study. Two patients
regeneration to reconstitute and maintain bone
requiring ridge augmentation procedures prior to
during the placement of endosseous implants.6,12–18
implant placement participated in this part of the
In these instances, DFDBA has been considered a
study, while 5 patients requiring routine endosse-
space maintaining device and osteopromotive, and
ous implant placement provided cores for the
new bone formation takes place predominantly by
untreated areas (Table 1). The patients, 4 males
a process of osteoconduction.3,16,18 The role of
and 4 females ranging in age from 30 to 65 years
DFDBA as an osteoinductive element has been
(mean 58.33), were all treated in Department of
both questioned19–24 and affirmed.2,25–27
Periodontology and Oral Biology Implant Center
COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING
408 Volume 14, Number 3, 1999
OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-
OUT WRITTEN PERMISSION FROM THE PUBLISHER. Smukler et al
at Boston University School of Dental Medicine.
ing the membranes from the soft tissue and under-
All patients were in good health as determined by
lying bone. Primary closure of the wounds was
medical history screening, had no contraindica-
obtained using suturing methods previously
tions to treatment, exhibited good oral hygiene,
described. Those membranes that were retained
and were informed of the nature of this investiga-
until implant placement were removed in the same
tion. All gave their informed consent according to
manner at the time of stage 2 surgery (Fig 3).
the guidelines of the Internal Review Board, which
Ridge Regeneration. Appropriate local anesthesia
was administered, and a distal-to-mesial incision
Surgical Technique. Socket Management. Fol-
was made on the crest of the edentulous ridge
lowing administration of appropriate local anes-
between the teeth adjacent to the edentulous space,
thesia, intrasulcular incisions were made around
from the mesiolingual line angle of the distal tooth
the teeth to be extracted. Vertical releasing inci-
to the distolingual line angle of the mesial tooth.
sions were made both palatally and facially, either
Vertical releasing incisions were made at the distal
at the mesial and distal line angles of teeth adjacent
line angle of the distal and the mesial line angle of
to the tooth being removed or one tooth distal and
the mesial adjacent teeth, both buccally and lin-
mesial to it, and mucoperiosteal flaps were care-
gually, and carried around the teeth to join the cre-
fully elevated. The tooth in question was atraumat-
stal incision. Mucoperiosteal flaps were elevated,
ically extracted and the socket was thoroughly
and the buccal alveolar surface was penetrated in
debrided (Fig 1). Intramarrow penetration with a
multiple areas to expose the endosseum. Wider
fine, round bur promoted appropriate bleeding.
holes, approximately 2 ϫ 2 mm (Fig 4a), were
Commercially obtained DFDBA (American Red
drilled to receive the specially prepared DFDBA cor-
Cross, St. Louis, MO) of 250 to 350 µm particle
tical columns (Northwest Tissue Center, Seattle,
size was hydrated with sterile normal saline for 30
WA), which, after being firmly placed in these holes,
minutes prior to placement within the sockets. The
projected out laterally approximately 3 mm like tent
DFDBA was placed in the socket and compressed
poles (Fig 4b) to support the e-PTFE membrane to
using saline-saturated gauze, from which all excess
be placed over the site.7 Particulate DFDBA with
saline had been expressed, and firm pressure from
the same properties as that used in the socket treat-
a hand instrument to eliminate dead spaces within
ment part of the study was similarly reconstituted
the graft material. This was repeated until the
and compressed onto the surface of the alveolar
socket was slightly overfilled (Fig 2).
bone around and between the cortical columns (Fig
A nonresorbable expanded polytetrafluoroeth-
4c). The membrane was then suitably trimmed,
using the same precautions as previously described,
Flagstaff, AZ) of appropriate dimension was
and adapted well to sound bone surrounding the
trimmed so that it extended approximately 3 mm
augmentation site. The buccal flaps were further
over the socket onto sound bone buccolingually
released via periosteal separation to permit primary
but did not engage adjacent tooth surfaces. The
closure of the wounds without undue tension, and
buccal flaps were further released by periosteal
the flaps were sutured with e-PTFE vertical mattress
separation to permit coronal positioning of the tis-
alternating with interrupted sutures. Postoperative
sues and primary closure. Suturing was accom-
medications and membrane removal were the same
plished with nonresorbable e-PTFE, vertical mat-
tress, and interrupted sutures. The patients were
Core Harvesting. At the time of implant place-
placed on doxycycline 100 mg/day for 2 weeks
ment, which varied between 8 and 23 months after
and nonsteroidal anti-inflammatory medication for
grafting, the patients received appropriate local
pain control for 5 days, and chlorhexidine glu-
infiltration anesthesia and mucoperiosteal flaps
conate mouthwash (twice daily) was prescribed
were elevated. Utilizing the photographic records
until mechanical plaque control could be recom-
made at each surgical stage as a frame of reference,
menced after 1 week. Sutures were removed after 1
the center of each augmented extraction site was
week and the patients were seen weekly to monitor
compared to the original, in an attempt to ensure
that the core would be taken from the treated site.
Membranes were kept in place for a minimum
The use of templates would have been more accu-
of 5 weeks; they were removed at the time of
rate, but since the study did not include measure-
implant placement if they had not already become
ment of the ridges, templates were not used. As the
exposed and been removed. The membranes were
first step in osteotomy site preparation, a 2-mm
removed following administration of local anesthe-
surgical trephine was used to remove a 7-mm-long
sia by elevating mucoperiosteal flaps and separat-
bone core from the center of the regenerated site.
COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTINGOF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
The International Journal of Oral & Maxillofacial Implants
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-
OUT WRITTEN PERMISSION FROM THE PUBLISHER. Smukler et al Fig 3 At stage 2 surgery, the e-PTFE
site. Note the fracture of thin, vulnerable
ridge, with holes trephined in the buccal
plate. Some of the holes will have corti-
extraction site. The width of the ridgehas been maintained.
COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING
410 Volume 14, Number 3, 1999
OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-
OUT WRITTEN PERMISSION FROM THE PUBLISHER. Smukler et al
This was immediately fixed in 10% formaldehyde;
maturely and were removed at 5 weeks. Socket
site preparation was then completed, the selected
treatment and ridge augmentation both resulted in
implants were placed (Fig 5), and the wounds were
ridges of adequate dimension for implant place-
closed with vertical and interrupted sutures.
ment. Microscopic examination of the extraction
Sutures were removed in 7 days; healing generally
site cores did not reveal any inflammatory
progressed uneventfully. The same modus operandi
response or fibrous encapsulation of particulate
was utilized when cores were obtained in the ridge
bone. Very little osteoclastic activity was noted
augmentation part of the study. Similarly, the cores
around the remaining nonvital DFDBA particles;
from healed, untreated sites were procured at the
rather, those particles still present were sur-
rounded by and appeared to be coalesced with
Histologic Preparation. Following fixation, the
newly formed bone (Fig 6a). Osteoblastic activity
cores were decalcified in nitric acid for 2 weeks.
was observed to still be occurring on some newly
The bone specimens were embedded in paraffin;
formed bone surfaces, indicating a persisting
cut serially, in a longitudinal plane, to a thickness
remodeling process (Fig 6b). The newly formed
of 6 to 8 µm; and stained with hematoxylin and
bone was woven, woven undergoing lamellation,
eosin and toluidine blue in preparation for micro-
or lamellar with secondary osteons being present
scopic evaluation. Only the 6 central sections
in the mineral phase (Fig 7a). In some sections,
obtained from each core were used for compara-
basophilic staining material was noted, sometimes
tive study. This selection was made in an attempt
eccentrically placed in lacunae, within the DFDBA
to minimize the inclusion of artifacts related to the
particles near their peripheries and adjacent to
harvesting process, which were more likely to
newly formed bone (Fig 7b). This material
appear on the surfaces of the cores. In addition, it
appeared to resemble the eccentrically placed
was assumed that these sections would be more
nuclei within newly formed vital bone.
The cores from the untreated, healed sites
Histomorphometric Analysis. The 2 most cen-
exhibited the trabecular bone pattern typically
tral sections of each core were evaluated histomor-
seen in alveolar bone, with large marrow spaces
phometrically by the same person, who was
filled with adipose-type tissue usually seen at
blinded. The microscopic slides were viewed on a
maturity (Fig 8). The experimental histologic sec-
Nikon FXA microscope with a digital analytic
tions seemed to reveal a more compact picture,
interface (MicroVideo Instruments, Avon, MA)
with new bone formation on and about the endur-
The microscope was attached to a video camera,
which was linked to a computer, the software used
appeared to be smaller and scarcer; some con-
being Image Pro+ (North Reading, MA). The
tained a mature adipose cellular arrangement,
amounts of bone, marrow, and DFDBA particles
while others exhibited an apparently more active
within a given field were measured and expressed
in pixels. The average number of fields for each
section analyzed was 5.53 (SD 2.67). The magnifi-
revealed essentially the same picture. The cortical
cation used was 200 ϫ. The trabecular bone vol-
columns were still recognizable histologically.
ume (TBV) index28 was used to establish the ratio
They appeared to be virtually unchanged, with
between trabecular bone and marrow spaces.
only early signs of cellular activity seen in isolated
Photographic Data Collection. At strategic times
areas. Newly formed bone was present and in inti-
during the treatment, 1-to-1 35-mm photographs
mate contact with the surfaces of the cortical
were taken to permit evaluation of clinical results
and to help ensure that cores were always taken
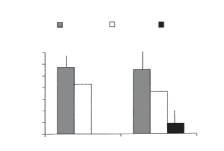
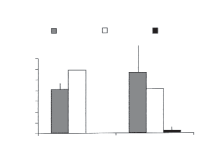
Histomorphometrically, the TBV for the maxil-
from the center of a regenerated site (Figs 1, 4a, and
lary test cores was 55.03% (SD = 15.02), while
5). Reference to pretreatment photographs permit-
that for maxillary untreated sites was 57.33% (SD
ted verification of ridge width maintenance in the
= 11.37) (Fig 11, Table 2). In the mandible, the
treated sites. Measurements were not made, as this
TBV for the experimental areas was 56.60% (SD
= 32.77) and 40.95% (SD = 2.76) for theuntreated areas (Fig 12, Table 3). The DFDBA
still present in the specimens was 8.7% (SD =7.58) for the maxillary and 2.45% (SD = 1.04) for
Primary closure was achieved in all surgical proce-
dures, the postoperative period being generallyuneventful. Two membranes became exposed pre-
COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTINGOF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
The International Journal of Oral & Maxillofacial Implants
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-
OUT WRITTEN PERMISSION FROM THE PUBLISHER. Smukler et al
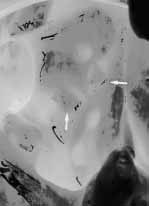
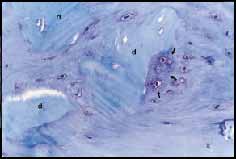
Photomicrograph demonstrating a large amount of new
High-power view (ϫ400) of outlined area in Fig 6a,
bone (nb) formation surrounding DFDBA particles (d) in a 21-
rotated 90 degrees counterclockwise. Note DFDBA particles (d)
month postoperative maxillary extraction site specimen (tolui-
surrounded and coalesced with new bone. Note cellular activ-
dine blue stain, original magnification ϫ200).
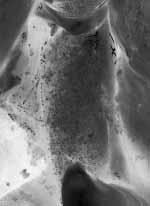
Photomicrograph representing newly formed bone of
High-power view of area outlined in Fig 7a. Note
woven and lamellar nature in a mandibular ridge augmentation
woven and lamellar bone, primary osteons, and occurrence of
at 8 months (hematoxylin and eosin, original magnification
what could be nuclei in DFDBA particle (arrows) (hematoxylin
and eosin, original magnification ϫ400).
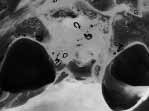
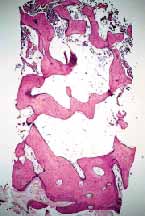
core from a nonfunctional, untreatededentulous maxillary area. Compare therelative amounts of bone and marrowspace sizes with those in Fig 9 (hema-toxylin and eosin, original magnification
mm core from a treated maxillary socketsite after 9 months of healing. Note thedenser appearance, scarcer and smallermarrow spaces, as compared to Fig 8(hematoxylin and eosin, original magnifi-cation ϫ40).
COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING
412 Volume 14, Number 3, 1999
OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-
OUT WRITTEN PERMISSION FROM THE PUBLISHER. Smukler et al
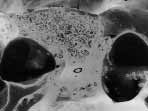
Photomicrograph illustrating a cortical column (cc)
surrounded by newly formed bone (nb) in an 8-monthmandibular ridge augmentation. The asterisk (*) indicates whatcould be an osteocyte surrounded by bone in the otherwiseunaltered cortical column (hematoxylin and eosin, originalmagnification ϫ400).
Bar graph comparing the TBV in test and untreated
Bar graph comparing the TBV in test and untreated
COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTINGOF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
The International Journal of Oral & Maxillofacial Implants
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-
OUT WRITTEN PERMISSION FROM THE PUBLISHER. Smukler et al Discussion
genic” tissues from “undemineralized” allogeneicbone implants, Urist et al30 described some
The present study appears to confirm that
basophilic staining elements in some of the osteo-
DFDBA can be used to successfully treat sockets
cyte lacunae. These elements may merely be a fea-
ture of nonvital bone implants. Urist et al30 also
implants.2,3,16,18 It also corroborates the findings
stated that all the treated and untreated allogeneic
that utilization of particulate DFDBA, in conjunc-
or autogenous implants used in their study exhib-
tion with the principles of guided tissue regenera-
ited empty lacunae within the same period after
tion for the treatment of extraction sockets, will
implantation. In addition, Urist in 198031 again
result in the gradual replacement of the allograft
stated that lacunae of implanted decalcified allo-
by newly formed bone.3,18 The finding that bone
grafts were predominantly empty and may remain
formation takes place in an appositional manner
so for extended periods of time. The findings of
on and around the allograft particles verifies the
empty lacunae in the remaining allograft particles
findings of others and tends to substantiate a con-
in the present study tend to agree with this.
ductive role for the DFDBA particles.3,7,17,18 The
The observation that the experimental cores
fact that osteoblastic activity was still occurring
presented a more compact picture than the cores
on the surfaces of the newly formed lamellar bone
from the untreated healed areas is probably merely
indicates that active remodeling of the DFDBA
an aggregation of the new bone formation on and
particles and bone formation continued to take
around the remaining DFDBA particles and the
place for up to 23 months in this study, a phe-
sparser and smaller number of marrow spaces.
nomenon also noted by others.3,17,18 It is note-
Whether this phenomenon would persist as the
worthy that Simion et al18 were still able to iden-
grafts mature or whether the new bone would
tify, in human peri-implant tissue, apparently
come to more closely resemble bone found in the
unaltered DFDBA particles some 4 years after
untreated sites still needs to be determined.
placement. In more apical portions of the same
The histomorphometric analysis revealed that
specimen, DFDBA particles could be seen com-
the TBV for the maxillary cores was 55.03% in the
pletely embedded in bone matrix and still show-
experimental sites and 57.33% in the untreated
ing signs of ongoing mineralization. This would
sites. Similarly, the mean TBV for mandibular
appear to indicate that allograft reconstitution or
experimental cores and cores from untreated sites
replacement may take many years to complete.
was 56.60% and 40.95%, respectively. It is appar-
It was not possible to corroborate the presence
ent that the amount of bone present in grafted
of mineralization nodules within the DFDBA parti-
areas is similar to that found in nongrafted, non-
cles.16 However, the occasional appearance of
functional edentulous ridge sites. The percentage of
deeply stained basophilic material in osteocyte
DFDBA particles still present in the maxillary test
lacunae, in the most peripheral portions of the
specimens was 8.70%, as opposed to 2.45% in
demineralized particles nearest to adjacent new
mandibular specimens. This difference may be the
bone formation, which may be osteocyte nuclei,
result of a more rapid reconstitution of the DFDBA
was noteworthy. This may permit the assumption
particles in the mandible, or there may also be indi-
that some sort of ongoing creeping substitution of
vidual biologic variations in response to allograft
the graft with new bone may be occurring.
placement. The small sample size does not permit a
How these events take place would be difficult
to explain, but as Zhang et al29 suggest, they may
The standard deviations for the maxillary test
be related to the stimulating effect of residual cal-
and untreated specimens were large (15.02 and
cium levels in allografts, or the degradation of
11.37, respectively), but in the mandible the even
organic matrix (collagen/proteoglycan), which may
larger SD for the experimental core (32.77) was
diffuse from the implant-stimulating cellular
much greater than that of the untreated areas (SD =
chemotaxis into the implant. Zhang et al further
1.25). It is noteworthy that among the 4 mandibu-
suggest that the degraded matrix could also act as
lar test specimens, 1 of the 2 sides with exposed
a site to which cells attach and receive appropriate
membrane became infected, resulting in very poor
regulatory signals. Growth factor release may also
bone formation (14.0%). If this site is excluded
be involved in cellular infiltration, differentiation,
from the analysis, the TBV for the mandibular test
and establishment of a matrix that facilitates
cores would be 70.80% (SD = 20.03), suggesting
appropriate cell infiltration. However, it should be
an even more marked difference from the untreated
noted that in an investigation of chemical and
sites. The large differences seen in both control and
“autodigestive” methods to remove “alloanti-
experimental data for most parameters examined
COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING
414 Volume 14, Number 3, 1999
OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-
OUT WRITTEN PERMISSION FROM THE PUBLISHER. Smukler et al
could well be a reflection of the small sample size
Conclusions
or perhaps indicate a biologic variation that is com-mon in nonfunctioning alveolar bone.
Based on the findings and within the limits of this
The value of DFDBA as an additive in bone
histologic and histomorphometric study, it may be
regeneration procedures has also been questioned
by Becker et al.19,24,32 The same authors claim thatDFDBA has no inductive effect in promoting bone
1. In human extraction sockets, commercially
formation in human extraction sockets, which
available DFDBA, in conjunction with cell
they found healed, with nonvital bone particles
occlusive barrier membranes, appears to play a
being surrounded by connective tissue. Sockets
positive conductive role in new bone formation.
treated with autologous bone grafts, on the other
2. Histomorphometric analysis indicates similar
hand, exhibited healing with vital woven bone.
trabecular bone volume in untreated sites and
Other studies20–23 agree with these findings. Stud-
extraction sockets grafted with DFDBA, when
ies that investigated the properties of particulate
guided bone regeneration principles are fol-
human allografts have demonstrated, in ectopic
lowed. The same applies to edentulous ridges
sites or when gaps in bone are bridged, that the
allografts do exhibit inductive properties.26,27
3. The new bone growth appears to be apposi-
Zhang et al,33 in investigating the osteoconductiv-
tional, and the DFDBA particles appear to
undergo a creeping reconstitution that may take
implanted into ectopic sites in athymic mice, more
many months, if not years, to complete.
recently confirmed an inductive role for human
4. These results do not offer conclusive evidence
particulate allograft. None of these studies used
regarding the osteoinductive capacity of com-
the principles of guided tissue regeneration, where
mercially available particulate bone allografts.
cell occlusive membranes are used in conjunctionwith allograft placement as a basis for treatment. The effect of this approach on induction needs to
Acknowledgments
In addition, Schwartz and coworkers34 have
The authors are indebted to Mr Tony Chin for the preparation
shown that human particulate allografts obtained
of the histology and to Dr Dana T. Graves for use of equipmentfor the histomorphometric analysis.
from different bone banks vary in biologic activitywhen placed in ectopic sites. This variation has
References
been attributed to the age of donors, the methodof sterilization used, irradiation, and residual acid
01. Amler MH, Johnson PL, Saman I. Histological and histo-
content. What effect, if any, these factors played in
chemical investigation of human alveolar socket healing in
the studies cited is not known. In an in vitro inves-
undisturbed extraction wounds. J Am Dent Assoc 1960;
tigation comparing the biologic activity of fresh
bone and allografts, Shigeyama and coworkers35
02. Nevins M, Mellonig JT. Enhancement of the damaged
edentulous ridge to receive dental implants. A combination
were able to show biologic activity for the allo-
of allograft and Gore-Tex membrane. Int J Periodontics
graft material, which was only slightly inferior to
that of the fresh bone. It is thus obvious that more
03. Brugnami F, Then PR, Moroi H, Leone CW. Histologic
information is necessary to more definitively
evaluation of human extraction sockets treated with de-
resolve the controversy over the inductive capacity
mineralized freeze-dried bone allograft (DFDBA) and cellocclusive membrane. J Periodontol 1996;67:821–825.
of DFDBA. The present limited study did not shed
04. Buser D, Brägger U, Lang NP, Nyman S. Regeneration and
light on the inductive capacity of DFDBA, but it
enlargement of jaw bone using guided tissue regeneration.
did seem to indicate a conductive role for the allo-
Clin Oral Implants Res 1990;1:22–32.
graft material, as evidenced by the appositional
05. Dahlin C, Gottlow J, Lindhe A, Nyman S. Healing of max-
bone formation on and around the DFDBA parti-
illary and mandibular bone defects using a membrane tech-nique. An experimental study in monkeys. Scand J Plast
cles. Therefore, it may be possible to conclude
Reconstr Surg Hand Surg 1990;24:13–19.
that, irrespective of the inductive potential of
06. Jovanovic SA, Nevins M. Bone formation utilizing titanium
human allografts, the endogenous inductors,
reinforced barrier membranes. Int J Periodontics Restora-
together with the conductive effect of DFDBA and
utilization of principles of guided tissue regenera-
07. Smukler H, Barbosa E, Burliss C. A new approach to
regeneration of surgically reduced alveolar ridges in dogs:
tion, are sufficient to promote appositional bone
A clinical and histologic study. Int J Oral Maxillofac
growth in the treatment of extraction sockets and
COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTINGOF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
The International Journal of Oral & Maxillofacial Implants
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-
OUT WRITTEN PERMISSION FROM THE PUBLISHER. Smukler et al
08. Melcher AH, Dreyer CJ. Protection of the blood clot in
22. Pinholt EM, Haanaes HR, Roeerik M, Bang G. Alveolar
healing circumscribed bone defects. J Bone Joint Surg
ridge augmentation by osteoinductive materials in goats.
Scand J Dent Res 1992;100:361–365.
09. Nyman S, Lindhe J, Karring T, Rylander H. New attach-
23. Pinholt EM, Haanaes HR, Roeerik M, Bang G. Titanium
ment following surgical treatment of human periodontal
implant insertion into dog alveolar ridges augmented by
disease. J Clin Periodontol 1982;9:290–294.
allogeneic material. Clin Oral Implants Res 1994;5:
10. Nyman S, Lang NP, Buser D, Brägger U. Bone regeneration
adjacent to titanium implants using guided tissue regenera-
24. Becker W, Becker BE, Caffesse RG. A comparison of de-
tion. A report of two cases. Int J Oral Maxillofac Implants
mineralized freeze-dried bone and autologous bone to
induce bone formation in human extraction sockets. J Peri-
11. Schenk RK, Buser D, Hardwick WR, Dahlin C. Healing
patterns of bone regeneration in membrane protected
25. Reddi AH. Biologic principles of bone induction. Orthop
defects. A histologic study in the canine mandible. Int J
Oral Maxillofac Implants 1994;9:13–29.
26. Gepstein R, Weiss RE, Saba K, Hallel T. Bridging large
12. Shanaman RH. The use of guided tissue regeneration to
bone defects in bone by demineralized bone matrix in the
facilitate ideal prosthetic placement of implants. Int J Peri-
form of powder. A radiographic, histological and radioiso-
odontics Restorative Dent 1992;12:257–268.
tope-uptake study in rats. J Bone Joint Surg [Am] 1987;69:
13. Werbitt MJ, Goldberg PV. The immediate implant: Bone
preservation and bone regeneration. Int J Periodontics
27. Kubler N, Reuther J, Kirchner T, Pressnitz B, Sebald W.
Osteoinductive, morphologic and biomechanical properties
14. Gelb DA, Lazzara R. Hierarchy of objectives in implant
of autolyzed, antigen-extracted, allogeneic human bone. J
placement to maximize esthetics: Use of preangulated abut-
Oral Maxillofac Surg 1993;51:1346–1357.
ment. Int J Periodontics Restorative Dent 1993;13:
28. Parfitt AM, Drezner MK, Glorieux FH, Kanis JA, Mal-
luche H. Meunier PJ, et al. Bone histomorphometry: Stan-
15. Mellonig TJ, Triplett RG. Guided bone regeneration and
dardization of nomenclature, symbols and units. J Bone
endosseous implants. Int J Periodontics Restorative Dent
29. Zhang M, Powers RM Jr, Wolfinbarger L Jr. Effect(s) of the
16. Simion M, Dahlin C, Trisi P, Piattelli A. Qualitative and
demineralization process on the osteoconductivity of de-
quantitative comparative study of different filling materials
mineralized bone matrix. J Periodontol 1997;68:
used in bone tissue regeneration: A controlled clinical
study. Int J Periodontics Restorative Dent 1994;14:
30. Urist MR, Mikulski A, Boyd SD. A chemosterilized anti-
gen-extracted autodigested alloimplant for bone banks.
17. Landsberg CJ, Grosskopf A, Weinreb M. Clinical and bio-
logic observations of demineralized freeze-dried bone allo-
31. Urist MR. Bone transplants and implants. In: Urist MR
grafts in augmentation procedures around dental implants.
(ed). Fundamentals of Clinical Bone Physiology. Philadel-
Int J Oral Maxillofac Implants 1994;9:586–592.
phia and Toronto: Lippincott, 1980:331–368.
18. Simion M, Trisi P, Piattelli A. GBR with an e-PTFE mem-
32. Becker W, Schenk RK, Higuchi K, Lekholm U, Becker BE.
brane associated with DFDBA: Histologic and histochemi-
Variations in bone regeneration adjacent to implants aug-
cal analysis in a human implant retrieved after 4 years of
mented with barrier membranes alone or with demineral-
loading. Int J Periodontics Restorative Dent 1996;16:
ized freeze-dried bone or autologous grafts. A study in
dogs. Int J Oral Maxillofac Implants 1995;10:143–145.
19. Becker W, Urist MR, Tucker LM, Becker BE, Ochsenbein
33. Zhang M, Powers RM Jr, Wolfinbarger L Jr. A quantitative
C. Human demineralized freeze-dried bone induced inade-
assessment of osteoinductivity of human demineralized
quate bone formation in athymic mice. A preliminary
bone matrix. J Periodontol 1997;68:1076–1084.
report. J Periodontol 1995;66:822–828.
34. Schwartz Z, Mellonig TJ, Carnes DL Jr, De la Fontaine J,
20. Aspenberg P, Kalebo P, Albrektsson A. Rapid bone healing
Cochran DL, Dean DD, Boyan BD. Ability of commercial
delayed by bone matrix implantation. Int J Oral Maxillo-
demineralized freeze-dried bone allograft to induce new
bone formation. J Periodontol 1996;67:918–926.
21. Aspenberg P, Lohmander LILS, Thorngren KG. Failure of
35. Shigeyama Y, D’Errico JA, Stone R, Somerman MJ. Com-
bone induction by bone matrix in adult monkey. J Bone
mercially prepared allograft material has biological activity
Joint Surg [Br] 1988(a);70:625–627.
in vitro. J Periodontol 1995;66:478–487.
COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING
416 Volume 14, Number 3, 1999
OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-
OUT WRITTEN PERMISSION FROM THE PUBLISHER.
New Contraceptives and Other Advances in Reproductive Health Emergency Contraception Plan B and Preven are two emergency contraceptive pill products (also called “dedicated products”)currently available to women with a doctor’s prescription. While the ingredients in these productsdiffer, both Plan B and Preven should be taken within 72 hours of unprotected intercourse. Thesooner t
Drug resistance of Mycobacterium tuberculosis in patients with new pulmonary tuberculosis in Lviv/UA T. Bodmer1 , M. Pavljuk2, O. Zargaryan2, L. Rak2, U. Bischler3, and J.-P. Zellweger4 1University of Berne, Institute for Infectious Diseases, Berne, Switzerland; 2Lviv Regional Phtisio-Pulmonological Treatment and Diagnostic Centre, Sykhiv, Ukraine; 3Bear and Lion, Berne, Switzerland;



 Smukler et al
Smukler et al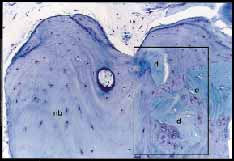



 Smukler et al
Smukler et al
 Smukler et al
Smukler et al